Hi
How to simplified microbiology
Microbiology Simplified
The Big Picture
| Type | Has Nucleus? | Cell Wall? | Treatment |
|---|---|---|---|
| Bacteria | No (prokaryote) | Yes | Antibiotics |
| Viruses | No nucleus - just DNA/RNA | No cell wall | Antivirals / Vaccines |
| Fungi | Yes (eukaryote) | Yes (ergosterol) | Antifungals |
| Parasites | Yes (eukaryote) | No | Antiparasitics |
1. Bacteria - The Most Tested
Step 1: Gram Stain (First thing you do)
| Gram Positive (Purple) | Gram Negative (Pink/Red) |
|---|---|
| Thick peptidoglycan wall | Thin wall + outer membrane (LPS) |
| Staphylococcus, Streptococcus | E. coli, Klebsiella, Pseudomonas |
| Listeria, Clostridium, Bacillus | Neisseria, Haemophilus, Salmonella |
Memory trick: Gram Positive = Purple
Step 2: Shape
- Cocci (round) - e.g., Staph, Strep, Neisseria
- Bacilli (rods) - e.g., E. coli, Klebsiella, Listeria
- Spirochetes (spiral) - e.g., Syphilis (Treponema), Lyme (Borrelia)
Step 3: Key Clinical Bugs
| Bug | Disease | Clue |
|---|---|---|
| S. aureus | Skin infections, pneumonia, food poisoning | "Clusters," golden colonies |
| S. pyogenes (Group A) | Strep throat, rheumatic fever | ASO titer rises |
| S. pneumoniae | Pneumonia, meningitis, otitis | Lancet-shaped diplococci |
| E. coli | UTI, neonatal meningitis | Most common UTI bug |
| N. meningitidis | Meningitis, septicemia | Petechial rash, diplococci |
| M. tuberculosis | TB | Acid-fast, caseating granuloma |
| C. difficile | Pseudomembranous colitis | After antibiotics |
2. Viruses - Think DNA vs RNA
DNA Viruses (memorize these)
- Herpes (HSV, VZV, CMV, EBV, HHV-8)
- Hepatitis B
- Adenovirus
- Papillomavirus (HPV)
- Poxvirus
- Parvovirus (single-stranded, exception)
RNA Viruses (most common)
- Influenza - segmented RNA, antigenic shift/drift
- HIV - retrovirus (RNA -> DNA via reverse transcriptase)
- Hepatitis C - flavivirus, blood-borne
- Measles, Mumps, Rubella - paramyxoviruses/togavirus
- Rabies - rhabdovirus, bullet-shaped, from animal bites
- Rotavirus - #1 cause of diarrhea in children
Key Viral Concepts
- Latency: Herpes viruses stay dormant and reactivate (stress, immunosuppression)
- Enveloped vs. Non-enveloped: Enveloped viruses are killed by alcohol/soap; non-enveloped (like Norovirus) are harder to destroy
- Oncogenic viruses: HPV (cervical cancer), EBV (Burkitt's lymphoma), HBV/HCV (hepatocellular carcinoma)
3. Fungi - Think Immunocompromised
| Fungi | Disease | Who gets it? |
|---|---|---|
| Candida | Thrush, UTI, systemic | Diabetics, antibiotic use, HIV |
| Aspergillus | Pulmonary aspergillosis | Neutropenic patients |
| Cryptococcus | Meningitis | HIV (CD4 < 100) |
| Pneumocystis jirovecii | PCP pneumonia | HIV (CD4 < 200) |
| Histoplasma | "Histo" lung disease | Ohio/Mississippi River Valley, bat caves |
| Coccidioides | Valley fever | Southwest US, California |
Key rule: If patient is immunocompromised + lung/brain infection = think fungus
4. Parasites - Group by Type
Protozoa (single-celled)
| Parasite | Disease | Transmission |
|---|---|---|
| Plasmodium | Malaria | Mosquito (Anopheles) |
| Toxoplasma | Toxoplasmosis | Cat feces, undercooked meat |
| Giardia | Watery diarrhea | Contaminated water |
| Entamoeba | Amoebic dysentery | Fecal-oral |
| Trichomonas | STI (vaginitis) | Sexual contact |
| Leishmania | Leishmaniasis | Sandfly |
| Trypanosoma | Sleeping sickness / Chagas | Tsetse fly / Reduviid bug |
Helminths (worms)
- Roundworms (Nematodes): Ascaris, Pinworm, Hookworm, Strongyloides
- Tapeworms (Cestodes): Taenia (pork/beef), Echinococcus (liver cysts)
- Flukes (Trematodes): Schistosoma (swimmer's itch), Clonorchis (liver fluke)
Quick Study Framework
- What type? (Bacteria / Virus / Fungus / Parasite)
- How is it transmitted? (Droplet, contact, fecal-oral, vector, sexual)
- What does it cause? (Key clinical presentation)
- How do you diagnose it? (Gram stain, culture, PCR, serology, antigen test)
- How do you treat it? (Antibiotic class, antiviral, antifungal)
Antibiotic Classes - Simplified
| Class | Covers | Examples |
|---|---|---|
| Penicillins | Gram+ mainly | Amoxicillin, Piperacillin |
| Cephalosporins | Gram+/-, broader with generations | Cefazolin (1st), Ceftriaxone (3rd) |
| Fluoroquinolones | Gram- urinary/respiratory | Ciprofloxacin, Levofloxacin |
| Macrolides | Atypicals (Mycoplasma, Chlamydia) | Azithromycin |
| Vancomycin | MRSA, resistant Gram+ | IV use only (mostly) |
| Metronidazole | Anaerobes, protozoa | C. diff, Giardia, Trichomonas |
| Aminoglycosides | Serious Gram- infections | Gentamicin, Tobramycin |
Top Tips for Exams
- Always ask: "Is the patient immunocompromised?" - changes everything
- Encapsulated bacteria (S. pneumo, H. flu, N. meningitidis, Klebsiella, Salmonella typhi, B. anthracis, Cryptococcus) - at risk in asplenic patients
- Atypical pneumonias (Mycoplasma, Chlamydia, Legionella) - don't respond to penicillin, treat with macrolides/doxycycline
- HACEK organisms - gram-negative, infective endocarditis
- Spore-forming bacteria: Bacillus anthracis, Clostridium species, (and Coxiella)

Make it simplified
⚡ TOXIC SHOCK SYNDROME (TSS) - Simplified
Types at a Glance
| Menstrual | Non-Menstrual | |
|---|---|---|
| Cause | High-absorbency tampons | S. pyogenes OR S. aureus infection |
| Toxin | TSST-1 | Erythrogenic toxin, TSST-1, Enterotoxins B/C (rare) |
Simple rule: Tampons = TSST-1 only. Outside tampons = more toxin options.
How it Works (Superantigen Mechanism - Simple)
Diagnosis & Treatment
- Step 1: Symptomatic (fluids, supportive care)
- Step 2: Antibiotics
| Bug | Drug |
|---|---|
| MSSA | Nafcillin / Oxacillin / Cloxacillin |
| MRSA | Vancomycin |
| Streptococcal TSS | Penicillin + Clindamycin |
Clindamycin is added in Strep TSS because it blocks toxin production (protein synthesis inhibitor)
🦠 OTHER STAPHYLOCOCCAL DISEASES - Simplified
Memory Map: Where does Staph go?
1. Skin & Soft Tissue
| Infection | What it is |
|---|---|
| Folliculitis | Hair follicle infection |
| Furuncle (Boil) | Deep follicle abscess |
| Carbuncle | Multiple boils merged |
| Stye | Eyelid follicle infection |
| Impetigo | Bullous (blistering) type = Staph |
| Botryomycosis | Chronic granulomatous skin infection |
| Surgical site infection | Post-op wound infection |
2. Musculoskeletal
- Osteomyelitis (bone infection)
- Septic arthritis + Bursitis
- Tropical pyomyositis (muscle abscess)
Staph = #1 cause of ALL three above
3. Respiratory
- Pharyngitis, Otitis media, Sinusitis
- Community-acquired pneumonia (CAP)
- Hospital-acquired + Ventilator-associated pneumonia
- Pneumonia in Cystic Fibrosis (important exam point!)
4. Endocarditis
| Type | Staph causes... |
|---|---|
| IE (Infective Endocarditis) | #1 cause, especially in IV drug users |
| NVE (Native Valve Endocarditis) | #1 cause |
| PVE (Prosthetic Valve Endocarditis) | Early PVE = Staph (late PVE = Strep) |
One-Line Staph Summary
S. aureus = skin + bone + heart + lung infections + toxin-mediated diseases (TSS, Scalded Skin, Food poisoning)
Quick Recall Table
| System | Staph Disease | Key Point |
|---|---|---|
| Skin | Folliculitis, Boil, Impetigo | Bullous impetigo = Staph |
| Bone | Osteomyelitis | #1 cause overall |
| Heart | IE, NVE, early PVE | IV drug users! |
| Lung | CAP, HAP, VAP | Cystic fibrosis too |
| Systemic | TSS | Superantigen mechanism |
Mention reference.. Based on which book.. You give all answer
📚 References - Sources Used
Primary Microbiology Textbooks
1. Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Edition
- ISBN: 9781260012026
- Covers: TSST-1 mechanism, Staphylococcal toxins, Streptococcal pyrogenic exotoxins, TSS definition
- Relevant section: "Toxic Shock Syndrome Toxin" and "Pyrogenic Exotoxins (Erythrogenic Toxin)"
2. Medical Microbiology, 9th Edition (Murray et al.)
- ISBN: 9780323673228
- Covers: Staphylococcal diseases (skin, musculoskeletal, endocarditis), coagulase, cytotoxins, MRSA
- Relevant section: "Staphylococcal diseases subdivided into localized vs. toxin-mediated"
3. Sherris & Ryan's Medical Microbiology, 8th Edition
- ISBN: 9781260464283
- General microbiology reference covering bacteria, viruses, fungi, parasites
Supporting Clinical References
4. Harrison's Principles of Internal Medicine, 22nd Edition (2025)
- ISBN: 9781265977061
- Covers: Case definition of S. aureus TSS, skin & soft tissue infections, endocarditis treatment
- Relevant section: "Skin and Soft Tissue Infections", "TABLE 152-2 Case Definition of Staphylococcus aureus Toxic Shock"
5. Goldman-Cecil Medicine (International Edition)
- ISBN: 9780323930345
- Covers: TSS caused by TSST-1, Streptococcal TSS and necrotizing fasciitis
- Relevant section: "Toxic Shock Syndrome" (Chapter 406)
6. Fitzpatrick's Dermatology, Volume 1 & 2
- ISBN: 9780071837781
- Covers: Superantigen mechanism in TSS, Streptococcal toxin-associated syndromes, scarlet fever
- Relevant section: "Streptococcal Toxin-Associated Syndromes"
Summary Table
| Topic | Primary Reference |
|---|---|
| TSS - TSST-1 mechanism | Jawetz Microbiology 28e |
| TSS - Streptococcal type | Jawetz Microbiology 28e + Goldman-Cecil Medicine |
| Superantigen mechanism | Fitzpatrick's Dermatology + Jawetz |
| TSS treatment (MSSA/MRSA) | Harrison's Internal Medicine 22e |
| Staphylococcal skin diseases | Medical Microbiology 9e (Murray) |
| Staphylococcal endocarditis | Harrison's Internal Medicine 22e |
| General microbiology overview | Sherris & Ryan's Microbiology 8e |
Note: Your classroom notes (Marrow 8.0) are a simplified summary of these exact textbooks - mainly Jawetz and Murray's Medical Microbiology, which are the standard references for Indian medical exams (USMLE/NEET PG).
Streptococcus and staphylococcus... Too much confusion.. Make it simple
STAPH vs STREP - The Ultimate Simple Guide
First: How to Tell Them Apart
| Staphylococcus | Streptococcus | |
|---|---|---|
| Shape under microscope | Clusters (like a bunch of grapes) 🍇 | Chains (like a necklace) 📿 |
| Catalase test | POSITIVE | NEGATIVE |
| Key test | Coagulase test | Hemolysis + Lancefield grouping |
Memory trick: STAPH = Stays in clusters. STREP = String of chains.
STAPHYLOCOCCUS - Simplified
One test splits everything: COAGULASE
Staphylococcus
|
├── Coagulase POSITIVE → S. aureus ← THE DANGEROUS ONE
|
└── Coagulase NEGATIVE → S. epidermidis, S. saprophyticus (less dangerous)
S. aureus - Know These 3 Things
| Toxin | Disease caused |
|---|---|
| TSST-1 | Toxic Shock Syndrome |
| Exfoliatin | Scalded Skin Syndrome (skin peels off in newborns) |
| Enterotoxin | Food poisoning (vomiting within 6 hrs) |
| Protein A | Evades immune system |
| Coagulase | Clots blood around bacteria (hides from immune cells) |
- Skin: Boils, carbuncles, impetigo, folliculitis
- Bone: Osteomyelitis (#1 cause)
- Heart: Endocarditis (#1 in IV drug users)
- Lung: Pneumonia (post-flu especially)
- Systemic: Bacteremia, sepsis
- Normal (MSSA): Nafcillin / Oxacillin / Cloxacillin
- Resistant (MRSA): Vancomycin
CoNS (Coagulase Negative Staph) - Quick
| Bug | Disease | Clue |
|---|---|---|
| S. epidermidis | IV catheter/prosthetic device infections | Hospital bug, biofilm former |
| S. saprophyticus | UTI in young women | 2nd most common UTI bug after E. coli |
STREPTOCOCCUS - Simplified
Two systems to classify - use BOTH
System 1: Hemolysis (what it does to blood on agar)
| Type | What happens | Who |
|---|---|---|
| Beta (β) | COMPLETE destruction of RBCs = clear zone | S. pyogenes (Grp A), S. agalactiae (Grp B) |
| Alpha (α) | PARTIAL destruction = green zone | S. pneumoniae, Viridans strep |
| Gamma (γ) | NO hemolysis | Enterococcus |
Memory: Beta = Big destruction. Alpha = A little green. Gamma = Gone (no reaction).
System 2: Lancefield Groups (A, B, D...)
Streptococcus
|
├── Group A (β-hemolytic) → S. pyogenes ← MOST IMPORTANT
├── Group B (β-hemolytic) → S. agalactiae ← NEONATAL infections
├── Group D → Enterococcus faecalis
└── No group (α-hemolytic) → S. pneumoniae, Viridans
The 4 Key Strep Species
1. S. pyogenes (Group A Strep - GAS) ⭐ Most tested
- Strep throat (pharyngitis)
- Scarlet fever (sandpaper rash + strawberry tongue)
- Impetigo (non-bullous type)
- Necrotizing fasciitis ("flesh-eating")
- Streptococcal TSS
- Rheumatic fever (heart valve damage)
- Post-strep glomerulonephritis (kidney)
2. S. agalactiae (Group B Strep - GBS)
- Who it hurts: Neonates and pregnant women
- Diseases: Neonatal meningitis, neonatal sepsis, neonatal pneumonia
- Clue: Screen all pregnant women at 35-37 weeks
- Treatment: Penicillin
3. S. pneumoniae (Pneumococcus) - Alpha hemolytic, no Lancefield group
- Capsule = key virulence factor
- Causes: The "3 M's" - Meningitis, (pneu)Monia, Middle ear (otitis media) + Sinusitis
- At risk: Asplenic patients, elderly, children
- Clue: Lancet-shaped diplococci, bile soluble, optochin sensitive
- Treatment: Penicillin (if sensitive) / Ceftriaxone
4. Viridans Streptococci (Alpha hemolytic, no Lancefield group)
- Normal mouth flora
- S. mutans = dental caries (tooth decay)
- S. sanguis / S. mitis = subacute bacterial endocarditis (after dental procedures)
- Treatment: Penicillin
THE MASTER COMPARISON TABLE
| Feature | S. aureus (Staph) | S. pyogenes (Strep A) | S. pneumoniae (Strep) |
|---|---|---|---|
| Hemolysis | Beta | Beta | Alpha |
| Catalase | Positive | Negative | Negative |
| Coagulase | Positive | Negative | Negative |
| Key toxin | TSST-1, Exfoliatin | Streptolysin O/S | Pneumolysin |
| Throat infection | No | Yes (#1 cause) | No |
| Skin infection | Yes (#1 cause) | Yes (impetigo) | Rare |
| Meningitis | Yes (rare) | Rare | Yes (#1 in adults) |
| Endocarditis | Yes (#1 acute) | Rare | Rare |
| Osteomyelitis | Yes (#1) | Rare | Rare |
| Treatment | Nafcillin/Vanco | Penicillin | Penicillin/Ceftriaxone |
| Resistance | MRSA common | None to penicillin | Increasing |
One-Liner Memory Summary
STAPH = Clusters + Catalase+ → Coagulase+ (aureus) = Skin, Bone, Heart, Toxins STREP = Chains + Catalase- → Hemolysis type → Group A (throat/skin), B (babies), Pneumo (3 M's)
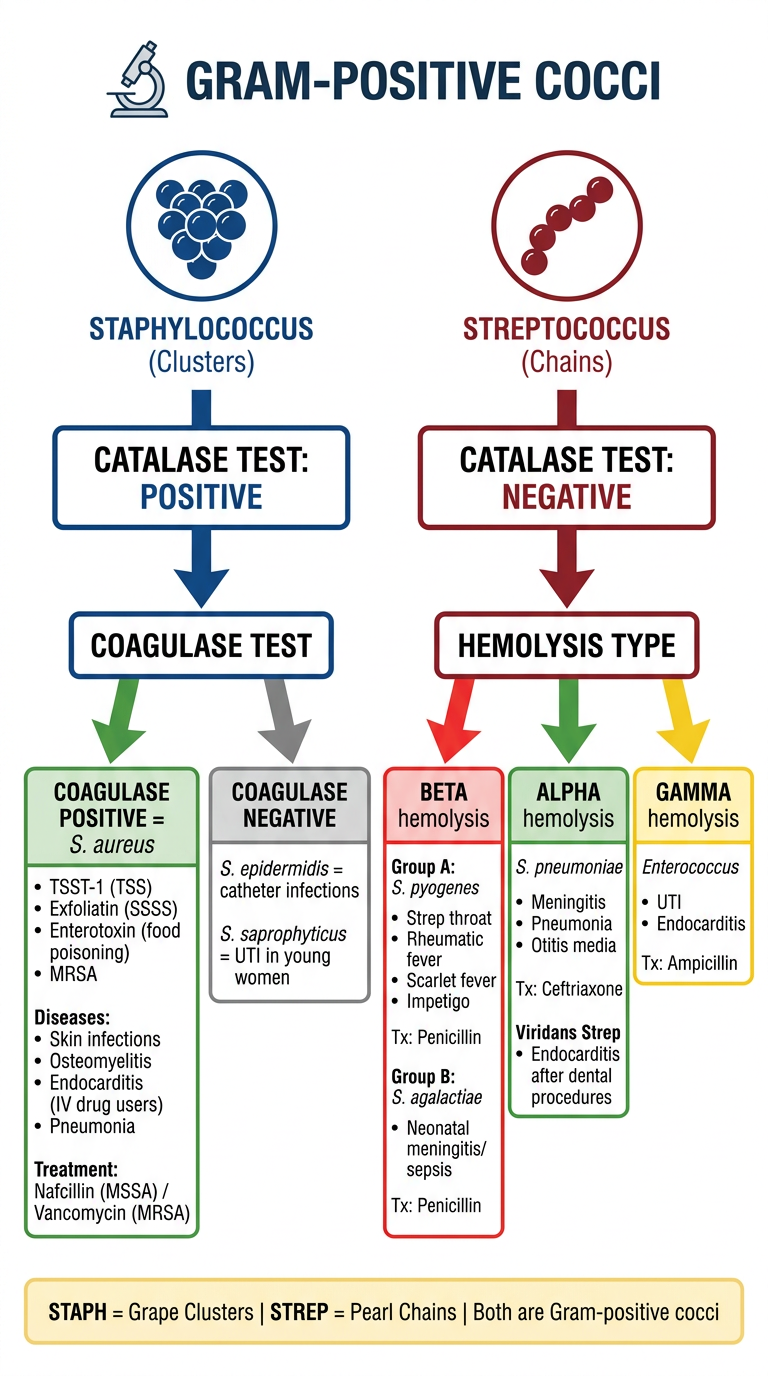
Create a visual flowchart/poster distinguishing Staph vs Strep
A clean, professional medical microbiology educational poster/flowchart distinguishing Staphylococcus vs Streptococcus for medical students. Layout: vertical flowchart on white background with two color-coded branches. TOP CENTER: Title "GRAM-POSITIVE COCCI" in bold dark text with a microscope icon. Below it: two round cocci bacteria icons - one in clusters labeled "STAPHYLOCOCCUS (Clusters)" in deep blue, one in chains labeled "STREPTOCOCCUS (Chains)" in deep red. LEFT BRANCH (Blue - Staphylococcus): - Box: "CATALASE TEST: POSITIVE" - Arrow down to: "COAGULASE TEST" - Two sub-branches: LEFT: Green box "COAGULASE POSITIVE = S. aureus" with bullet points: TSST-1 (TSS), Exfoliatin (SSSS), Enterotoxin (food poisoning), MRSA. Diseases: Skin infections, Osteomyelitis, Endocarditis (IV drug users), Pneumonia. Treatment: Nafcillin (MSSA) / Vancomycin (MRSA) RIGHT: Gray box "COAGULASE NEGATIVE" with: S. epidermidis = catheter infections, S. saprophyticus = UTI in young women RIGHT BRANCH (Red - Streptococcus): - Box: "CATALASE TEST: NEGATIVE" - Arrow down to: "HEMOLYSIS TYPE" - Three sub-branches: LEFT: Red box "BETA hemolysis" → Group A: S. pyogenes (Strep throat, Rheumatic fever, Scarlet fever, Impetigo) Tx: Penicillin. Group B: S. agalactiae (Neonatal meningitis/sepsis) Tx: Penicillin MIDDLE: Green box "ALPHA hemolysis" → S. pneumoniae (Meningitis, Pneumonia, Otitis media) Tx: Ceftriaxone. Viridans Strep (Endocarditis after dental procedures) RIGHT: Yellow box "GAMMA hemolysis" → Enterococcus (UTI, Endocarditis) Tx: Ampicillin BOTTOM: Memory tip box in light yellow: "STAPH = Grape Clusters | STREP = Pearl Chains | Both are Gram-positive cocci" Style: Clean medical textbook style, clear arrows, color-coded sections, easy to read fonts, professional educational poster design.
- Catalase POSITIVE → then Coagulase test
- Coagulase+ = S. aureus (dangerous one)
- Coagulase- = S. epidermidis / S. saprophyticus (less dangerous)
- Catalase NEGATIVE → then Hemolysis type
- Beta = Group A (throat/skin) + Group B (babies)
- Alpha = Pneumococcus + Viridans
- Gamma = Enterococcus
Catalase+ = STAPH | Catalase- = STREP