Gynecomastia features
Reading File
Finding Sources
Searching PubMed
gynecomastia
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of gynecomastia features:
Gynecomastia
Definition
Enlargement of the male breast glandular tissue resulting from excess estrogen action, usually due to an increased estrogen/androgen ratio. True gynecomastia involves glandular tissue >4 cm in diameter, often tender, and should be distinguished from pseudogynecomastia (excess adipose tissue/lipomastia).
- Glandular tissue = firmer, contains fibrous-like cords
- Adipose tissue = softer, diffuse
Physiologic Phases (Normal Occurrence)
| Phase | Mechanism |
|---|---|
| Neonatal | Transplacental transfer of maternal/placental estrogens |
| Pubertal (ages 12–15) | High estrogen-to-androgen ratio in early puberty; often unilateral |
| Senescent (men 50–70) | Age-related testosterone decline + increased aromatase activity in adipose tissue; usually bilateral |
Prevalence increases with age and BMI (adipose tissue aromatase activity).
Pathophysiology
Core mechanism: ↑ estrogen / ↓ androgen ratio
Estrogen Excess
- Gonadal tumors: Leydig cell tumors, Sertoli cell tumors (isolated or in Peutz-Jeghers / Carney complex), granulosa-theca cell tumors
- hCG-secreting tumors: Testicular germ cell tumors (choriocarcinoma, seminoma, embryonal carcinoma) — stimulate Leydig cell estrogen synthesis
- Non-testicular tumors: Adrenal cortical neoplasms, lung carcinoma, hepatocellular carcinoma
- Liver disease: Cirrhosis impairs estrogen catabolism → androstenedione shunted to aromatase at peripheral sites
- Hyperthyroidism: Elevated SHBG → increased free estradiol/free testosterone ratio
- Obesity: Increased aromatization of androgen precursors to estrogens
- Inherited aromatase excess (CYP19 mutation/chromosomal rearrangement): Pre-pubertal/peripubertal gynecomastia, advanced bone age, short stature, hypogonadotropic hypogonadism
Androgen Deficiency
- Primary testicular failure: Klinefelter syndrome (47,XXY) — classic association; also Reifenstein syndrome, Rosewater-Gwinup-Hamwi syndrome, Kallmann syndrome
- Secondary testicular failure: Trauma, orchitis, cryptorchidism
- Androgen insensitivity disorders
- Androgen deprivation therapy (GnRH analogues ± AR blockers for prostate cancer): causes painful breast enlargement
- Renal failure (any cause)
- Refeeding gynecomastia: Resumption of pituitary gonadotropin secretion after pituitary shutdown following starvation/malnourishment
Drug-Induced Causes
| Mechanism | Drugs |
|---|---|
| Direct estrogenic activity | Oral contraceptives, phytoestrogens, digitalis, anabolic steroids |
| Inhibit androgen synthesis | GnRH agonists, ketoconazole |
| Inhibit androgen action (AR blocker) | Spironolactone, enzalutamide, bicalutamide, cimetidine |
| Enhance estrogen synthesis | hCG |
| Uncertain mechanism | Imatinib, antiretroviral drugs (HIV), phenytoin, alcohol, marijuana, heroin |
Histopathology (Robbins)
- Subareolar button-like enlargement, unilateral or bilateral
- Microscopically: dense collagenous connective tissue + epithelial hyperplasia of duct lining
- Lobule formation almost never seen (distinguishes from female breast hypertrophy)
Grading (Schwartz's Surgery)
| Grade | Features |
|---|---|
| I | Mild enlargement, no skin redundancy |
| IIa | Moderate enlargement, no skin redundancy |
| IIb | Moderate enlargement with skin redundancy |
| III | Marked enlargement with skin redundancy and ptosis |
Clinical Features
- Subareolar, disc-like, rubbery or firm mass — often tender
- May be unilateral or bilateral
- Nipple retraction, skin dimpling, or hard/fixed tissue → red flags for malignancy
- In Klinefelter syndrome: small testes, azoospermia, hypergonadotropic hypogonadism — increased risk of male breast cancer
Evaluation
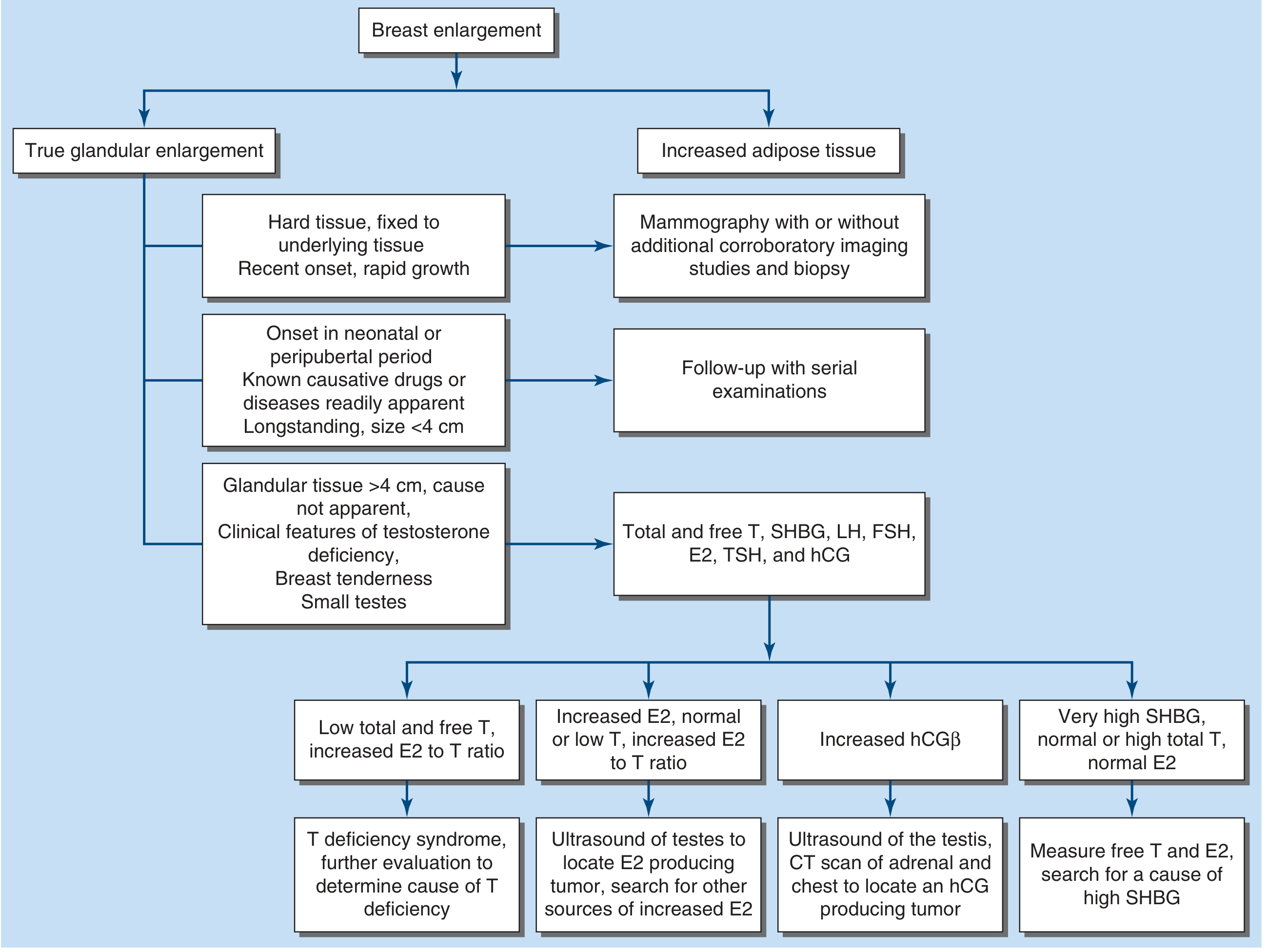
Workup for glandular tissue >4 cm with unclear cause:
- Total/free testosterone, SHBG, LH, FSH, E2 (17β-estradiol), TSH, β-hCG
- Markedly elevated E2 + suppressed LH → search for estrogen-secreting testicular/adrenal tumor
- Elevated hCG → testicular USS + CT chest/abdomen for hCG-producing tumor
- Very small testes → karyotype to exclude Klinefelter syndrome
- Liver function tests
Treatment
| Scenario | Management |
|---|---|
| Cause identified and corrected early | Breast tissue usually regresses over months |
| Long-standing gynecomastia | Surgery most effective |
| Painful gynecomastia (medical) | Tamoxifen 20 mg/day — reduces pain and size in >50%; raloxifene also used |
| Early proliferative phase | Aromatase inhibitors (anastrozole) — effective early; not better than placebo for established gynecomastia |
| Prostate cancer + ADT | Tamoxifen for prevention and treatment of breast enlargement/pain |
| Indications for surgery | Severe psychological distress, continued growth, failure of medical therapy, suspected malignancy |
Cancer Risk
- The relative risk of breast cancer is increased in men with gynecomastia, but the absolute risk remains small.
- Klinefelter syndrome carries a meaningfully higher breast cancer risk than gynecomastia from other causes.
Sources: Harrison's Principles of Internal Medicine 22E, p. 3159–3160; Robbins, Cotran & Kumar Pathologic Basis of Disease; Schwartz's Principles of Surgery 11E
Female mei hai
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.