Skin in rheumatology and immunlogy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have rich textbook content from both Firestein & Kelley's and the Elsevier Rheumatology set. Here is a thorough, well-organized answer.
Skin in Rheumatology and Immunology
The skin is one of the most diagnostically informative organs in rheumatic and autoimmune disease. Cutaneous findings often precede systemic involvement, help classify disease, and can mirror disease activity. Below is a disease-by-disease breakdown.
1. Systemic Lupus Erythematosus (SLE)
Cutaneous lupus is classified using the Gilliam Classification into three major types:
A. Acute Cutaneous LE (ACLE)
- Malar ("butterfly") rash - erythematous, macular or raised, pruritic/painful, follows a malar distribution and spares the nasolabial folds (photoprotected region). Fluctuates with disease activity and lasts days to weeks.
- Generalized ACLE - widespread photosensitive erythema that may simulate toxic epidermal necrolysis in severe cases.
B. Subacute Cutaneous LE (SCLE)
- Widespread, nonscarring, nonindurated, photosensitive lesions.
- Start as erythematous papules/macules and evolve into:
- Papulosquamous form (resembles psoriasis or lichen planus)
- Annular/polycyclic form
- Strongly associated with anti-Ro (SSA) antibodies (up to 90% of SCLE). SCLE is also seen in Sjögren syndrome and RA with anti-SSA positivity.
C. Chronic Cutaneous LE (CCLE)
- Discoid LE (DLE) - most common chronic form. Erythematous plaques with thick adherent scale, follicular plugging, central hypopigmentation, and ultimately scarring + permanent alopecia when on the scalp.
- Lupus profundus (panniculitis) - firm deep subcutaneous nodules from lobular panniculitis. Overlying epidermis may be normal or show DLE changes.
- Bullous SLE - subepidermal bullae with neutrophilic infiltrate in dermal papillae (rare).
- Other chronic forms: chilblain lupus, tumid lupus, hypertrophic CLE.
D. Non-specific SLE skin signs
- Livedo reticularis, Raynaud's phenomenon, oral/nasal ulcers, hair thinning, photosensitivity.
E. Histopathology and Immunopathology
- Liquefactive (vacuolar) degeneration of the basal cell layer, fibrinoid necrosis, and perivascular/perifollicular T-cell infiltrate.
- Lupus band test - immunofluorescence demonstrates IgG, IgA, IgM + complement deposits at the dermal-epidermal junction (DEJ). Positive in both lesional AND non-lesional sun-exposed skin in active SLE. Can also be positive in RA, Sjögren, DM, and SSc.
- Rheumatology, 2-Volume Set (2022, Elsevier), pp. 1217-1224
2. Dermatomyositis (DM)
The skin rashes are often the most visible feature and some are pathognomonic.
Pathognomonic signs
| Sign | Description |
|---|---|
| Gottron's papules | Slightly elevated, violaceous/pink papules over the dorsal MCP/IP joints (knuckles), elbows, and knees. Considered pathognomonic. |
| Heliotrope rash | Periorbital red/violaceous erythema of one or both eyelids, often with edema. |
Highly specific signs
- Linear extensor erythema - over extensor joint surfaces.
- V-sign - photosensitive rash over the anterior neck and upper chest.
- Shawl sign - erythema over the upper back and shoulders.
- Holster sign - erythema over the hips and thighs.
Periungual changes
- Nailfold telangiectasias, periungual erythema, cuticular overgrowth, digital ulceration.
Other skin features
- Mechanic's hands (hyperkeratotic fissuring of the lateral fingers), panniculitis, livedo reticularis, nonscarring alopecia, poikiloderma (hypo/hyperpigmentation in late disease), pruritus (often severe).
Key differential - DM rash affects the knuckles but spares the phalanges, whereas SLE rash affects the phalanges but spares the knuckles.
In Juvenile DM (JDM)
- Gottron's papules and heliotrope are the hallmarks.
- Calcinosis (in 40%+) and ulcerative skin lesions - more common in JDM than adult DM. Ulcerative lesions herald systemic vasculopathy.
- Nailfold capillaroscopy shows dilated, abnormally shaped capillaries correlating with disease duration and severity.
- Firestein & Kelley's Textbook of Rheumatology, p. 2412; Rheumatology (Elsevier), p. 1575
3. Systemic Sclerosis (SSc / Scleroderma)
Skin involvement is the hallmark of SSc.
Skin Fibrosis
- Begins with edema and pruritus in early diffuse disease, progressing to fibrosis.
- Histology: dermal edema → mononuclear perivascular infiltrates → markedly increased collagen deposition in the reticular dermis → loss of hair follicles, sweat glands, and the intradermal white adipose layer.
- Myofibroblasts (α-SMA positive) are central to fibrosis.
- Late stage: acellular dermis with compact hyalinized collagen, loss of rete pegs, effacement of dermal-epidermal ridges.
- Modified Rodnan Skin Score (mRSS) is used clinically to grade skin thickness.
- Diffuse cutaneous SSc (dcSSc): proximal limb + trunk skin involvement; tends to improve over 3-5 years.
- Limited cutaneous SSc (lcSSc): restricted to face, neck, and extremities (CREST features).
Vascular Skin Changes
- Raynaud's phenomenon - triphasic color change (white/blue/red) in response to cold.
- Telangiectasias - classical palmar/facial lesions and serpiginous patterns. Increasing telangiectasia predicts pulmonary arterial hypertension.
- Rarefaction of dermal capillaries → chronic hypoxia → VEGF upregulation.
- Pruritus - prominent in early dcSSc; also occurs in late disease with skin dryness.
- Firestein & Kelley's Textbook of Rheumatology, p. 1680; Rheumatology (Elsevier), p. 1135
4. Psoriatic Arthritis (PsA) and Psoriasis
- 84% of PsA patients develop skin psoriasis before joint disease (typically 7-10 years before joint involvement).
- Up to 30% of psoriasis patients develop PsA.
- Higher risk psoriasis phenotypes for PsA development: nail disease, scalp, intergluteal, and inverse/flexural psoriasis. Obesity also increases risk.
- No direct correlation exists between extent of skin disease and extent of joint involvement.
- Nails: 60-80% of PsA patients have nail involvement (vs 20-40% in uncomplicated psoriasis). Nail-joint anatomical connection via Sharpey fibers to the distal phalanx underpins this association. Nail changes often precede joint involvement by only 1-2 years.
Immunopathology of psoriatic skin
- IL-23 → Th17 differentiation → IL-17A + TNF → keratinocyte hyperproliferation.
- Epidermal hyperplasia, mononuclear leukocytes in papillary dermis, neutrophils in the stratum corneum, increased dendritic cells (producing TNF, IL-12, IL-23).
- CD8+ T cells predominate in the epidermis; CD4+/CD8+ mix in the dermis.
- Prominent vascular changes with growth and dilation of superficial vessels (distinctive from RA synovium).
- Firestein & Kelley's Textbook of Rheumatology, p. 1665
5. Rheumatoid Arthritis (RA)
Vasculitis-related skin manifestations
| Feature | |
|---|---|
| Petechiae/purpura | |
| Digital infarcts | |
| Nailfold telangiectasias and infarctions | |
| Gangrene | |
| Livedo reticularis | |
| Necrotizing granulomatous vasculitis | |
| Erythema elevatum diutinum | |
| Urticaria vasculitis |
Nonspecific and associated skin disorders in RA
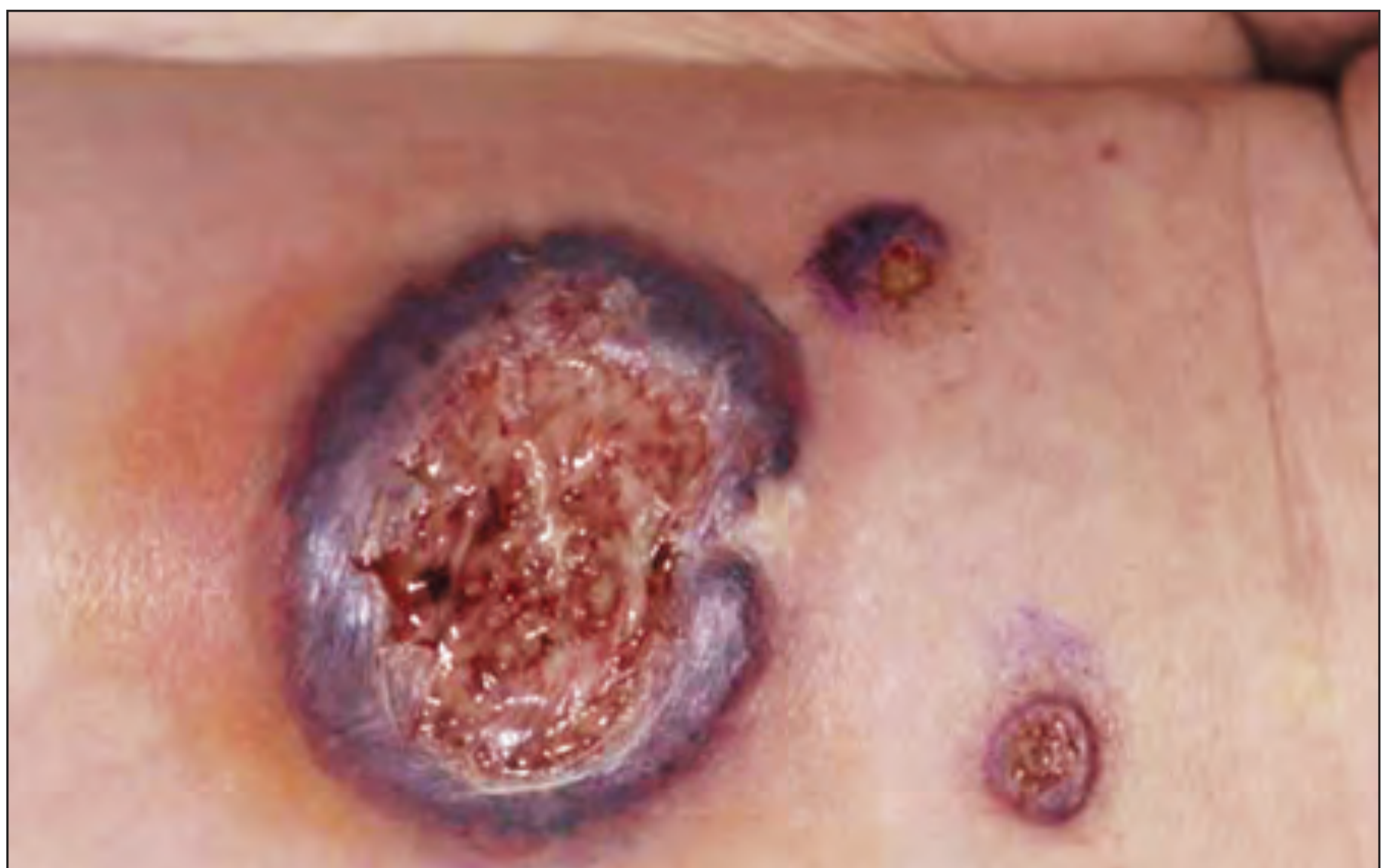
- Pyoderma gangrenosum (PG) - painful ulcer with undermined hemorrhagic borders (see image below). Histology shows neutrophilic infiltrate and small abscesses. Not directly correlated with RA course. DD includes venous/arterial ulcers, antiphospholipid syndrome, vasculitis.
- Palisaded neutrophilic and granulomatous dermatitis
- Interstitial granulomatous dermatitis
- Atrophic/fragile and transparent skin
- Palmar erythema, periungual erythema
- Splinter hemorrhages, nailfold thromboses
- Erythema nodosum, erythema multiforme, urticaria
- Alopecia areata, vitiligo
- Yellow nail syndrome
- Rheumatology (Elsevier), p. 322
6. Sjögren Syndrome
- Most common dermatologic feature: xerosis (dry skin), eyelid dermatitis, angular cheilitis.
- Annular erythema - three types:
- Type I: donut-ring erythema with elevated border (specific to primary Sjögren's, mainly Asian populations)
- Type II: SCLE-like polycyclic scaled erythema
- Type III: papular insect bite-like erythema
- Histology: deep perivascular lymphocytic infiltrate WITHOUT the epidermal changes of lupus.
- Cutaneous vasculitis: most common form is palpable purpura of the lower extremities. Associated with anti-Ro/SS-A and anti-La/SS-B antibodies, cryoglobulins (~50%), and elevated RF.
- Cutaneous vasculitis predicts extraglandular manifestations: arthritis, peripheral neuropathy, Raynaud's.
- Firestein & Kelley's Textbook of Rheumatology, p. 1505
7. Cutaneous Vasculitis in Rheumatic Disease
Vessel size and depth correlation
- Firestein & Kelley's Textbook of Rheumatology
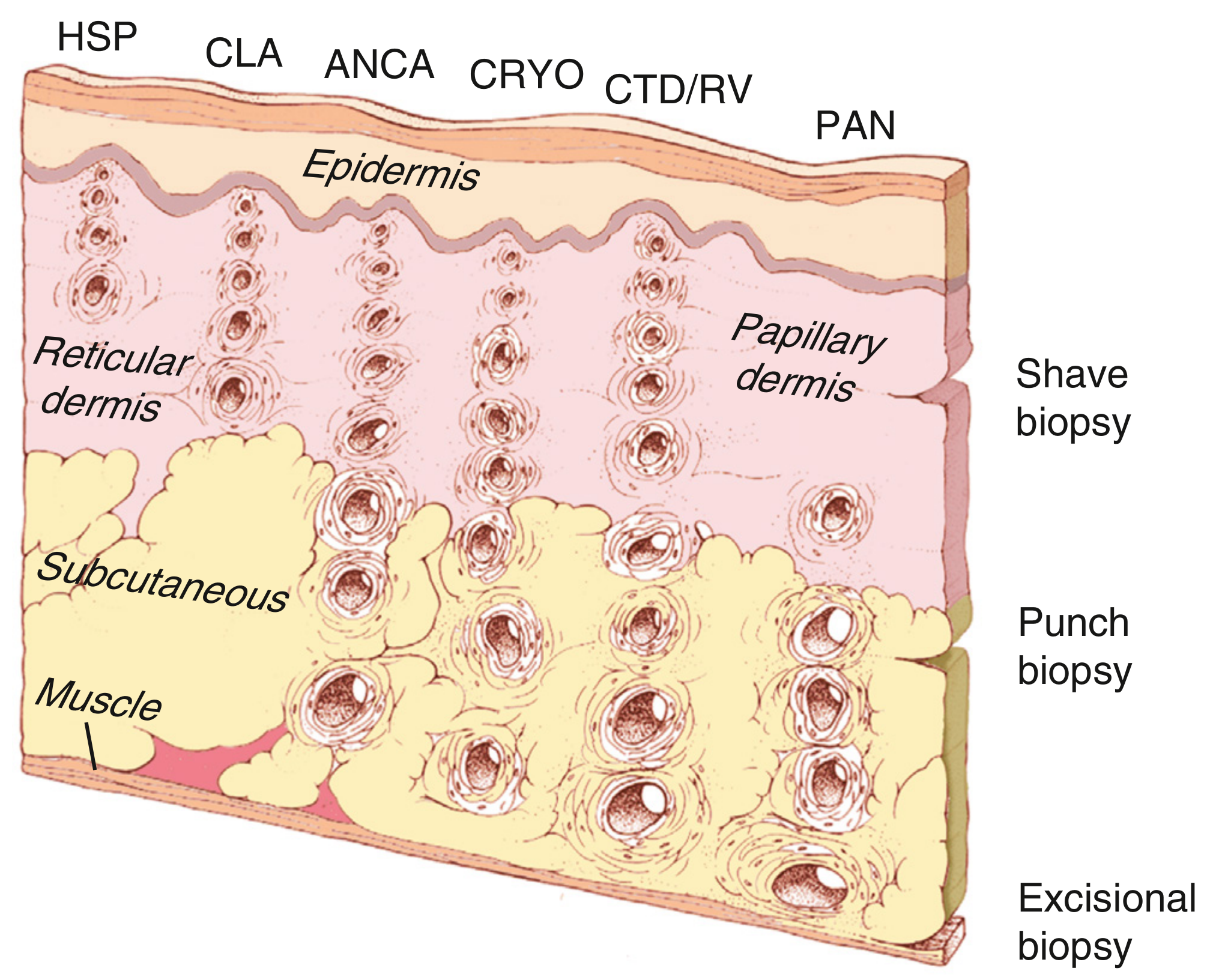
The depth of cutaneous vasculitis corresponds to vessel size:
- Small vessels (<50 µm): capillaries, postcapillary venules - in the papillary dermis → IgA vasculitis (HSP), cutaneous leukocytoclastic angiitis (CLA), mixed cryoglobulinemia, CTD/rheumatoid vasculitis, ANCA vasculitis.
- Medium vessels (50-150 µm): in the reticular dermis/subcutaneous junction → PAN.
Key skin manifestation: Palpable purpura
- Palpable purpura = synonymous with small vessel vasculitis - the most common cutaneous finding in immune complex-mediated vasculitis.
- Results from erythrocyte extravasation through damaged vessel walls.
- Does not blanch on pressure (unlike reactive hyperemia).
- Other forms: vesicles, pustules, urticaria, superficial ulcerations, macules/patches, splinter hemorrhages.
- Firestein & Kelley's Textbook of Rheumatology, p. 2022
Summary Table: Skin Findings by Disease
| Disease | Hallmark Skin Features |
|---|---|
| SLE | Malar rash (spares nasolabial folds), SCLE (annular/papulosquamous), DLE (scarring), lupus profundus, bullous SLE |
| Dermatomyositis | Gottron's papules (pathognomonic), heliotrope rash, V-sign, shawl sign, mechanic's hands, nailfold telangiectasias |
| SSc | Skin thickening/fibrosis (mRSS), Raynaud's, telangiectasias, pruritus, digital pitting scars |
| Psoriatic arthritis | Plaque psoriasis (84% before joint disease), nail pitting/onycholysis, DIP involvement |
| RA | Rheumatoid nodules, vasculitis changes, pyoderma gangrenosum, palpable purpura |
| Sjögren | Xerosis, annular erythema, palpable purpura (lower limbs), cutaneous vasculitis |
| IgA vasculitis (HSP) | Palpable purpura (buttocks/lower limbs), petechiae |
| JDM | Gottron's papules, heliotrope, calcinosis, ulcerative lesions, nailfold capillary changes |
Key Immunological Mechanisms
| Mechanism | Disease | Skin consequence |
|---|---|---|
| Immune complex deposition at DEJ | SLE | Lupus band test positive; vacuolar basal cell damage |
| IL-23/Th17/IL-17A axis | Psoriasis/PsA | Epidermal hyperplasia, neutrophils in stratum corneum |
| TGF-β/myofibroblast activation | SSc | Dermal collagen accumulation and fibrosis |
| Small vessel vasculitis (IgA, IC) | Vasculitides, RA, SLE | Palpable purpura, digital infarcts |
| CD4+ T-cell mediated | DM | Perifollicular and perivascular dermal infiltrate |
Sources:
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set (2023)
- Rheumatology, 2-Volume Set (Elsevier, 2022)
This is a shared conversation. Sign in to Orris to start your own chat.