teach mebasal ganglia..parts, functions, lesions, diseases, and everything related to it in a simplified way that i can remember in a 20 marks shortnote...combine your information with this ppt too..but make is easy and simplified
Reading File
Reading File
Running Command
Finding Sources
Running Command
Reading File
Reading File
Running Command
Reading File
Reading File
Loading Image
Loading Image
I now have everything I need. Here is your complete, simplified 20-mark short note on Basal Ganglia, fully combining your PPT with authoritative textbook content.
🧠 BASAL GANGLIA - Complete Short Note (20 Marks)
1. DEFINITION
The basal ganglia are large masses of grey matter situated deep within the white core of each cerebral hemisphere. They are a collection of subcortical nuclei concerned with planning and organization of voluntary movement through feedback circuits to the motor and premotor cortex. They form essential constituents of the extrapyramidal system and are derived from the telencephalon (except globus pallidus, which is diencephalic in origin).
2. COMPONENTS - "CSGS + SN" (Easy Memory Trick)
Key Groupings to Remember:
| Group Name | What's In It |
|---|---|
| Striatum (Neostriatum) | Caudate nucleus + Putamen |
| Lentiform nucleus | Putamen + Globus pallidus |
| Corpus striatum | Caudate + Putamen + Globus pallidus |
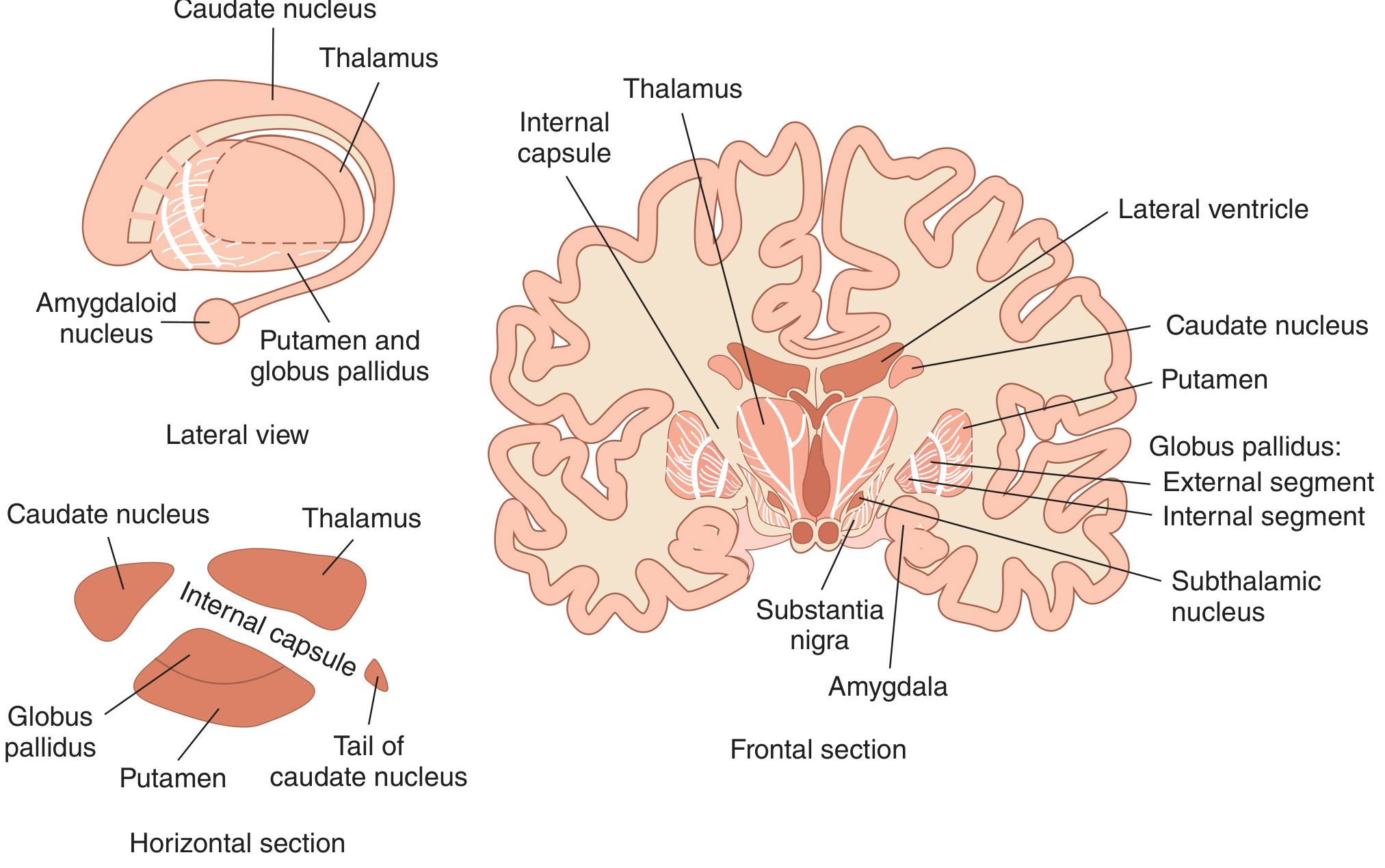
The 5 Core Structures:
1. Caudate Nucleus - C-shaped structure; 3 parts:
- Head - near frontal horn of lateral ventricle; receives input from prefrontal cortex; involved in executive functions, decision-making
- Body - sensorimotor control and spatial integration
- Tail - curves near amygdala; involved in emotional processing and memory
2. Putamen - Round, shell-like; lateral to globus pallidus; forms striatum with caudate. Key for motor planning and execution. Receives excitatory (glutamate) input from cortex and dopaminergic input from substantia nigra.
3. Globus Pallidus (GP) - Inner component of lentiform nucleus; uses GABA as neurotransmitter:
- GPe (External) - modulates the indirect pathway
- GPi (Internal) - major OUTPUT of basal ganglia; sends inhibitory signals to thalamus
4. Subthalamic Nucleus (STN) - Small but vital; uses glutamate (excitatory); modulates motor, cognitive, and emotional circuits. Damage → Hemiballismus
5. Substantia Nigra (SN) - Located in the midbrain:
- Pars Compacta (SNc) - dopaminergic neurons; projects to striatum via the nigrostriatal pathway
- Pars Reticulata (SNr) - GABAergic neurons; acts as an output nucleus (like GPi)
Bonus: Ventral Striatum - Nucleus accumbens + olfactory tubercle; part of limbic system; associated with reward, motivation, and addiction
3. INPUTS TO BASAL GANGLIA (3 main afferents)
All inputs terminate in the Striatum (the major recipient):
| Pathway | From | Neurotransmitter | Function |
|---|---|---|---|
| Corticostriatal | Neocortex (layers V & VI) | Glutamate (excitatory) | Primary input; motor, cognitive, emotional control |
| Nigrostriatal | SNc | Dopamine | Modulates striatal activity; degeneration → Parkinson's |
| Thalamostriatal | Intralaminar nuclei (central median nucleus) | Glutamate | Learning, memory, and action |
4. INTERNAL CIRCUITS - Direct vs Indirect Pathway
This is the most important concept. Think of it as a "gas pedal vs brakes" system for movement.
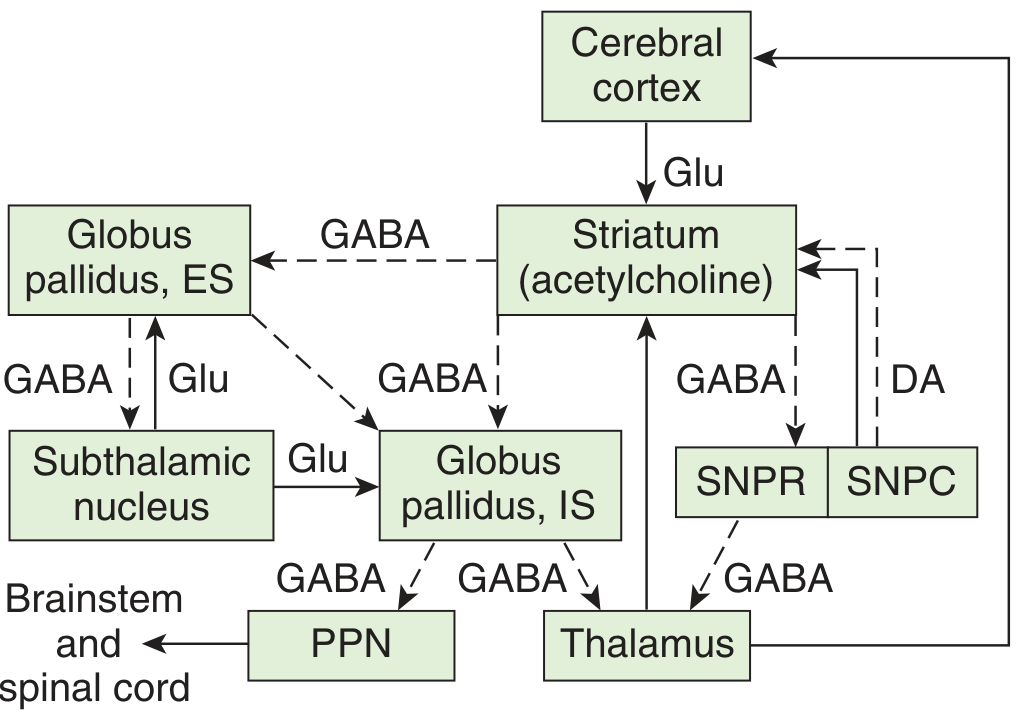
DIRECT PATHWAY = "GO" pathway (promotes movement)
Cortex (Glu↑) → Striatum → GPi/SNr (GABA inhibits GPi) → Thalamus less inhibited →
Cortex excited → MORE MOVEMENT
- Striatal neurons here contain Substance P + D1 receptors
- Dopamine (D1) = EXCITES direct pathway → promotes movement
- Net effect: Excitatory on motor cortex
INDIRECT PATHWAY = "STOP" pathway (suppresses movement)
Cortex (Glu↑) → Striatum → GPe (GABA inhibits GPe) → STN less inhibited →
STN excites GPi (Glu↑) → GPi inhibits Thalamus more → LESS MOVEMENT
- Striatal neurons here contain Enkephalin + D2 receptors
- Dopamine (D2) = INHIBITS indirect pathway → promotes movement
- Net effect: Inhibitory on motor cortex
Key rule: Direct and indirect pathways are equal and opposite. Any imbalance = movement disorder.
Memory trick for dopamine effect:
"D1 = Direct = Do it! D2 = indirect = Don't (inhibit it)!" Both D1 and D2 stimulation ultimately promotes movement - dopamine is pro-movement overall.
5. OUTPUT OF BASAL GANGLIA
- Main output: GPi (most) + SNr → to Ventral Lateral (VL) and Ventral Anterior (VA) thalamic nuclei → Premotor cortex + Prefrontal cortex → Primary motor cortex
- Output uses GABA (inhibitory)
- GPi also projects to brainstem → motor neurons via PPN (pedunculopontine nucleus)
- Key concept: Cortex inputs excite → back-to-back inhibitions within BG → final result is disinhibition of thalamus/cortex
6. FUNCTIONS OF BASAL GANGLIA
| Domain | Function |
|---|---|
| Motor | Planning, programming, initiation of voluntary movement; postural control and muscle tone; filtering out unnecessary movements |
| Cognitive | Executive functions (caudate nucleus particularly); procedural learning and habit formation; working memory |
| Emotional | Emotional regulation; interface with limbic system via nucleus accumbens and amygdala |
| Behavioral | Reward and addiction (nucleus accumbens); language; decision-making |
7. INVOLUNTARY MOVEMENTS WITH BASAL GANGLIA DAMAGE
| Movement | Character | Lesion Site |
|---|---|---|
| Tremor | Rhythmic; resting tremor (pill-rolling) | Dopamine loss (SN) |
| Chorea | Random, quick, jerky, purposeless "dancing" movements | Caudate nucleus damage |
| Athetosis | Slow, continuous writhing movements; affects arms/hands | Striatum |
| Ballism/Hemiballismus | Violent, flinging, involuntary movements of one arm/leg (contralateral to lesion) | Subthalamic nucleus (usually stroke) |
| Dystonia | Slow, sustained, twisting contractions; abnormal postures | Extrapyramidal pathways |
| Tics | Uncontrollable repeated movements or vocalizations | Striatum/GP dysregulation |
Hyperkinetic disorders (too much movement): Chorea, athetosis, ballism, tics, dystonia Hypokinetic disorders (too little movement): Akinesia, bradykinesia (Parkinson's)
8. DISEASES OF THE BASAL GANGLIA
A. PARKINSON'S DISEASE
- Most common BG disorder
- Pathology: Loss of dopaminergic neurons in SNc → reduced dopamine in striatum → indirect pathway overactive, direct pathway underactive → LESS movement
- Features (TRAP): resting Tremor (pill-rolling), Rigidity (cogwheel), Akinesia/Bradykinesia, Postural instability; shuffling gait
- Treatment: L-DOPA (dopamine precursor), dopamine agonists (bromocriptine), Deep Brain Stimulation (DBS) of STN or GPi
B. HUNTINGTON'S DISEASE
- Pathology: Autosomal dominant; CAG trinucleotide repeat expansion in IT15 gene on chromosome 4; destroys striatal GABAergic neurons and cortical cholinergic neurons
- Features: Chorea + Athetosis + Dystonia; personality change; psychiatric disorder; dementia; onset 35-50 years
- Mechanism: Loss of indirect pathway inhibition → STN disinhibited → less GPi output → thalamus over-excited → excess movement
- No cure available
C. HEMIBALLISMUS
- Pathology: Subthalamic nucleus lesion (usually stroke)
- Features: Violent, flinging movements of contralateral arm/leg
- Mechanism: Loss of STN → less GPi activation → thalamus over-active → excessive involuntary movement
D. WILSON'S DISEASE (Hepatolenticular Degeneration)
- Pathology: Autosomal recessive; defective ATP7B gene on chromosome 13 → copper accumulates in liver, brain (especially lenticular nuclei), and eyes (Kayser-Fleischer rings)
- Features: Rigidity, dystonia, chorea, athetosis, dysarthria, tremor; psychiatric disturbances in ~50%
E. FAHR'S DISEASE
- Pathology: Idiopathic bilateral calcification of basal ganglia; autosomal dominant
- Features: Parkinsonism, dystonia, tremors; psychiatric (depression, psychosis); seizures
- Age pattern: 20-40 yrs → schizophreniform/catatonic; 40-60 yrs → dementia and choreoathetosis
F. PROGRESSIVE SUPRANUCLEAR PALSY (PSP)
- Pathology: Degenerative; affects SN, striatum, thalamus, subthalamus, brainstem nuclei
- Deficits: Dopamine (nigrostriatal) and acetylcholine
- Features: Cognitive impairment in 80%; vertical gaze palsy; Parkinsonism features
G. TOURETTE'S SYNDROME
- Pathology: Dysregulation in basal ganglia circuits (striatum and GP); onset before 18 years
- Features: Multiple motor tics + vocal (phonic) tics, waxing and waning; associated with OCD, ADHD, anxiety
9. PSYCHIATRIC DISORDERS LINKED TO BASAL GANGLIA
| Disorder | Basal Ganglia Involvement |
|---|---|
| OCD | Overactivity of CSTC loop (Orbitofrontal cortex-Striatum-Thalamus-Cortex); hyperactivity of caudate nucleus |
| Schizophrenia | Dysregulation of dopamine in nigrostriatal + mesolimbic pathways; caudate-putamen volume increase |
| Depression | Reduced activity in ventral striatum (reward processing) → anhedonia, psychomotor retardation |
| Addiction | Nucleus accumbens (reward) + dorsal striatum (habit formation) are key; dopamine drives craving |
| ADHD | Structural/functional changes in striatum; volume compression in caudate head/body and anterior putamen |
| Autism | Altered cell density in BG nuclei; disruption of normal motor feedback to cortex |
10. QUICK MEMORY SUMMARY TABLE
| Structure | Key Neurotransmitter | Key Function | Lesion Effect |
|---|---|---|---|
| Striatum (Caudate+Putamen) | GABA (medium spiny neurons); ACh interneurons | Input station | Chorea (Huntington) |
| GPe | GABA | Indirect pathway modulation | Hemiballismus (via STN) |
| GPi | GABA | MAIN OUTPUT to thalamus | Parkinsonism if overactive |
| STN | Glutamate | Excites GPi; controls movement | Hemiballismus if damaged |
| SNc | Dopamine | Nigrostriatal pathway; modulates striatum | Parkinson's disease |
| SNr | GABA | Output nucleus (like GPi) | Motor rigidity |
| Nucleus Accumbens | Dopamine | Reward, motivation | Addiction, depression |
FINAL EXAM MNEMONIC
"CAPS SN" = Caudate + Accumbens (ventral striatum) + Putamen + Subthalamic + Substantia Nigra + Globus pallidus
For pathways: Think "D = Direct = DO move" and "I = Indirect = INHIBIT movement"
For diseases: Think PHWFT = Parkinson, Huntington, Wilson, Fahr, Tourette
Sources: Ganong's Review of Medical Physiology (26th Ed.), Neuroanatomy through Clinical Cases (3rd Ed.), Kaplan & Sadock's Comprehensive Textbook of Psychiatry (10th Ed.), Costanzo Physiology (7th Ed.), and your PPT (Dr. HRIM Shah, SBKS MI&RC)
This is a shared conversation. Sign in to Orris to start your own chat.