



What to with this patient for prostate as it cause difficulty in urination and may future it can also grow and patient may unable to do urination
"prostate cancer" AND "urinary obstruction" AND (TURP OR "hormonal therapy" OR "androgen deprivation")
"prostate cancer" AND "bone metastasis" AND "androgen deprivation therapy"
"prostate cancer" AND "Gleason" AND (TURP OR "lower urinary tract symptoms" OR "urinary retention")
Patient Summary: Revabhai Koyabhai Patel, Male, 76 Years
What the Reports Show
- Prostate: enlarged at 52x47x52 mm (70 gm) - significantly enlarged (normal is ~20 gm)
- Bladder wall: mildly thickened and trabeculated - sign of chronic outlet obstruction
- Pre-void bladder volume: 354 cc
- Post-void residual (PVR) urine: 241 cc - significant (normal < 50 cc)
- No hydronephrosis yet, kidneys normal
- Incidental finding: reducible epigastric hernia (21x19 mm)
- 12 cores taken from both lobes
- RL1 (Right lower lobe): Prostatic Acinar Adenocarcinoma, Gleason 3+3=6, Grade Group 1, ~40% tumor in core, no perineural invasion
- LU2 (Left upper lobe): Prostatic Acinar Adenocarcinoma, Gleason 3+3=6, Grade Group 1, ~20% tumor in core, no perineural invasion
- Other cores: normal prostatic tissue, atypical acinar gland proliferation (ASAP), or chronic prostatitis
- Diagnosis: Low-grade prostate adenocarcinoma (Grade Group 1) in 2 out of 12 cores
- Prostate: 37x45x46 mm with PSMA-expressive lesion in central and left half - consistent with primary malignant lesion
- Bony Metastases confirmed:
- PSMA-expressive sclerotic lesions in left half of body and spinous process of D12 vertebra, and sternal body
- SUVmax at D12 spinous process: 18.8, sternum: 3.7
- No regional lymph node involvement
- No visceral metastases
- Bladder changes: mild cystitis, small bladder diverticulum
Staging
Management Approach
1. URINARY OBSTRUCTION - URGENT PRIORITY
- Acute urinary retention
- Recurrent UTIs
- Bladder decompensation (trabeculation already present)
- Upper tract damage (hydroureteronephrosis)
| Option | Detail |
|---|---|
| Alpha-1 blockers (Tamsulosin 0.4 mg OD or Silodosin) | First-line for LUTS/BPO relief. Relax prostate/bladder neck smooth muscle. Can give symptomatic relief within days. |
| 5-alpha reductase inhibitors (Finasteride or Dutasteride) | Shrink prostate over 3-6 months. Often combined with alpha blocker. |
| TURP (Transurethral Resection of Prostate) | Gold standard if medical therapy fails or retention is imminent. Also palliative for obstruction in prostate cancer. Safe even in metastatic disease for urinary decompression. |
| Urethral catheterization | If acute retention occurs - insert Foley catheter immediately and assess bladder recovery. |
Note: Androgen Deprivation Therapy (ADT) itself will shrink the prostate over weeks to months, which will also improve urinary flow as a secondary benefit.
2. SYSTEMIC TREATMENT FOR METASTATIC PROSTATE CANCER
- Surgical: Bilateral orchiectomy - permanent, cheap, reliable castration
- Medical (preferred): GnRH agonists (Leuprolide, Goserelin, Triptorelin) or GnRH antagonists (Degarelix, Relugolix)
- Important: When starting GnRH agonists, co-administer an antiandrogen (Bicalutamide 50 mg) for at least 4 weeks to prevent testosterone flare, which can worsen bone pain or spinal cord symptoms
- GnRH antagonists (Degarelix, Relugolix) do NOT cause flare and are preferred in patients with painful bone disease
| Agent | Role |
|---|---|
| Abiraterone + Prednisone | Blocks adrenal androgen synthesis. Significantly improves overall survival when added to ADT. |
| Enzalutamide or Apalutamide or Darolutamide | Next-gen androgen receptor blockers. Added to ADT in mHSPC. |
| Docetaxel (chemotherapy) | For high-volume disease or fit patients. Extends median survival ~17 months when added to ADT in high-volume disease. |
3. BONE METASTASIS MANAGEMENT
-
Bone-protecting agents:
- Zoledronic acid (IV) or Denosumab (SC) - reduce skeletal-related events (fractures, pain, spinal cord compression)
- Monitor calcium and renal function before dosing
- Dental check before starting (osteonecrosis of jaw risk)
-
Radium-223: FDA-approved for symptomatic bone metastases in castration-resistant disease. Not yet indicated at this stage but relevant if disease progresses.
-
Pain management: If D12 spine lesion causes pain - analgesia (NSAIDs, opioids), and/or targeted radiation to the D12 site.
-
Spinal surveillance: D12 vertebral involvement needs monitoring. Neurosurgery/spine team consultation if any signs of cord compression (back pain, weakness, bowel/bladder dysfunction changes).
4. MONITORING
| Parameter | Frequency |
|---|---|
| PSA | Every 3 months initially |
| Testosterone | Every 3-6 months (confirm castration level <50 ng/dL) |
| Bone scan or PSMA PET | Every 6-12 months or if symptoms |
| Renal function, CBC, LFTs | Every 3 months (especially if on abiraterone) |
| Post-void residual urine | At each urology visit |
| Bone mineral density (DEXA) | Baseline then annually (ADT causes osteoporosis) |
5. ADDITIONAL FINDINGS TO ADDRESS
- Epigastric hernia (21x19 mm, reducible): Non-urgent but should be referred to general surgery for elective repair when the patient is medically stable.
- Bladder diverticulum (small, anterosuperior wall): Monitor; may enlarge with continued obstruction.
- Chronic prostatitis changes (RL2): Not requiring separate treatment.
- ASAP (atypical acinar proliferation) in multiple cores: Indicates field effect; ongoing biopsy surveillance may be recommended.
Summary of Immediate Action Plan
- Start Tamsulosin 0.4 mg at night - for urinary symptoms right away
- Refer to urologist - assess need for TURP given PVR 241 cc
- Start ADT (Leuprolide/Goserelin + Bicalutamide cover, or Degarelix directly) - under medical oncology/urology supervision
- Add Abiraterone or Enzalutamide to ADT as per oncologist
- Start Zoledronic acid for bone protection
- Radiation oncology consult for D12 vertebral lesion if symptomatic
- Spine monitoring - urgent MRI spine if any neurological symptoms develop
- Germline genetic testing recommended for metastatic prostate cancer (BRCA2 mutations alter therapy choices)
Disclaimer: This analysis is for educational/informational purposes. All treatment decisions must be made by the patient's treating urologist and medical oncologist after full clinical assessment. This patient needs urgent multidisciplinary care.
How to regain normal urination
"prostate cancer" AND "urinary symptoms" AND (TURP OR "alpha blocker" OR ADT)
PMID: 40402299
How to Regain Normal Urination - Revabhai Patel, 76M
- The prostate (70 gm, PSMA-positive cancer) is physically squeezing the urethra shut from outside
- The bladder is already damaged - trabeculated wall + PVR 241 cc means the bladder muscle has been straining for months/years and is now weak
STEP 1 - Start Medications Immediately (This Week)
Alpha-1 Blocker - First Priority
- Relaxes smooth muscle in the bladder neck and prostate urethra within 24-48 hours
- Reduces the squeezing pressure on the urethra
- Improves urine flow rate and reduces straining
- Main side effects: Dizziness when standing (take at night), retrograde ejaculation
5-Alpha Reductase Inhibitor - To Shrink the Prostate
- Blocks conversion of testosterone to DHT inside the prostate
- Physically shrinks prostate volume by 20-30% over 3-6 months
- Works slowly - improvement takes 3-6 months but is sustained
- Important note: These drugs reduce PSA by ~50%, so tell the oncologist so they can adjust interpretation
Combination is Better Than Either Alone
However, in this patient with confirmed cancer and bone metastases: The 5-ARI may need to be held depending on oncologist decision, since ADT (which will be started for cancer) will do the same thing - shrink the prostate by dropping testosterone.
STEP 2 - Androgen Deprivation Therapy (ADT) Will Help Urination Too
- Shrink the prostate by 30-50% over 3-6 months
- Directly relieve the urethral compression
- Reduce the LUTS (hesitancy, weak stream, incomplete emptying)
STEP 3 - TURP (Surgery) if Medications Are Not Enough
When TURP is needed:
- PVR stays above 150-200 cc despite 4-6 weeks of medication
- Acute urinary retention (completely unable to urinate)
- Recurrent UTIs from stagnant urine
- Bladder stone formation
- Worsening kidney function (creatinine rising)
What TURP does:
Evidence for palliative TURP in prostate cancer with metastases:
- PVR reduced by mean 50 cc (significant improvement)
- Symptom score improved by 14 points (very significant)
- Safe to do even with bone metastases
- Complications to be aware of: need for repeat TURP (23%), incontinence (14%), continued catheter need (11%)
Modern TURP options (laser is better for elderly):
| Procedure | Notes |
|---|---|
| HoLEP (Holmium Laser Enucleation) | Best for large prostates like this 70 gm one. Less bleeding, faster recovery |
| Bipolar TURP | Safer than old monopolar TURP - uses saline, no electrolyte imbalance risk |
| Standard TURP | Still widely used, good outcomes |
STEP 4 - If Acute Retention Happens Before Surgery
- Go to emergency immediately
- A Foley catheter will be inserted through the urethra to drain the bladder
- Keep catheter for 5-7 days to rest the bladder
- Trial of voiding after removing catheter
- If still cannot void - Clean Intermittent Self-Catheterization (CISC) or proceed to TURP
STEP 5 - Bladder Rehabilitation After Obstruction is Relieved
Bladder Training Exercises
- Timed voiding: Urinate every 2-3 hours by schedule, not just when desperate
- Double voiding: After finishing urination, wait 1-2 minutes, then try again to push out the residual urine
- Pelvic floor exercises (Kegel): Tighten the pelvic floor muscles (as if stopping urine midstream), hold 5 seconds, release. Repeat 10 times, 3 sets daily - strengthens bladder control
Fluid Management
- Drink 1.5-2 liters of water daily - spread throughout the day, not in large gulps
- Reduce fluids 2 hours before bedtime to decrease nighttime waking (nocturia)
- Avoid: caffeine (tea, coffee), alcohol, fizzy drinks - all irritate the bladder
What to Avoid
- Do NOT hold urine for long periods (damages bladder further)
- Do NOT push/strain to urinate (can worsen bladder neck dysfunction)
- Avoid constipation (full bowel presses on bladder) - eat fiber, stay active
STEP 6 - Monitoring Progress
| Test | Target | When to Check |
|---|---|---|
| Post-void residual (PVR) | < 50 cc | Every 4-6 weeks |
| Urine flow rate (uroflowmetry) | Peak flow > 15 mL/sec | At urology visit |
| IPSS symptom score | Score < 8 (mild) | Every visit |
| Creatinine | Stable/normal | Every 3 months |
| PSA | Falling (response to ADT) | Every 3 months |
Realistic Expectations for This Patient
| Timeline | What to Expect |
|---|---|
| 24-72 hours after starting Tamsulosin | Easier urine flow, less hesitancy |
| 4-6 weeks of ADT | Prostate begins to shrink, further improvement |
| 3-6 months of ADT | Prostate significantly smaller, best medical response |
| After TURP (if needed) | Dramatic improvement within 1-2 weeks; most patients void freely |
| Bladder recovery | May take 3-12 months for trabeculated bladder to regain normal capacity |
Honest note: Because the bladder wall is already thickened/trabeculated and PVR is 241 cc, this patient may not achieve completely "normal" urination even after perfect treatment. The goal is functional urination with PVR below 100 cc, a good stream, and no pain/infections. This is very achievable with proper management.
How bad can happen in d12 and it's progress and worsening scenario
"spinal cord compression" AND "prostate cancer" AND "vertebral metastasis"
"metastatic spinal cord compression" AND "prostate cancer" AND treatment
The D12 Vertebral Metastasis - Full Progression and Worsening Scenarios
Why D12 is a Particularly Dangerous Location
- The spinal cord ends at approximately L1-L2 (the conus medullaris). D12 is right above this. Any cord compression here affects the most distal spinal cord and the beginning of the cauda equina simultaneously
- It is a transition zone between the rigid thoracic spine and the mobile lumbar spine, making it prone to mechanical failure and fracture
- This patient's lesion has SUVmax 18.8 - extremely high PSMA activity, indicating very metabolically active, aggressive tumor involvement
Stage-by-Stage Progression: From Current State to Worst Case
Stage 1 - Current State (Where patient is NOW)
- Tumor cells have seeded the vertebral bone via blood
- The spinous process is currently involved (the bony projection at the back of the vertebra)
- Sclerotic = bone-hardening response to tumor (typical of prostate cancer metastases)
- Symptoms at this stage: Mid-back pain, pain worse at night or when lying flat, pain that does NOT improve with rest (unlike disc pain), tenderness when you press on the D12 spine
- Radicular pain may begin - band-like tightening sensation around the lower chest/abdomen
Stage 2 - Vertebral Body Involvement and Expanding Tumor Mass
- The tumor enlarges and invades more of the D12 vertebra
- The pedicles (small bony bridges connecting the vertebral body to the posterior elements) erode - visible on X-ray as the "winking owl" sign
- Symptoms worsening:
- Back pain becomes constant and severe
- Pain radiates around the abdomen/lower chest in a band (T12 dermatome = lower abdomen, groin)
- Pain sharply worsens with coughing, sneezing, or straining (Valsalva maneuver)
- Pain is worst at night lying down - this is a key warning sign distinguishing metastatic pain from normal back pain
Stage 3 - Epidural Extension and Spinal Cord/Cauda Equina Compression
- The distal spinal cord (conus medullaris) - controls bladder, bowel, lower limb motor/sensation
- The upper cauda equina roots - L1, L2, L3 nerve roots
- Leg weakness starting (difficulty climbing stairs, getting up from chair)
- Numbness/tingling in the legs, inner thighs, groin, or perineum
- Feeling of "tight band" around the abdomen at the T12 level
- Lhermitte's sign: electric shock sensation shooting down the spine when bending the neck
Stage 4 - Cauda Equina Syndrome (MEDICAL EMERGENCY)
- Saddle anesthesia - numbness of the inner thighs, perineum, buttocks (the area that touches a saddle)
- Bilateral leg weakness - patient struggles to walk, may fall
- Bowel dysfunction - loss of urge to defecate, constipation, or fecal incontinence
- Bladder dysfunction - already has urinary retention (PVR 241 cc); this will dramatically worsen - complete retention, overflow incontinence, or paradoxical incontinence
- Sexual dysfunction - loss of erection/sensation
- Loss of anal and bulbocavernosus reflexes on examination
Stage 5 - Pathological Fracture and Complete Paralysis
- Sudden onset of severe back pain (often described like being stabbed or hit in the back)
- Can cause complete paraplegia (paralysis of both legs) within hours
- Loss of all bladder and bowel control permanently
- Loss of all sensation below T12 level
- This can happen from a trivial event - bending over, a mild fall, even a cough - because the bone structure is already weakened
The D12 Dermatome Map - What Gets Affected
| Structure Compressed | What it Controls | Symptom When Damaged |
|---|---|---|
| T12 nerve root | Skin over lower abdomen, groin | Pain/numbness in lower abdomen and groin |
| L1 nerve root | Upper inner thigh, inguinal region | Pain shooting to groin, hip flexor weakness |
| Conus medullaris | Bladder, bowel, genital sphincters | Retention, incontinence, impotence |
| L2-L3 nerve roots | Hip flexion, knee extension, anterior thigh sensation | Difficulty lifting the leg, knee giving way |
Warning Signs That Mean GO TO HOSPITAL IMMEDIATELY
- Back pain suddenly much worse - especially at night or lying down
- Any new leg weakness - difficulty walking, stumbling
- Numbness in legs, inner thighs, groin, or perineum
- Cannot urinate at all (beyond current partial retention)
- Cannot control bowel - unexpected fecal soiling or inability to defecate
- Feeling of electric shock down the back when bending neck (Lhermitte's sign)
- Band-like pain or tightness around the lower chest or abdomen
If any of these develop: Emergency MRI of the full spine immediately. Dexamethasone (steroid) must be started within hours. The management flowchart below applies directly:
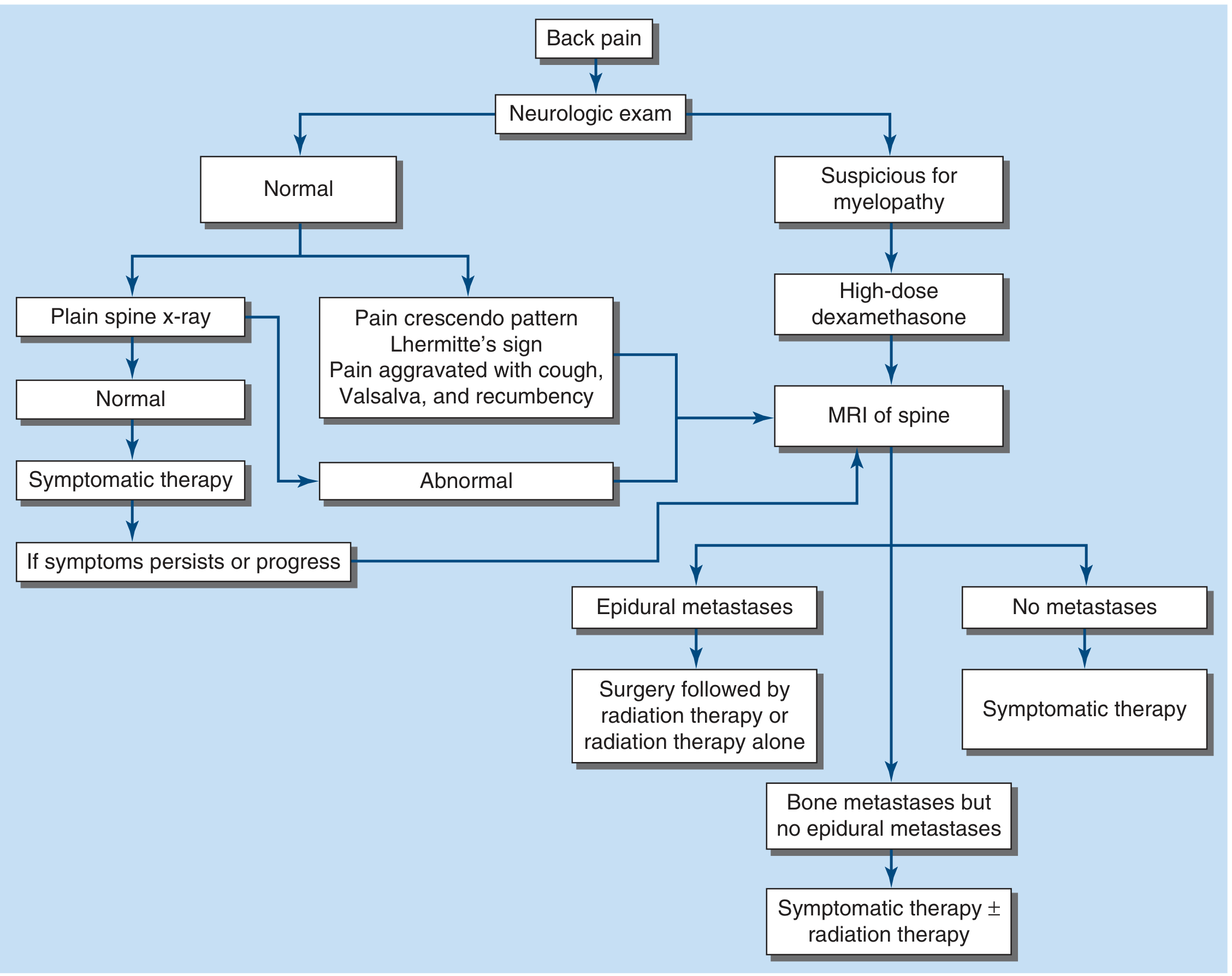
Treatment if Cord Compression Develops
Step 1 - Immediate: High-dose Dexamethasone
- Dexamethasone 16 mg IV loading dose, then 4 mg every 6 hours
- Reduces edema and swelling around the compressed cord
- Buys time - can temporarily stabilize or even partially reverse early compression
- Must be started within hours of symptoms
Step 2 - Urgent MRI Full Spine
- Within 24 hours (or immediately if neurological signs are present)
- Confirms the level and extent of compression
- Checks if other spinal levels are also involved (25% of patients have multiple sites)
Step 3 - Radiation Therapy (Most Likely Treatment for This Patient)
- Radiotherapy to D12 is the standard treatment for MSCC in prostate cancer
- Prostate cancer is moderately radiosensitive
- Delivered urgently (within 24 hours of diagnosis if possible)
- Typically 20 Gy in 5 fractions or 30 Gy in 10 fractions
- Can shrink the tumor mass and relieve cord compression
- Best results when started before paralysis develops
Step 4 - Surgery (If Indicated)
- Decompressive laminectomy + spinal stabilization
- For: rapid neurological deterioration, spinal instability, pathological fracture with bone in the canal, or failure of radiotherapy
- Followed by radiotherapy after surgery
- Per Goldman-Cecil: "Patients with an unstable spine, limited disease burden, and a relatively favorable prognosis may benefit from decompressive resection and spinal stabilization."
- At age 76 with bone metastases, surgery risk must be carefully weighed
Step 5 - Vertebroplasty/Kyphoplasty
- If the vertebra is collapsing/fractured but cord compression is not yet severe
- Cement is injected into the fractured vertebral body to stabilize it
- Reduces pain and prevents further collapse
- Can be done under local anesthesia - safer for elderly patients
Step 6 - ADT and Bone-Protecting Agents (Ongoing)
- ADT (already indicated for cancer treatment) will shrink the tumor, including the D12 lesion
- Zoledronic acid or Denosumab - reduce skeletal events including fracture and need for radiation
- Radium-223 - once disease becomes castration-resistant, targets bone metastases directly
Prognosis Honestly Stated
- Prostate cancer is generally more slowly progressive than lung or breast
- Prostate cancer responds well to ADT - the D12 lesion can regress with treatment
- The goal is to treat the cancer aggressively with ADT + second agent before cord compression develops
- The patient who is ambulatory at the time of treatment has significantly better outcomes than one who is already paralyzed