Portal hypertension General surgery PG exam theory
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from Bailey & Love, Schwartz's, and Sabiston. I have enough to write a thorough PG exam-style answer. Let me now compile the complete answer.
Portal Hypertension - General Surgery PG Exam Theory
Sources: Bailey & Love's Short Practice of Surgery (28th ed), Schwartz's Principles of Surgery (11th ed), Sabiston Textbook of Surgery
Definition
Portal hypertension is defined as a portal venous pressure >10 mmHg (normal: 5-10 mmHg). Clinically significant portal hypertension begins at a hepatic venous pressure gradient (HVPG) >10 mmHg, and variceal bleeding is unlikely below 12 mmHg. Portal hypertension per se produces no symptoms - it is diagnosed following presentation with its complications.
Portal Venous Anatomy (High-Yield)
- Portal vein carries ~75% of total hepatic blood flow and 72% of hepatic oxygen supply
- Flow: 1000-1500 mL/min in normal adults, significantly increased in cirrhosis
- No valves - drains spleen, pancreas, gallbladder, and abdominal alimentary tract
- Tributaries: Superior mesenteric vein + splenic vein form the portal vein behind the neck of the pancreas
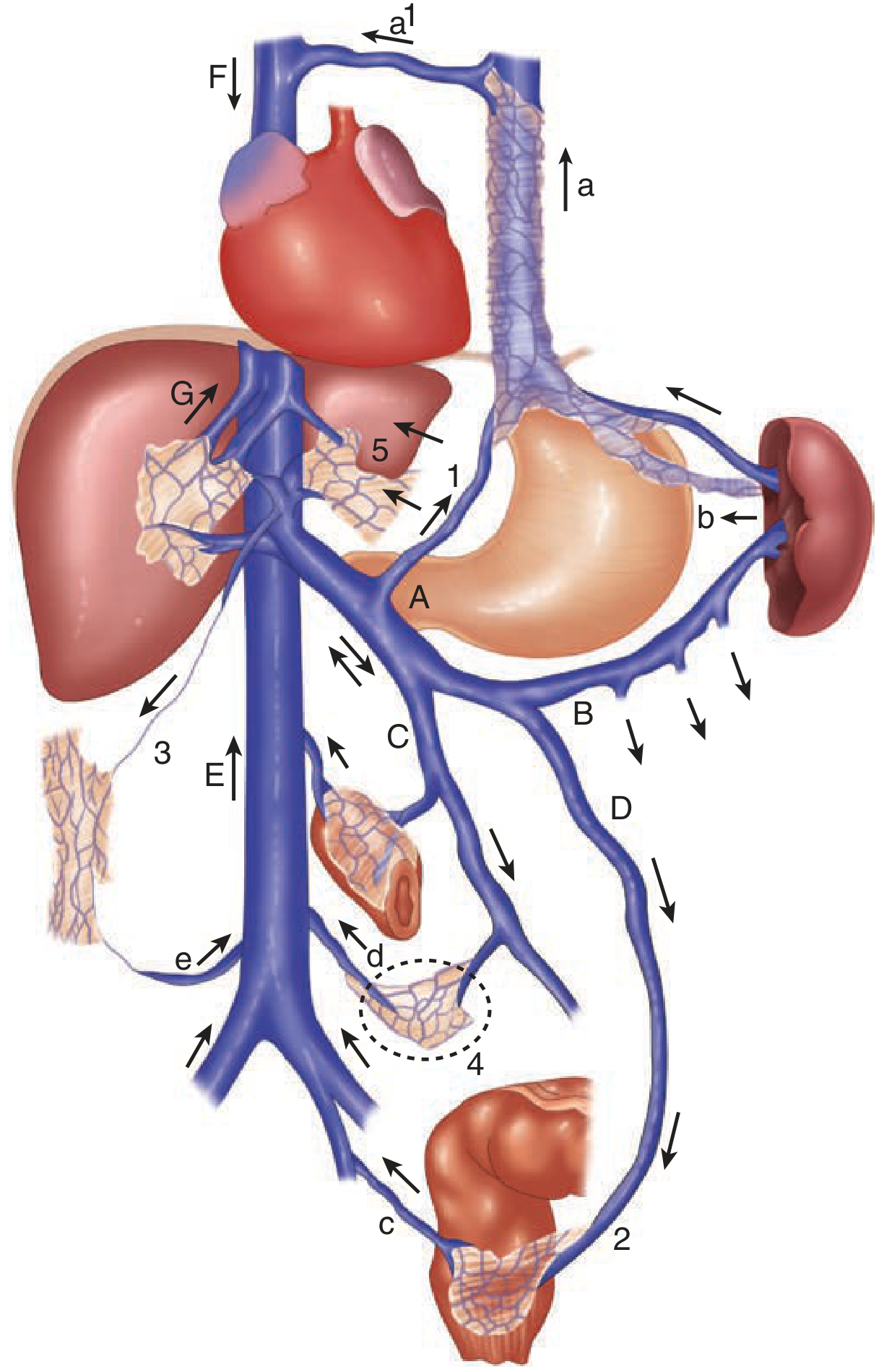
Portosystemic collaterals form at five sites (exam favorite):
| Site | Portal tributary | Systemic tributary | Clinical result |
|---|---|---|---|
| Gastroesophageal junction | Coronary (left gastric) vein | Azygos vein | Esophageal varices |
| Anal canal | Superior rectal (hemorrhoidal) | Middle/inferior rectal | Anorectal varices |
| Falciform ligament | Paraumbilical veins | Epigastric veins | Caput medusae |
| Retroperitoneum | Retzius veins | Lumbar/renal veins | Retroperitoneal varices |
| Splenorenal | Splenic venous bed | Left renal vein | Spontaneous splenorenal shunt |
Note: Hemorrhoids do NOT communicate with the portal system and are not increased in portal hypertension. Anorectal varices (present in ~45% of cirrhotics) must be distinguished from hemorrhoids.
Classification of Causes (Pre-sinusoidal / Sinusoidal / Post-sinusoidal)
Pre-sinusoidal
Extrahepatic:
- Portal vein thrombosis
- Splenic vein thrombosis (pancreatitis, pancreatic tumour) - causes LEFT-SIDED (sinistral) portal hypertension
- Myelofibrosis, tropical splenomegaly, splenic arteriovenous fistula
Intrahepatic:
- Schistosomiasis (most common cause worldwide)
- Congenital hepatic fibrosis
- Nodular regenerative hyperplasia, sarcoidosis, myeloproliferative disorders
- Veno-occlusive disease (sinusoidal obstruction syndrome), drugs/toxins, graft-vs-host disease
Sinusoidal (Intrahepatic)
- Cirrhosis (most common cause in the West/India)
- Alcohol-related liver disease, viral hepatitis (HBV/HCV)
- Primary biliary cholangitis, primary sclerosing cholangitis
- Autoimmune hepatitis, metabolic liver disease (NAFLD/NASH)
Post-sinusoidal
Intrahepatic: Vascular occlusive disease
Extrahepatic (most important):
- Budd-Chiari syndrome (hepatic vein occlusion) - polycythemia vera, essential thrombocythemia, factor V Leiden, OCP use, IVC web
- Congestive cardiac failure / constrictive pericarditis
- Inferior vena caval web
Key exam point: In the West, cirrhosis accounts for the majority of portal hypertension. In India and developing nations, extrahepatic portal venous obstruction (EHPVO) and schistosomiasis are common non-cirrhotic causes.
Measurement of Portal Pressure
Gold standard: Hepatic Venous Pressure Gradient (HVPG)
- Balloon catheter placed in hepatic vein via jugular approach
- FHVP (free hepatic venous pressure) = balloon deflated
- WHVP (wedged hepatic venous pressure) = balloon inflated
- HVPG = WHVP - FHVP
- Normal: <5 mmHg
- Portal hypertension: >5 mmHg
- Clinically significant: >10 mmHg
- Variceal bleeding threshold: >12 mmHg
- Severe (ascites): >12 mmHg
Non-invasive imaging:
- Doppler ultrasound: best initial investigation - shows portal vein patency, thrombosis, direction of flow, collaterals
- CT/MRI angiography: detailed anatomy, patency
- Visceral angiography/venography: reserved for complex cases
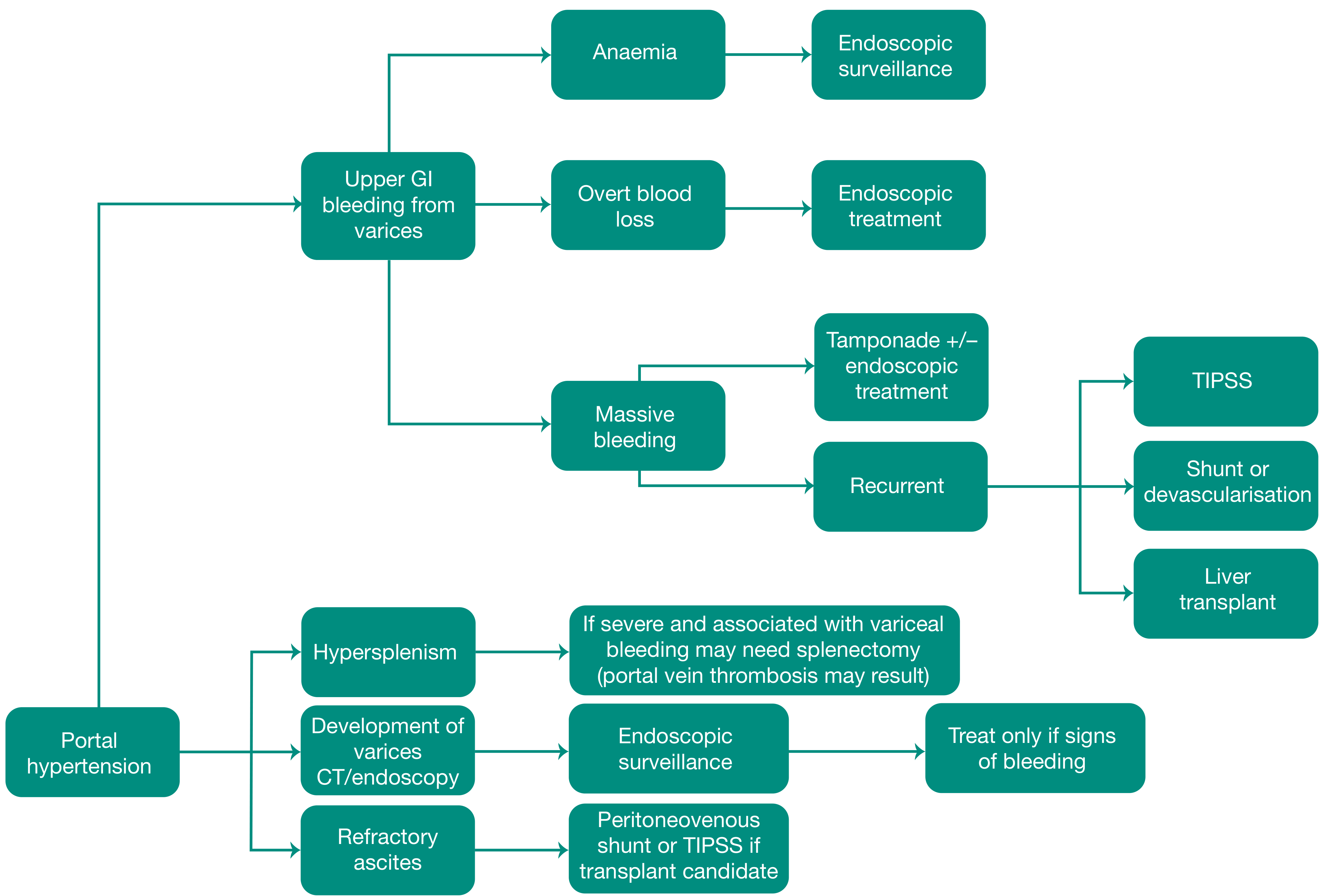
Complications of Portal Hypertension
Surgical involvement occurs in four situations (Bailey & Love):
- Ascites
- Oesophageal/gastric varices
- Portosystemic shunting (for problems not managed by other methods)
- Left-sided portal hypertension and hypersplenism
1. Variceal Bleeding (Most Important)
- ~30% of compensated cirrhotics and 60% of decompensated cirrhotics have esophageal varices
- 1/3 of patients with varices will bleed
- Each episode: 20-30% mortality
- 70% of survivors will re-bleed within 2 years without treatment
2. Splenomegaly & Hypersplenism
- Causes leukopenia, thrombocytopenia, anemia
- Requires treatment if platelet count <50 × 10⁹/L or associated with variceal bleeding
3. Ascites
- Develops due to severe portal hypertension + hepatocyte dysfunction
- May develop spontaneous bacterial peritonitis (SBP)
4. Hepatic Encephalopathy
5. Hepatorenal Syndrome
Assessment of Liver Function - Scoring Systems (High-Yield PG Exam)
Child-Turcotte-Pugh (CTP) Score
| Variable | 1 Point | 2 Points | 3 Points |
|---|---|---|---|
| Bilirubin | <2 mg/dL | 2-3 mg/dL | >3 mg/dL |
| Albumin | >3.5 g/dL | 2.8-3.5 g/dL | <2.8 g/dL |
| INR | <1.7 | 1.7-2.2 | >2.2 |
| Encephalopathy | None | Controlled (Gr 1-2) | Uncontrolled (Gr 3-4) |
| Ascites | None | Slight/controlled | Moderate/uncontrolled |
Class A = 5-6 (mortality 10%), Class B = 7-9 (mortality 30%), Class C = 10-15 (mortality 75-80%)
- Originally developed to evaluate risk of portocaval shunt procedures
- Elective surgery generally NOT considered for Child B or C cirrhosis
- Limitation: includes subjective variables (ascites, encephalopathy); narrow range (5-15)
MELD Score (Model for End-Stage Liver Disease)
- Formula: 3.78[ln bilirubin (mg/dL)] + 11.2[ln INR] + 9.57[ln creatinine (mg/dL)] + 6.43
- Based on three objective values: INR, serum bilirubin, serum creatinine
- Originally developed to predict mortality after TIPS
- Now the primary method of liver transplant allocation
- MELD <16: lower postoperative mortality
- MELD-Na adds sodium as fourth variable (more accurate for ascites patients)
- Largely supplanted CTP for surgical risk stratification
Management of Variceal Bleeding
Step 1: Resuscitation (Immediate)
- Admit to ICU; large-bore IV access (two peripheral lines)
- Blood transfusion to Hb ~8 g/dL - avoid over-transfusion (raises portal pressure, worsens bleeding)
- IV Vitamin K 10 mg; FFP for coagulopathy; platelets if <50 × 10⁹/L
- Prophylactic antibiotics (ceftriaxone 1g/day IV) - reduces infection risk and increases survival
- Endotracheal intubation if encephalopathy present before endoscopy (airway protection)
Step 2: Vasoactive Drugs (Start immediately on clinical suspicion)
- Terlipressin (vasopressin analogue) - first choice; reduces splanchnic blood flow
- Octreotide / Somatostatin (somatostatin analogue) - preferred in many centres; can be given for 5 days; fewer systemic side effects than vasopressin
- Vasopressin - most potent vasoconstrictor; limited by side effects (hypertension, myocardial ischemia, arrhythmias, limb gangrene)
- Non-selective beta-blockers (propranolol/nadolol): reduce index bleed by 45%, bleeding mortality by 50% - used for PRIMARY PROPHYLAXIS, not acute bleeding
Step 3: Endoscopy (as soon as stable)
- Confirms source in 70% (30% will have non-variceal source)
- Oesophageal varices: Endoscopic band ligation (EBL) preferred over sclerotherapy - lower rebleeding rate
- Fundal/gastric varices: Cyanoacrylate (tissue glue) injection; thrombin injection
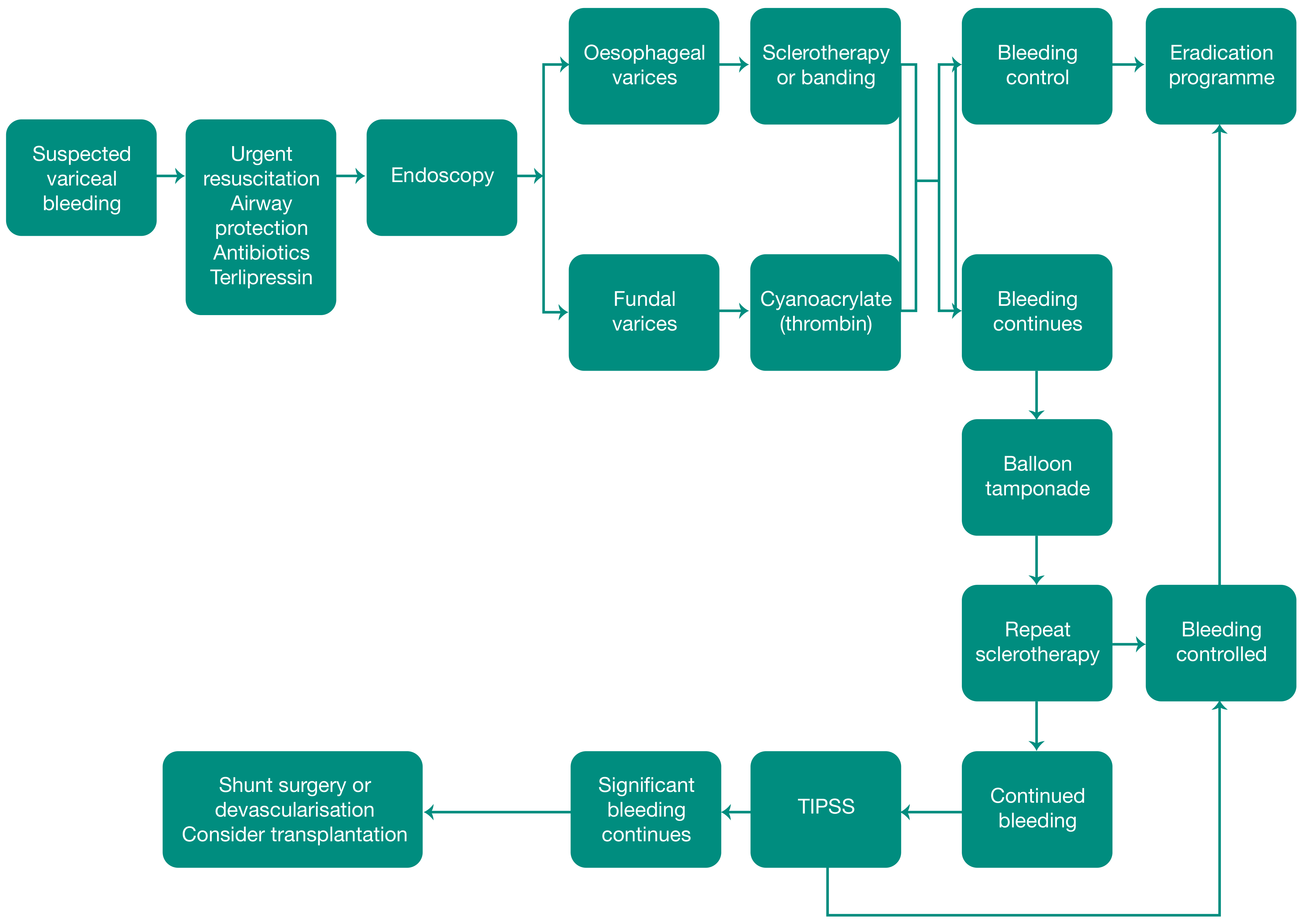
Step 4: Balloon Tamponade (Bridge therapy only)
- Used when endoscopic + pharmacological therapy fails
- Sengstaken-Blakemore (SB) tube - gastric and esophageal balloons
- Minnesota tube - adds a fourth port for esophageal suction
- Controls bleeding in up to 90%, but only temporary bridge
- Complications: aspiration, airway obstruction, esophageal perforation
- CONTRAINDICATION: hiatal hernia, recent esophageal surgery
- Should be replaced within 24-48 hours; max 24 hours recommended
Step 5: TIPSS (Transjugular Intrahepatic Portosystemic Stent Shunt)
- Has replaced surgical portocaval shunt as preferred method for refractory portal hypertension
- First described in 1969; widely available since 1985 with endovascular stents
- Technique: Via internal jugular vein → superior vena cava → hepatic vein → guidewire through hepatic parenchyma into portal vein branch → tract dilated → metallic stent inserted
- Creates a channel between portal vein and hepatic vein
- Performed under local anaesthetic with fluoroscopic + US guidance
- Complications:
- Early: liver capsule perforation with fatal intraperitoneal haemorrhage
- Stent occlusion (more common with good hepatic synthetic function)
- Post-TIPSS encephalopathy in 40% (comparable to surgical shunts) - due to portal blood bypassing hepatic detoxification
- If severe encephalopathy: flow in stent is reduced (flow-restricting device inserted)
- Preferred over surgical shunts in transplant candidates (easier subsequent transplant)
Step 6: Surgery
- Failure to control bleeding with medical management: 10-20% of cases
- Options: portosystemic shunts, devascularisation procedures
Surgical Portosystemic Shunts (High-Yield)
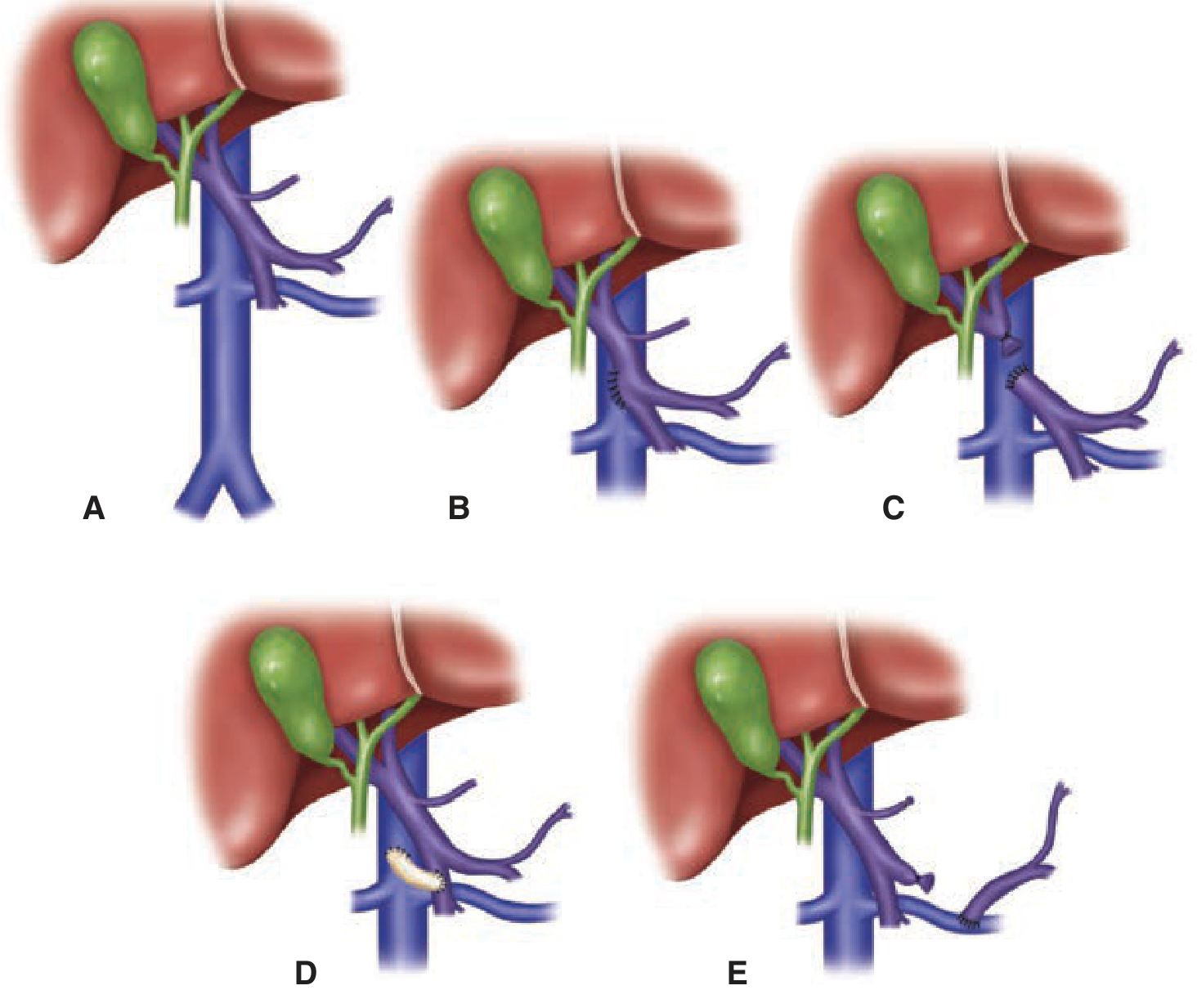
Classification of Shunts
| Type | Shunt | Notes |
|---|---|---|
| Non-selective (total) | End-to-side portacaval shunt | Portal vein completely diverted; abolishes hepatic portal flow; high encephalopathy |
| Non-selective (total) | Side-to-side portacaval shunt | Decompresses both portal system AND sinusoids; good for ascites; high encephalopathy |
| Non-selective (total) | Mesocaval (H-graft) shunt | Interposition graft between SMV and IVC |
| Selective (partial) | Distal splenorenal shunt (Warren shunt) | Selective decompression of gastroesophageal varices via splenorenal anastomosis while preserving hepatoportal blood flow; lower encephalopathy; preferred when transplant not planned |
| Partial | Central splenorenal shunt | Spleen removed; central end of splenic vein to left renal vein |
Key points on shunts:
- Selective shunts (Warren) - lower incidence of encephalopathy; preserve hepatic blood flow
- No evidence prophylactic shunting is beneficial
- Previous surgical shunts increase complexity and morbidity of liver transplantation
- TIPSS should be preferred over surgical shunts in transplant candidates
Devascularisation Procedures
Sugiura Procedure (for refractory esophageal varices)
- Combines splenectomy with oesophagogastric devascularisation
- Permanently interrupts intraoesophageal portacaval shunt while preserving perioesophageal varices
- Devascularisation of both lesser and greater curves of upper stomach
- 8-10 cm of oesophagus cleared
- Oesophageal transection with large stapler just above cardia
- Preserves collateral channels and vagus nerve
Management of Ascites in Portal Hypertension
- CT confirms aetiology (irregular shrunken cirrhotic liver, portal hypertension, splenomegaly)
- IV contrast demonstrates abdominal varices and portal vein patency
- SAAG (Serum-Ascites Albumin Gradient) >1.1 g/dL = portal hypertension
- Protein content distinguishes causes: cardiac ascites (high protein) vs cirrhotic (low protein)
Management:
- Salt restriction + diuretics (spironolactone ± furosemide)
- Therapeutic paracentesis + albumin replacement
- Refractory ascites: Peritoneovenous shunt (LeVeen shunt) or TIPSS (if transplant candidate)
- Ultimately: Liver transplantation
Budd-Chiari Syndrome (Post-sinusoidal Portal Hypertension)
- Hepatic vein obstruction → hepatomegaly, liver congestion, RUQ pain
- Causes: Polycythemia vera (35-50% of primary cases), essential thrombocythemia, factor V Leiden (25%), anticardiolipin antibodies, oral contraceptives, hyperhomocysteinemia
- Caudate lobe hypertrophy in ~50% (direct venous drainage into IVC is preserved)
- 70% have centrilobular necrosis on biopsy
- Diagnosis: Abdominal US + Doppler first; CT/MRI; definitive = hepatic venography
- Treatment: Anticoagulation + treat underlying condition → angioplasty/TIPS + thrombolytics → surgical shunt → liver transplantation
Primary Prophylaxis of Variceal Bleeding
- Non-selective β-blockers (propranolol/nadolol): reduce index bleed by 45%, mortality by 50%
- ~20% do not respond; ~20% cannot tolerate
- Endoscopic band ligation (EBL): recommended for medium-to-large varices
- Every 1-2 weeks until obliteration
- EGD 1-3 months later, then surveillance every 6 months
Key PG Exam "One-Liners"
| Fact | Answer |
|---|---|
| Normal portal pressure | 5-10 mmHg |
| HVPG threshold for varices to bleed | >12 mmHg |
| Most common cause of portal HTN worldwide | Schistosomiasis |
| Most common cause in West/India (clinically) | Cirrhosis |
| Left-sided portal hypertension cause | Splenic vein thrombosis |
| Best initial investigation | Doppler ultrasound |
| Gold standard for measuring portal pressure | HVPG (hepatic venography) |
| Most common site of variceal bleeding | Lower oesophagus |
| Acute variceal bleed mortality per episode | 20-30% |
| Drug of choice - acute variceal bleeding | Terlipressin (or octreotide) |
| Gastric fundal varices: treatment | Cyanoacrylate injection |
| Balloon for refractory bleeding | Sengstaken-Blakemore tube |
| TIPSS encephalopathy rate | ~40% |
| Selective shunt (preserves hepatic flow) | Warren (distal splenorenal) shunt |
| Shunt not suitable before transplantation | Surgical shunts (prefer TIPSS) |
| CTP class A operative mortality | ~10% |
| CTP class C operative mortality | 75-80% |
| Budd-Chiari: characteristic finding | Caudate lobe hypertrophy |
| MELD uses which variables | Bilirubin, INR, Creatinine (+ Na for MELD-Na) |
| Caput medusae: which vein recanalises | Paraumbilical vein (falciform ligament) |
| Hemorrhoids vs anorectal varices | Varices communicate with portal system; hemorrhoids do NOT |
| Sugiura procedure combines | Splenectomy + esophagogastric devascularisation |
| Definitive treatment of portal hypertension | Liver transplantation |
Bailey and Love's Short Practice of Surgery, 28th ed. | Schwartz's Principles of Surgery, 11th ed. | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.