Management of Diabetes Step Wise 50 year old female No history of HTN, IHD, CAD, CKD just hypothyroidism
Reading File
Finding Sources
Searching PubMed
"type 2 diabetes" AND "management" AND "guidelines"
Searching the Web
ADA 2025 2026 standards diabetes care stepwise management algorithm type 2
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
I have enough comprehensive data to construct a detailed, stepwise management plan. Here is the full answer:
Stepwise Management of Type 2 Diabetes - 50-Year-Old Female (Hypothyroidism, No HTN/IHD/CAD/CKD)
Patient Profile Summary
- Age: 50 years, Female
- Comorbidity: Hypothyroidism (ensure TSH optimized - uncontrolled hypothyroidism worsens insulin resistance and dyslipidemia)
- No ASCVD, HTN, IHD, CAD, CKD - this simplifies the algorithm as we do NOT need to prioritize SGLT-2 or GLP-1RA for cardioprotection as first choice
STEP 1 - Initial Assessment Before Starting Therapy
| Test | Target/Purpose |
|---|---|
| HbA1c | Establishes glycemic baseline and guides intensity of therapy |
| FPG / OGTT | Confirm diagnosis if not done |
| Fasting lipid profile | Screen for dyslipidemia (common with T2DM + hypothyroidism) |
| Serum creatinine / eGFR | Baseline renal function (for Metformin safety) |
| LFTs | Baseline |
| Urine microalbumin / ACR | Early nephropathy screen |
| TSH, Free T4 | Optimize thyroid status - hypothyroidism impairs glycemic control and lipid metabolism |
| Retinal exam | Screen for retinopathy at diagnosis |
| BMI / waist circumference | Guide lifestyle and drug choice |
| BP | Baseline |
Key point: First optimize thyroid replacement (levothyroxine titration to TSH 0.5-2.5 mIU/L). Uncontrolled hypothyroidism independently worsens dyslipidemia, insulin resistance, and weight gain - all of which worsen diabetes management.
STEP 2 - Set Individualized Glycemic Targets
Per Harrison's Principles of Internal Medicine 22E (2025):
| Parameter | Target for this patient |
|---|---|
| HbA1c | < 7.0% (she is 50, no major comorbidities, cognitively intact) |
| Fasting plasma glucose | 80-130 mg/dL |
| 2-hr post-prandial glucose | < 180 mg/dL |
| BP (though no HTN) | < 130/80 mmHg (monitor) |
| LDL | < 100 mg/dL (< 70 if high risk) |
A more stringent HbA1c ≤ 6.5% may be considered if achievable without hypoglycemia.
STEP 3 - Lifestyle Modification (Non-Pharmacological - Initiated from DAY 1)
These are concurrent with, not prior to, pharmacotherapy at diagnosis if HbA1c ≥ 7.5-8%.
a) Medical Nutrition Therapy (MNT)
- Reduce total caloric intake; target 5-10% weight loss if overweight/obese
- Low glycaemic index diet; limit refined carbohydrates and saturated fats
- Consistent carbohydrate distribution across meals
- Mediterranean or DASH dietary pattern preferred
b) Physical Activity
- 150 min/week moderate aerobic exercise (brisk walking, cycling, swimming)
- Resistance training 2-3 days/week
- Reduce prolonged sedentary time
- Stress test needed only if disease duration > 10 years before intensive activity
c) Behavioral/Lifestyle
- Weight management program if BMI > 25
- Smoking cessation
- Limit alcohol (≤1 drink/day for women)
- Diabetes self-management education and support (DSMES)
- Structured self-monitoring of blood glucose (SMBG)
STEP 4 - Pharmacotherapy: Stepwise Escalation
Step 4A - First-Line Monotherapy: METFORMIN
Start at diagnosis - Metformin remains the universal consensus first-line agent.
| Aspect | Detail |
|---|---|
| Mechanism | Decreases hepatic glucose production (gluconeogenesis inhibition via AMPK activation); improves peripheral insulin sensitivity |
| Starting dose | 500 mg OD or BD with meals |
| Target dose | 1000 mg BD (max 2550 mg/day) |
| Titration | Increase by 500 mg every 1-2 weeks to minimize GI side effects |
| HbA1c reduction | 1.0-1.5% |
| Weight effect | Neutral to slight weight loss |
| Hypoglycemia risk | None (does not cause hypoglycemia as monotherapy) |
| Key benefit | Cardiovascular neutral/beneficial; low cost; weight neutral |
| Contraindications | eGFR < 30 (avoid), 30-45 (use with caution, reduce dose) - not applicable here |
| Side effects | GI (nausea, diarrhea, flatulence - dose dependent, mitigated with food and slow titration); rarely lactic acidosis; B12 deficiency with long-term use |
| Special note for hypothyroidism | If patient is on levothyroxine, no interaction with metformin directly, but watch for malabsorption |
Reassess HbA1c at 3 months. If target NOT met, proceed to Step 4B.
Step 4B - Dual Therapy: Metformin + Second Agent
Since this patient has no ASCVD, no HF, no CKD, the second agent choice is primarily based on:
- HbA1c gap from target
- Weight (overweight - prefer weight-neutral or weight-losing agents)
- Hypoglycemia risk
- Cost and patient preference
- Menopausal status (perimenopausal at 50 - TZDs may worsen bone density)
| Agent Class | Examples | HbA1c ↓ | Weight | Hypo Risk | Notes for this patient |
|---|---|---|---|---|---|
| GLP-1 Receptor Agonist | Semaglutide, Dulaglutide, Liraglutide | 1.0-1.5% | ↓↓ (weight loss) | Low | Preferred 2nd agent if overweight/obese. CV benefit. Nausea common initially |
| SGLT-2 Inhibitor | Empagliflozin, Dapagliflozin, Canagliflozin | 0.5-1.0% | ↓ (modest) | Low | Good if overweight; UTI/genital infections risk; monitor eGFR |
| DPP-4 Inhibitor | Sitagliptin, Vildagliptin, Saxagliptin | 0.5-0.8% | Neutral | Low | Well tolerated, oral, convenient; less potent |
| Sulfonylurea | Glimepiride, Glipizide, Gliclazide | 1.0-1.5% | ↑ (weight gain) | Yes - hypoglycemia risk | Cheap but weight gain and hypo risk; less preferred |
| Thiazolidinedione (TZD) | Pioglitazone | 0.5-1.4% | ↑↑ | Low | Avoid in perimenopausal - increases fracture risk. Also weight gain and fluid retention |
For this 50-year-old overweight/obese patient: Preferred 2nd agent is GLP-1RA (semaglutide oral 7-14 mg daily, or weekly SC dulaglutide/semaglutide) given weight reduction benefit and CV protection even as a preventive strategy. If cost is a concern, SGLT-2 inhibitor is a strong alternative.
Reassess HbA1c at 3 months. If still not at target, proceed to Step 4C.
Step 4C - Triple Therapy: Metformin + 2 Other Agents
Choose a complementary third agent addressing different mechanisms:
- Example: Metformin + GLP-1RA + SGLT-2 inhibitor (excellent combination - complementary mechanisms, weight loss, low hypoglycemia)
- Or: Metformin + SGLT-2 inhibitor + DPP-4 inhibitor
- Or: Metformin + Sulfonylurea + DPP-4 inhibitor (if cost is the priority)
Note: Avoid combining DPP-4 inhibitors with GLP-1RAs (redundant mechanism via the same incretin pathway, no additive benefit).
Step 4D - Insulin Therapy
When oral/injectable non-insulin agents fail to maintain targets, or HbA1c is very high at presentation (> 10-11%), insulin is added or substituted.
Initiation:
- Basal insulin first: Insulin glargine (U100 or U300) or Insulin degludec
- Start: 10 units SC at bedtime OR 0.1-0.2 units/kg/day
- Titrate: Increase by 2 units every 3 days until fasting glucose 80-130 mg/dL
- Continue metformin with basal insulin (reduces insulin dose requirement and weight gain)
Intensification if needed:
- Add prandial insulin (rapid-acting: Aspart, Lispro, Glulisine) before largest meal
- Titrate to post-meal glucose targets
- "Basal-bolus" regimen: 4 injections/day - 1 basal + 3 prandial
Premixed insulin option (for simpler regimen):
- Biphasic insulin 30/70 or 70/30 BD (before breakfast and dinner)
- Less flexible but simpler for adherence
STEP 5 - Management of Comorbidities
Dyslipidemia (very likely with T2DM + hypothyroidism)
- Check lipids AFTER TSH is optimized - hypothyroidism-related dyslipidemia may partly resolve with euthyroid state
- If LDL remains elevated: Statin therapy - Atorvastatin 10-40 mg (moderate intensity for primary prevention at age 50 with diabetes)
- Target LDL < 100 mg/dL
Blood Pressure
- No HTN currently - monitor at every visit
- Target if BP develops: < 130/80 mmHg
- First-line if diabetes + HTN develops: ACE inhibitor or ARB (renoprotective)
Antiplatelet Therapy
- No aspirin for primary prevention in T2DM without established CVD per current ADA guidance (bleeding risk outweighs benefit)
Thyroid Management (Key Interaction)
- Maintain TSH in target range (0.5-2.5 mIU/L)
- Poorly controlled hypothyroidism → worsens insulin resistance, dyslipidemia, weight, and makes diabetes harder to control
- Levothyroxine should be taken 30-60 min before breakfast, away from metformin and other drugs that may affect absorption
- Monitor TSH every 6 months in stable diabetes + hypothyroidism
STEP 6 - Screening for Complications (from Diagnosis Onwards)
| Complication | Screen | Frequency |
|---|---|---|
| Diabetic Retinopathy | Dilated fundus exam | At diagnosis, then annually |
| Diabetic Nephropathy | Urine ACR + eGFR | Annually |
| Diabetic Neuropathy | Monofilament test, vibration sense | Annually |
| Peripheral Arterial Disease | Foot exam, ABI if indicated | Annually |
| ASCVD risk | Framingham/ASCVD score, lipids | Annually |
| Non-alcoholic fatty liver (MASLD) | LFTs, USS abdomen | Per clinical suspicion |
| Dental health | Dental exam | Biannually |
| Sleep apnea | Clinical screen | If symptoms present |
STEP 7 - Monitoring Schedule
| Parameter | Frequency |
|---|---|
| HbA1c | Every 3 months until target, then every 6 months |
| Fasting blood glucose | SMBG as per regimen (at least fasting daily) |
| Urine microalbumin | Annually |
| eGFR / Creatinine | Annually |
| Lipid profile | Annually |
| TSH | Every 6 months |
| BP | Every visit |
| Weight / BMI | Every visit |
| Retinal exam | Annually |
| Foot exam | Every visit (inspect), formal annually |
| ECG | Baseline, then as clinically indicated |
| Vitamin B12 | Every 1-2 years (Metformin-related depletion) |
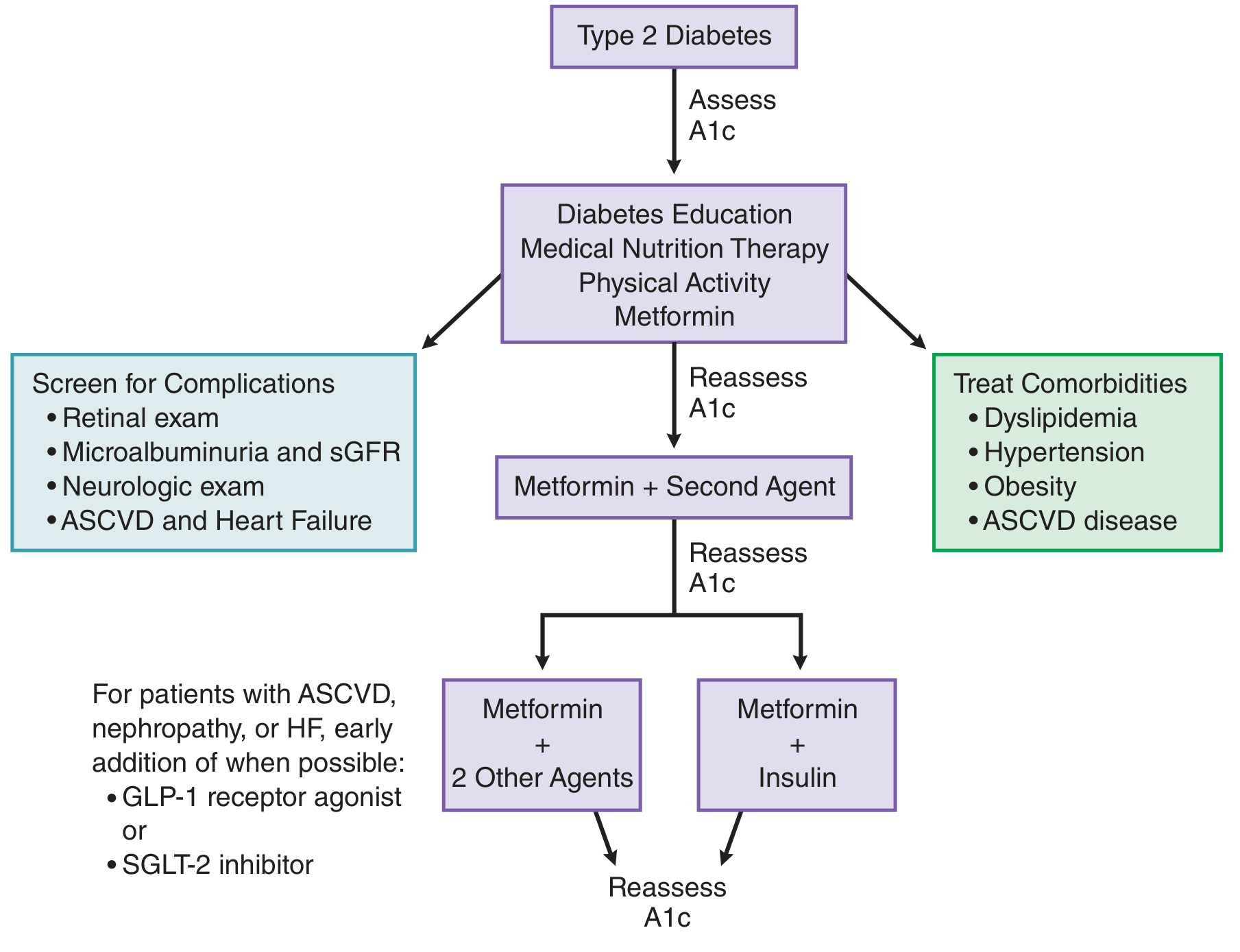
Summary Flowchart for This Patient
Diagnosis of T2DM in 50F with Hypothyroidism
↓
STEP 1: Optimize TSH + Full metabolic work-up
↓
STEP 2: Set HbA1c target < 7.0%
↓
STEP 3: Lifestyle (diet + exercise + DSMES) - start immediately
↓
STEP 4A: Metformin (500mg → 2000mg) + reassess HbA1c at 3 months
↓ [If HbA1c not at target]
STEP 4B: Add GLP-1RA (preferred if overweight) or SGLT-2i
↓ [If HbA1c still not at target]
STEP 4C: Add 3rd agent (triple therapy)
↓ [If still failing]
STEP 4D: Add Basal Insulin (+ continue Metformin)
↓ [If post-meal glucose also uncontrolled]
STEP 4E: Basal-Bolus Insulin Regimen
↓
STEP 5: Treat dyslipidemia (statin), monitor BP, optimize thyroid
↓
STEP 6: Ongoing complication screening
↓
STEP 7: Regular monitoring (HbA1c q3 months, annual bloods/eyes/feet)
Sources: Harrison's Principles of Internal Medicine 22E (2025), Goodman & Gilman's Pharmacological Basis of Therapeutics, Textbook of Family Medicine 9E - ADA/EASD consensus algorithm for T2DM management.
This is a shared conversation. Sign in to Orris to start your own chat.