Csom ent topic explain in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple authoritative ENT textbooks. Let me compose the detailed answer.
CSOM - Chronic Suppurative Otitis Media: A Complete Overview
Definition
Chronic Suppurative Otitis Media (CSOM) is a chronic inflammatory condition of the middle ear and mastoid, characterized by a persistent or recurrent discharge (otorrhea) through a non-intact tympanic membrane (perforation), lasting more than 2-6 weeks. It represents the end stage of a spectrum of middle ear disease driven primarily by Eustachian tube dysfunction.
Classification
CSOM is traditionally divided into two types based on the site of tympanic membrane involvement and potential danger:
1. Tubotympanic (Safe/Benign) Type
- Perforation involves the pars tensa (central or subtotal)
- No cholesteatoma
- Associated with mucosal disease
- Discharge is mucoid or mucopurulent
- Considered "safe" - rarely causes serious complications
2. Atticoantral (Unsafe/Dangerous) Type
- Perforation involves the pars flaccida (attic/marginal)
- Cholesteatoma is present
- Bone erosion is a hallmark
- Discharge is scanty, foul-smelling (fetid)
- "Unsafe" - serious intracranial and extracranial complications possible
(Shambaugh Surgery of the Ear, p. 466)
Pathophysiology / Etiology
CSOM is believed to originate from Eustachian tube (ET) dysfunction leading to a cascade of pathological events:
- ET dysfunction → negative middle ear pressure → persistent middle ear effusion (MEE)
- The MEE causes mucosal edema, inflammatory mediator release, and mucosal metaplasia to a secretory type - perpetuating the effusion
- Bacterial infection of the effusion → purulent discharge → rupture of the tympanic membrane basement membrane
- Granulation tissue formation: inflammatory cells + lamina propria elements extrude through the basement membrane. Angiogenic and epithelial growth factors drive fibroblast recruitment, neovascularization, and polyp formation
- Enzymatic weakening of the tympanic membrane: enzymes in the effusion and granulation tissue break down collagen - leading to retraction pockets and eventually perforation
- Deep retraction pockets + perforations create the conditions for cholesteatoma genesis
(Shambaugh Surgery of the Ear, pp. 527-528)
Microbiology
Common organisms isolated in CSOM:
| Type | Organisms |
|---|---|
| Gram-negative (most common) | Pseudomonas aeruginosa, Proteus mirabilis, Klebsiella |
| Gram-positive | Staphylococcus aureus (including MRSA), Streptococcus spp. |
| Anaerobes | Bacteroides, Peptostreptococcus (especially in cholesteatoma - responsible for fetid odor) |
| Fungi (secondary) | Candida albicans, Aspergillus (especially after prolonged antibiotic use) |
One prospective study found Candida species in 10% of ears with purulent otorrhea, rising to 35% after topical ciprofloxacin treatment for 3 weeks - highlighting the risk of fungal overgrowth. (Cummings Otolaryngology, p. 3072)
Clinical Features
Symptoms
- Otorrhea: intermittent or persistent - the hallmark symptom
- Tubotympanic type: mucoid/mucopurulent, not fetid
- Atticoantral/cholesteatoma type: scanty, foul-smelling (fetid)
- Conductive hearing loss: virtually always present; CHL > 30 dB suggests ossicular erosion
- Otalgia and headache: uncommon in uncomplicated CSOM - their presence should raise suspicion of intracranial involvement or malignancy
- Vertigo: raises suspicion for labyrinthine fistula or labyrinthitis
- Occasionally blood-stained discharge with aural polyp formation
(Shambaugh Surgery of the Ear, p. 528)
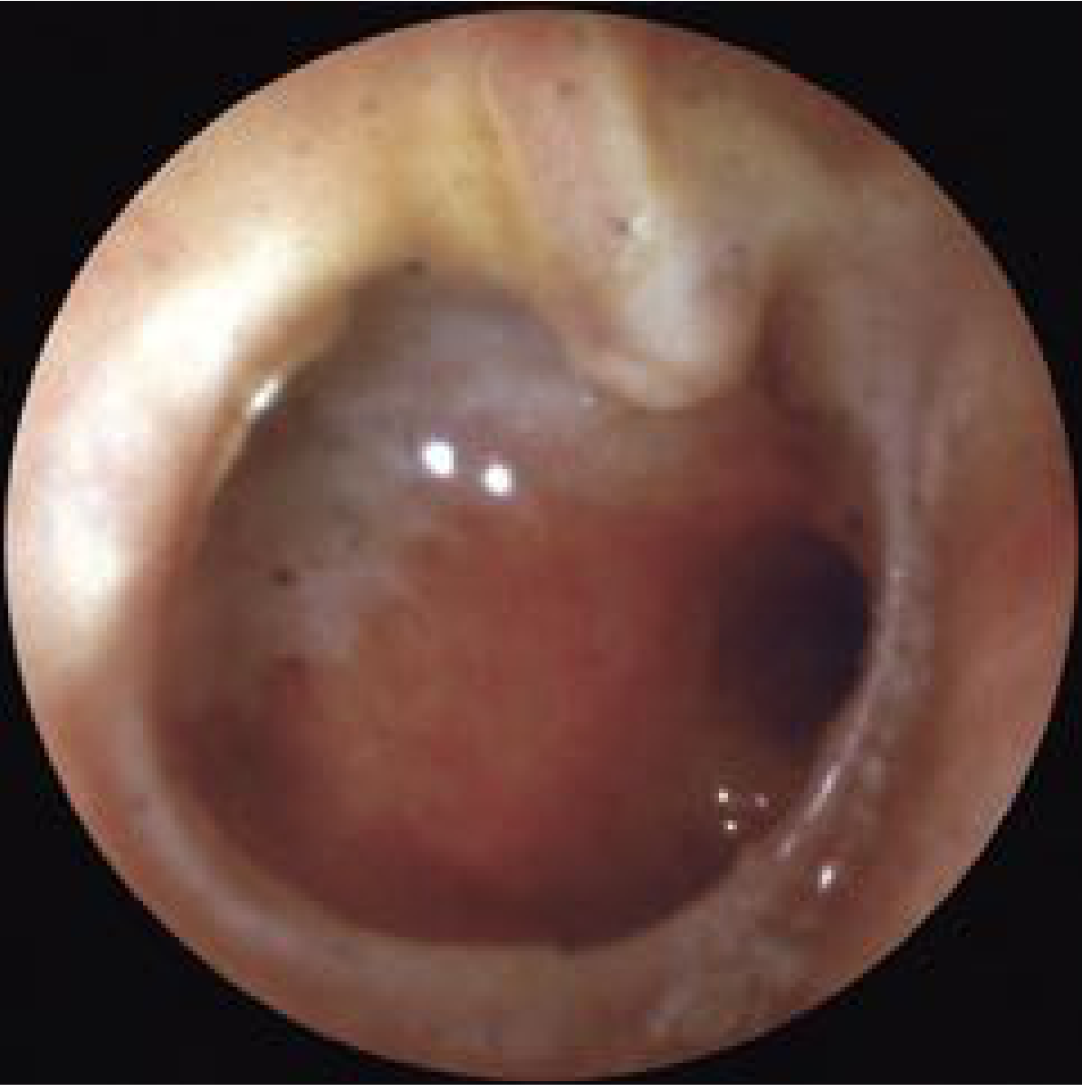
Signs (on otoscopy/otomicroscopy)
- Tympanic membrane perforation (central vs. marginal/attic)
- Discharge in the canal (may obscure the TM)
- Granulation tissue or aural polyps in the EAC
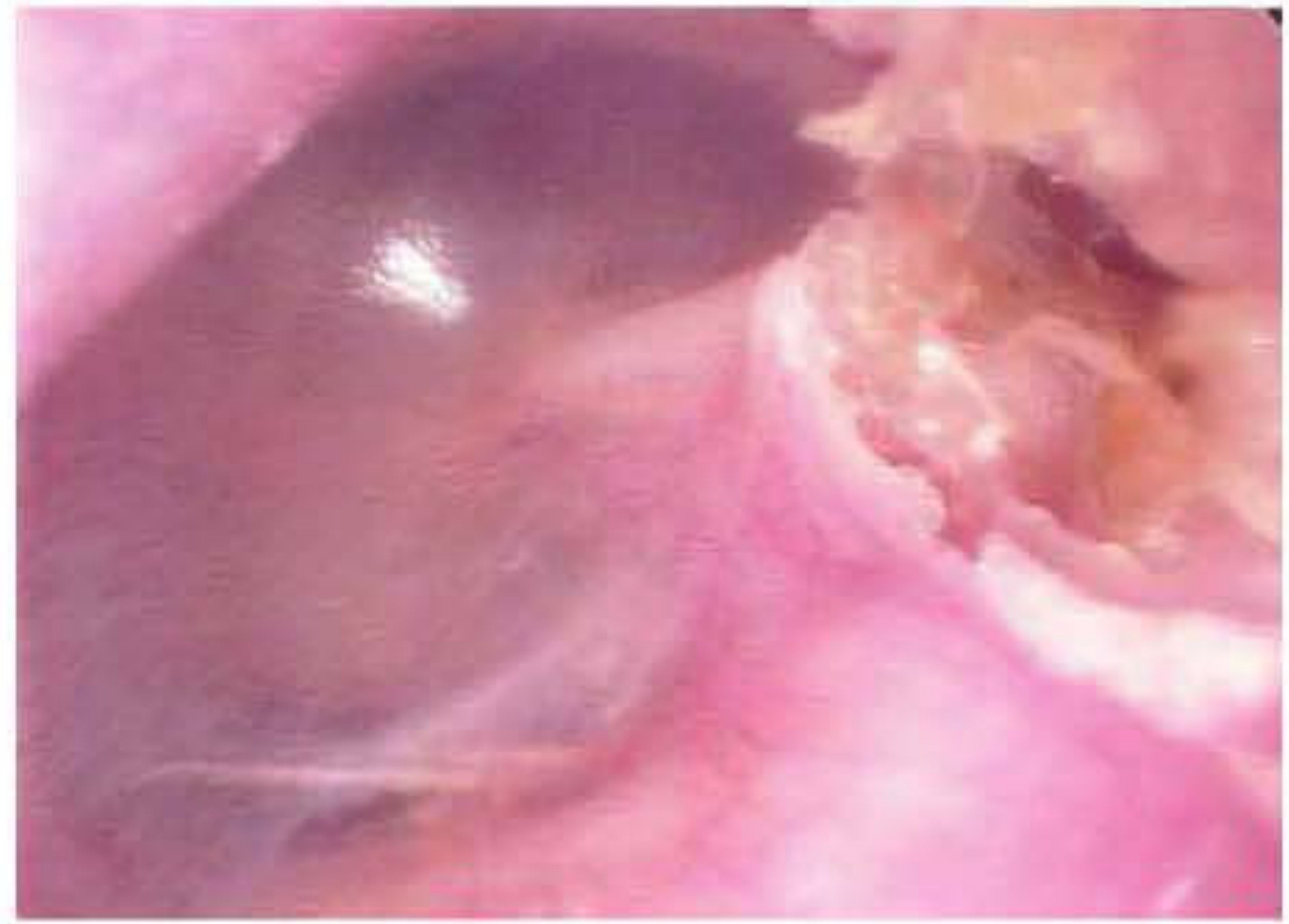
- Evidence of cholesteatoma (white, pearly mass, keratin flakes)
- Scutal erosion (bone erosion at the attic wall)
- Ossicular erosion may be visible through the perforation
Tympanic Membrane Perforation - Clinical Image
Cholesteatoma - The Dangerous Component
Cholesteatoma = epidermal inclusion of keratinizing squamous epithelium within the middle ear or mastoid. The name (coined by Johannes Müller in 1838) is a misnomer - it actually contains keratin, not cholesterol. Cruveilhier first described it as a "pearly tumor" of the temporal bone.
Types
- Congenital: present behind an intact TM, no history of infection
- Acquired Primary: from deep retraction pocket of pars flaccida (attic), no prior perforation
- Acquired Secondary: keratinizing epithelium migrates through a pre-existing perforation
How Cholesteatoma Destroys Bone
The mechanism is complex and multifactorial:
- Cholesteatoma-bone contact → normal mucosal lining degenerates
- Macrophages, monocytes, and osteoclasts accumulate
- Elevated cytokines: TNF-α, IL-1α, IL-1β, IL-6, IFN-γ, EGF, PTHrp
- Lipopolysaccharides prime osteoclast precursors via RANKL pathway
- Nitric oxide type II enhances osteoclastic activation synergistically with IL-1β and TNF-α
- Result: progressive bone erosion of ossicular chain, scutum, tegmen, otic capsule, fallopian canal
(Shambaugh Surgery of the Ear, pp. 453-454)
Pathology Without Cholesteatoma
In CSOM without cholesteatoma, histopathology reveals:
- Granulation tissue in 96% of cases
- Ossicular changes in 96%
- Tympanosclerosis in 43%
- Cholesterol granuloma in 21%
The inflammatory sequence progresses from mucosal edema → submucosal fibrosis → lymphocytic infiltrate → soft, friable granulation tissue → polyp formation. (Cummings Otolaryngology, p. 2690)
Diagnosis
History
- Chronic intermittent otorrhea (character, duration, odor)
- Degree of hearing loss
- History of prior ear surgery or medical treatment
- Presence of vertigo, facial weakness, or headache (alarm features for complications)
Examination
- Full head and neck exam including otomicroscopy
- Note: EAC edema, polyps, discharge
- TM: perforation site, retraction, atelectasis, cholesteatoma
- Middle ear mucosa through perforation: granulation tissue, ossicular erosion, scutal erosion
Audiometry
- Conductive hearing loss - most common
- CHL > 30 dB: suggests ossicular erosion
- Sensorineural hearing loss (5-33 dB range in studies) - may coexist; must be documented preoperatively
- Note: hearing may be preserved despite ossicular erosion if sound transmits directly to oval window via cholesteatoma matrix
Imaging
- High-resolution CT temporal bone (HRCT): gold standard for evaluating extent of disease, bone erosion, cholesteatoma extent, tegmen integrity, facial nerve canal involvement
- MRI (non-echo planar DW-MRI): preferred for detecting residual/recurrent cholesteatoma, especially after surgery; avoids CI artifact issues
- Both modalities complementary in complex cases
Complications
Complications arise from spread of infection or from mechanical destruction by cholesteatoma.
Extracranial Complications
- Acute mastoiditis / Coalescent mastoiditis
- Postauricular abscess
- Bezold abscess (pus tracking along sternomastoid under deep cervical fascia)
- Temporal abscess
- Petrous apicitis (Gradenigo syndrome: triad of otorrhea, retroorbital pain, abducens palsy)
- Labyrinthine fistula (most commonly lateral semicircular canal)
- Facial nerve paralysis (erosion of the fallopian canal)
- Acute suppurative labyrinthitis
- Encephalocele and CSF leakage
Intracranial Complications
- Meningitis (most common intracranial complication)
- Brain abscess (temporal lobe or cerebellar)
- Subdural empyema
- Epidural abscess
- Lateral sinus thrombosis
- Otitic hydrocephalus
(Cummings Otolaryngology, Box 141.1)
Medical Treatment
The goal of medical management is to "dry the ear" and control inflammation:
- Aural toilet (ear suctioning/debridement) - removes debris, discharge, and biofilm; essential before topical therapy
- Ototopical antibiotics: fluoroquinolones (ciprofloxacin/ofloxacin eardrops) are first-line - safe, effective, minimal ototoxicity
- Systemic antibiotics: used if ototopical treatment insufficient or signs of systemic spread; guided by culture and sensitivity
- Antifungal treatment: if fungal overgrowth suspected (especially post-antibiotic treatment); clotrimazole drops or systemic azoles
- Avoid water contamination of the ear (ear protection during bathing)
Indications to escalate to surgery:
- Failed multiple attempts at medical treatment
- Cholesteatoma (near-absolute indication for surgery)
- Symptoms suggesting complications: vertigo, facial weakness, headache
- Persistent/progressive disease despite adequate medical therapy
(Shambaugh Surgery of the Ear, pp. 528-529)
Surgical Treatment
The three priorities in surgery for CSOM (in order):
- Eradication of disease
- Prevention of recurrence
- Preservation or restoration of hearing
Types of Surgery
Tympanoplasty (Myringoplasty for isolated TM perforation)
- Repair of TM perforation alone (Type I tympanoplasty) or with ossicular reconstruction
- Temporalis fascia is the most widely used graft material
- Underlay vs. overlay technique
- Success depends on: dry ear preoperatively, ET function, size/site of perforation
Mastoidectomy Types
| Procedure | Description | When Used |
|---|---|---|
| Canal Wall Up (CWU) / Intact Canal Wall | Posterior EAC wall preserved; mastoid exenterated via cortical mastoidectomy | Localized disease, good access, easier aftercare |
| Canal Wall Down (CWD) / Modified Radical Mastoidectomy | Posterior EAC wall removed; creates open mastoid cavity | Extensive cholesteatoma, poor ET function, revision cases |
| Radical Mastoidectomy | As CWD + middle ear obliterated; no hearing reconstruction | Rarely needed; extensive unresectable disease |
CWU advantages: Normal anatomy preserved, no cavity care, no water restrictions, better hearing results
CWD advantages: Better disease clearance, lower cholesteatoma recurrence, complete visualization
CWD advantages: Better disease clearance, lower cholesteatoma recurrence, complete visualization
Ossiculoplasty
- Reconstruction of eroded ossicular chain at time of tympanoplasty or at second stage
- Materials: autologous cartilage/bone, PORP (Partial Ossicular Replacement Prosthesis), TORP (Total Ossicular Replacement Prosthesis)
Second-Look Surgery
In CWU mastoidectomy for cholesteatoma, a planned second-look operation at 9-12 months is often recommended to identify residual disease, as recurrence rates can be significant.
(Shambaugh Surgery of the Ear, pp. 528-529)
CSOM and Cochlear Implantation
CSOM was initially considered a contraindication to cochlear implantation (CI). Current practice:
- Staged approach: first stage clears disease (radical mastoidectomy ± mastoid obliteration), CI performed 2-6 months later when the ear is dry
- If a stable, dry cavity exists, single-stage blind sac closure + CI may be feasible
- Microbial biofilms (bacterial or fungal) on the CI are a significant risk - must be eradicated before implant insertion
- All patients receive antimicrobial prophylaxis perioperatively
(Scott-Brown's Otorhinolaryngology, p. 142; Cummings Otolaryngology, pp. 3072-3073)
Summary Table
| Feature | Tubotympanic (Safe) | Atticoantral (Unsafe) |
|---|---|---|
| TM Perforation | Central/pars tensa | Marginal/attic/pars flaccida |
| Cholesteatoma | Absent | Present |
| Discharge | Mucoid, not fetid | Scanty, fetid |
| Hearing loss | Conductive | Conductive (may be severe) |
| Bone erosion | Rare | Common |
| Complications | Uncommon | Common, serious |
| Treatment | Medical ± tympanoplasty | Surgery mandatory |
Sources:
- Shambaugh Surgery of the Ear, pp. 527-529, 453-454, 466
- Cummings Otolaryngology Head and Neck Surgery, pp. 2690, 3072-3073, Box 141.1
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, p. 142
This is a shared conversation. Sign in to Orris to start your own chat.