Lymphatic drainage of tongue answer as a 10marks question
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from the textbooks. Let me compose the full 10-mark answer.
Lymphatic Drainage of the Tongue
Introduction
The tongue has a rich lymphatic network that ultimately drains into the deep cervical chain of nodes along the internal jugular vein. The pattern of drainage is regionally specific, varies between the oral (anterior two-thirds) and pharyngeal (posterior one-third) parts, and has critical clinical significance because of the tongue's tendency for lymphatic metastasis.
Lymphatic Vessels of the Tongue
The lymphatic vessels of the tongue are arranged into three groups based on their origin:
- Marginal vessels – arise from the mucosa at the edges of the tongue
- Central vessels – arise from the central mucosa and deep tongue musculature
- Apical vessels – arise from the tip of the tongue
Regional Drainage — By Region
1. Tip of the Tongue
- Lymphatics from the tip pierce the mylohyoid muscle and drain into the submental nodes (Level IA).
- From there, drainage proceeds to the jugulo-omohyoid node (a large node of the lower deep cervical group at the crossing of the omohyoid muscle and internal jugular vein).
- This is a key landmark node specifically associated with the tongue.
2. Anterior (Oral) Tongue — Lateral Borders
- The lateral margins of the oral tongue drain primarily to submandibular nodes (Level IB) and upper deep cervical nodes (Levels I–II, particularly the jugulodigastric node).
- Lymphatics may also drain directly into Levels III and IV (mid- and lower jugular nodes), skipping Levels I and II — a clinically important phenomenon in tongue cancer management.
- Drainage is predominantly ipsilateral due to the lack of anastomoses between anterior lymphatics and the presence of the median fibrous lingual septum, which acts as a partial barrier to crossover drainage.
3. Posterior (Pharyngeal) Tongue — Base of Tongue
- The posterior one-third (base) of the tongue drains through the pharyngeal wall directly into the upper cervical lymphatics, primarily the jugulodigastric nodes (Level II).
- This region has a rich lymphatic plexus with extensive crossover connections, resulting in frequent bilateral cervical lymph node spread (up to 20% incidence of bilateral metastasis in carcinoma).
- The base of tongue also communicates with retropharyngeal and lateral pharyngeal nodes.
Summary Table
| Region | First-Echelon Nodes | Final Destination |
|---|---|---|
| Tip | Submental (Level IA) | Jugulo-omohyoid node |
| Lateral oral tongue | Submandibular (Level IB), Upper deep cervical (Level II) | Deep cervical chain |
| Dorsum/central oral tongue | Submental + submandibular (bilateral possible) | Deep cervical chain |
| Base of tongue (posterior 1/3) | Jugulodigastric (Level II), retropharyngeal | Deep cervical chain, bilateral |
Final Common Pathway
All lymphatic drainage from the tongue ultimately reaches the deep cervical chain along the internal jugular vein. From there, lymphatic vessels form the:
- Right jugular trunk → right lymphatic duct → right venous angle
- Left jugular trunk → thoracic duct → left venous angle
Diagram
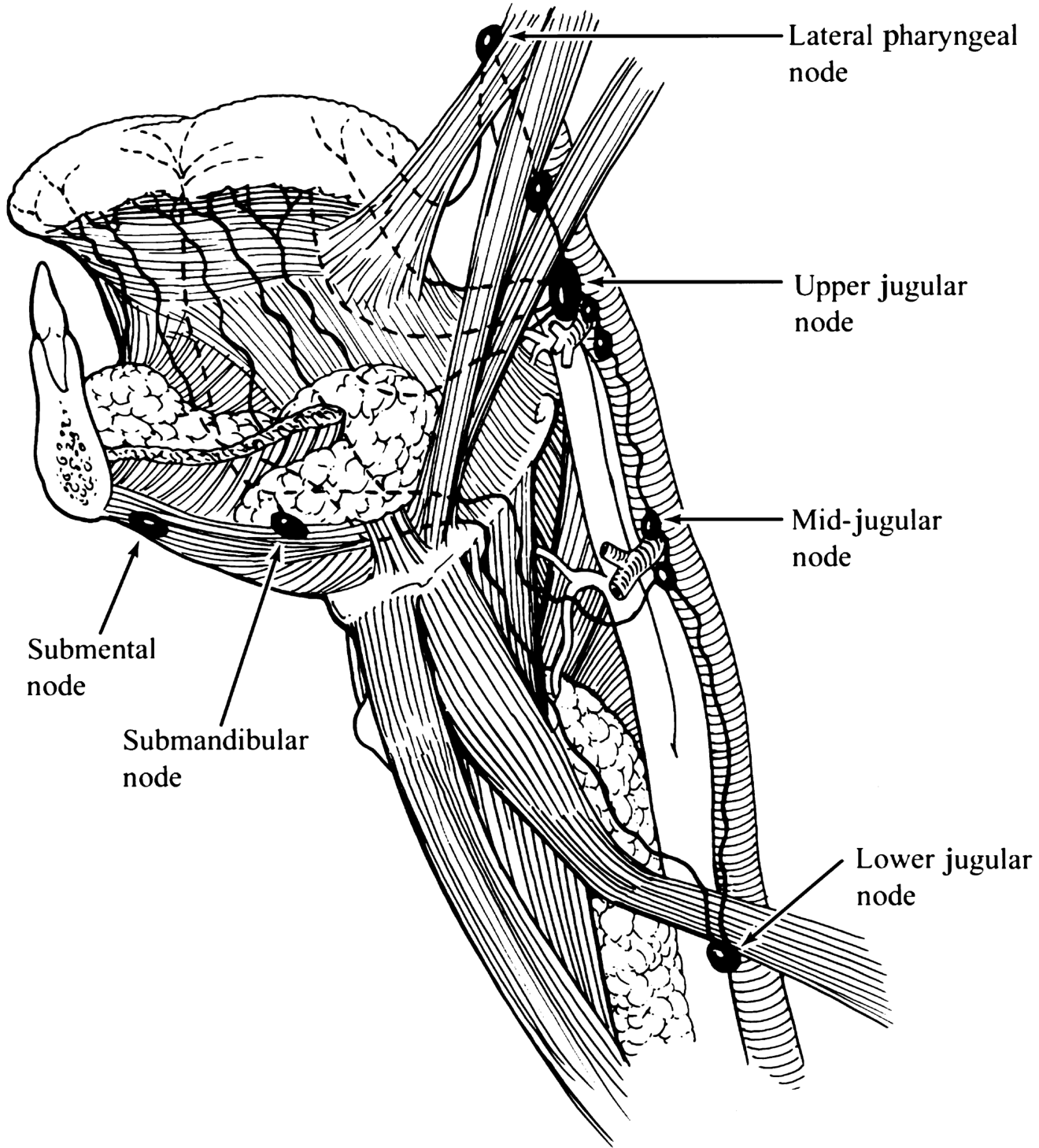
Lymphatic drainage of the oral tongue and oropharynx — K.J. Lee's Essential Otolaryngology, Fig. 45-3
Clinical Significance
-
Skip metastasis: Oral tongue carcinoma can metastasize directly to Levels III/IV without involving Levels I/II. This mandates addressing the lower neck even in early disease.
-
Bilateral drainage at the base: Midline and posterior tongue lesions drain bilaterally. Cancer at the base of the tongue therefore warrants bilateral neck dissection or bilateral irradiation.
-
Occult nodal disease: 20–25% of oral tongue cancers have occult (clinically undetectable) nodal metastases, making elective treatment of the neck (elective neck dissection or sentinel node biopsy) important.
-
Depth of invasion: Tumors >2–4 mm deep have significantly higher rates of regional lymph node spread.
-
Jugulo-omohyoid node enlargement: Isolated enlargement of this node is a classic sign of tongue carcinoma and should prompt thorough tongue examination.
Sources:
- Gray's Anatomy for Students — Lymphatics of the tongue (Deep cervical lymph nodes section)
- Cummings Otolaryngology: Head and Neck Surgery — Oral Tongue, Base of Tongue (pp. 1655)
- K.J. Lee's Essential Otolaryngology — Carcinoma of the Oral Tongue, Fig. 45-3
This is a shared conversation. Sign in to Orris to start your own chat.