Scaphoid fracture
Reading File
Finding Sources
Searching PubMed
"scaphoid fracture" AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full synthesis:
Scaphoid Fracture
Epidemiology
The scaphoid is the most commonly fractured carpal bone, accounting for 62-87% of all carpal fractures. It most often affects young active adults (males 20-30 years old) and is frequently seen after sports injuries.
Anatomy & Blood Supply - The Key to Understanding Complications
The scaphoid spans both rows of the carpus and has a unique, vulnerable blood supply. Arteries (branches of the radial artery, plus palmar and superficial arteries) enter through the distal pole and travel retrograde (distally to proximally) to supply the proximal pole. This means:
- A fracture across the waist cuts off the blood supply to the proximal fragment
- Approximately 10% of individuals have a sole blood supply from the radial artery, making AVN prediction impossible
- The more proximal the fracture, the higher the risk of AVN - up to 80% of proximal pole fractures develop avascular necrosis
(Gray's Anatomy for Students; Tintinalli's Emergency Medicine)
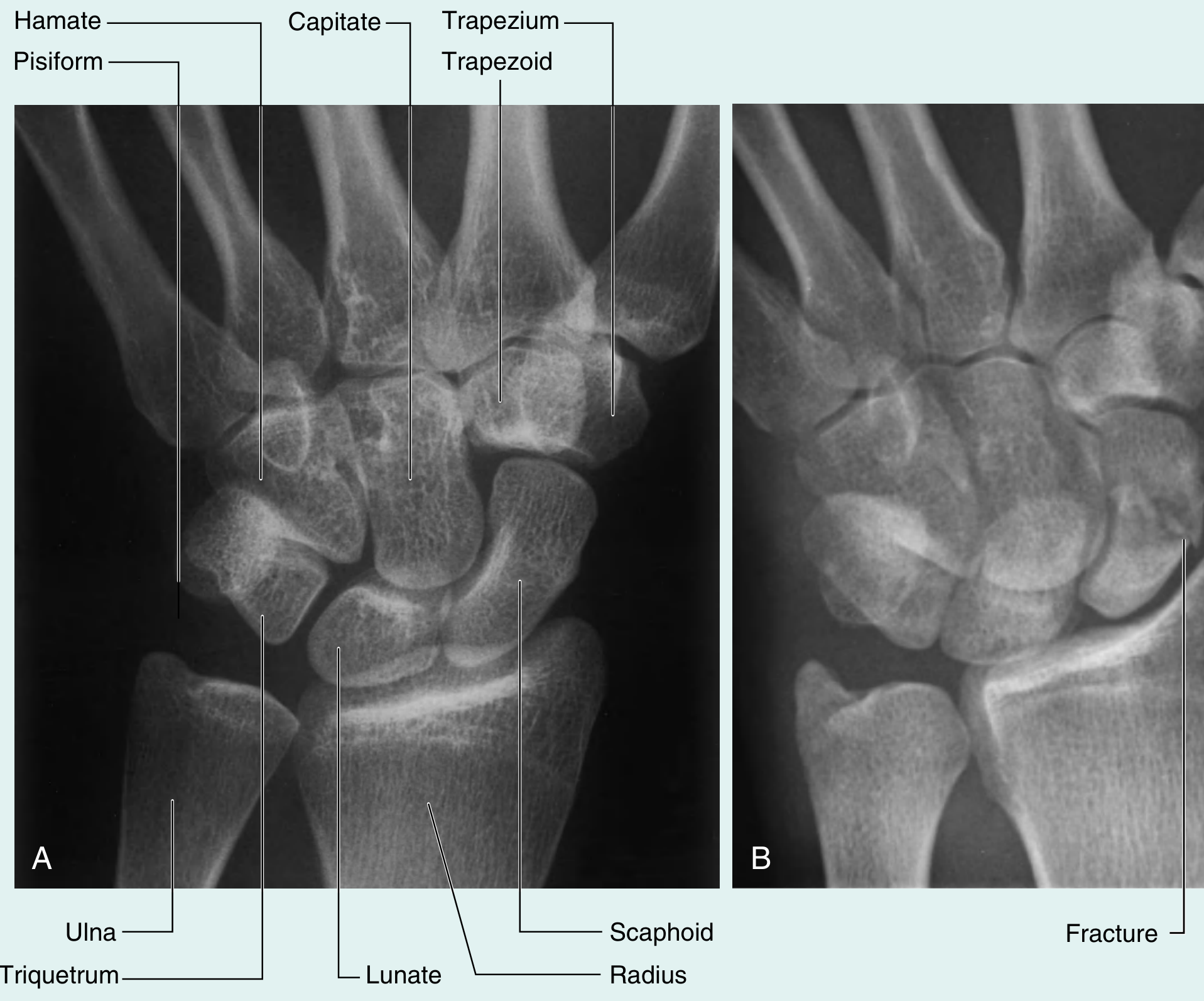
Wrist anatomy and scaphoid fracture (PA view):
Mechanism of Injury
- Fall on an outstretched, dorsiflexed hand (FOOSH) - most common
- Axial load directed along the thumb's metacarpal
- ~12% of scaphoid fractures have an associated injury (distal radius, other carpal bones, carpal instability pattern, or dislocation)
Fracture Location
| Location | Frequency |
|---|---|
| Waist (middle third) | ~65% |
| Proximal third | 16-28% |
| Distal third (tubercle) | ~10% |
Clinical Features
Symptoms: Pain along the radial aspect of the wrist after FOOSH.
Signs:
| Test | Sensitivity | Specificity |
|---|---|---|
| Anatomical snuffbox tenderness | 90% | 40% |
| Scaphoid tubercle tenderness | 87% | 57% |
| Pain with resisted supination/pronation | 79% | 58% |
| Thumb-index finger pinch pain | 73% | 75% |
The first three examination findings combined achieve a specificity of 75%. The anatomical snuffbox is best palpated with the wrist in ulnar deviation, which exposes more of the scaphoid.
Key rule: Tenderness in the anatomical snuffbox after trauma should be treated as a scaphoid fracture until proven otherwise. (Schwartz's Principles of Surgery)
Imaging
Plain X-rays:
- Include standard PA, lateral, and dedicated scaphoid view (PA in ulnar deviation - profiles the bone lengthwise)
- Distortion of the radial fat stripe is suggestive of injury
- Up to ~20% of fractures are invisible on initial X-ray
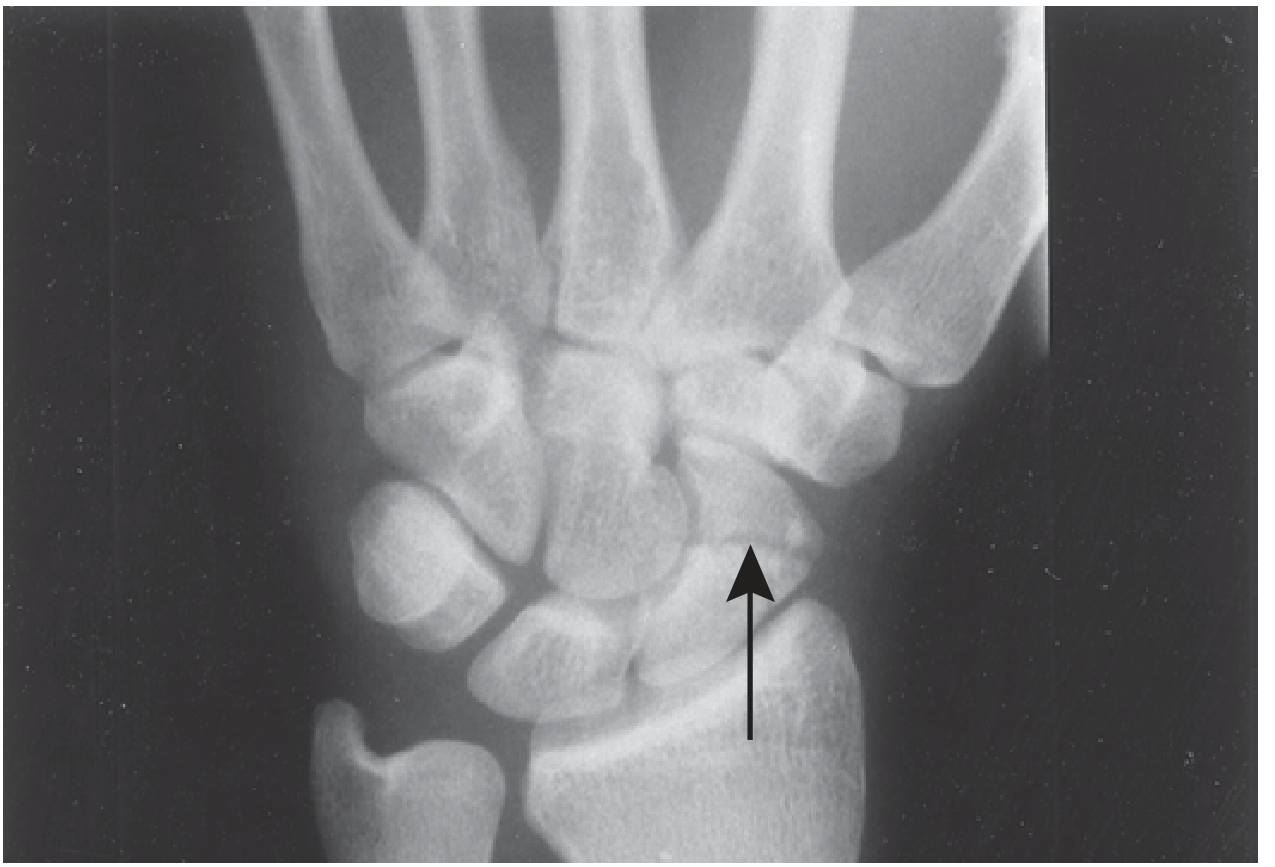
Scaphoid fracture on X-ray (waist fracture, arrow):
Advanced imaging:
| Modality | Sensitivity | Specificity | Notes |
|---|---|---|---|
| CT | 89-100% | 85-100% | Good for cortical detail, displacement measurement |
| MRI | 98-100% | ~100% | Gold standard for occult fractures |
| Bone scan | High but non-specific | Lower | Can be used if MRI unavailable |
MRI is the gold standard for definitive diagnosis when initial X-rays are negative but clinical suspicion remains high. Recent UK trial data showed immediate MRI improves cost savings, diagnostic accuracy, and patient satisfaction compared to serial casting. (Rosen's Emergency Medicine)
Classification (Instability Criteria)
A scaphoid fracture is considered unstable if:
- Displacement ≥ 1 mm
- Oblique fracture pattern
- Fracture angulation (hump-back deformity on lateral X-ray)
- Associated perilunate injury or carpal instability
Management
Suspected Fracture (X-ray negative, clinically suspected)
Apply a thumb spica splint (short arm, wrist in ~10° dorsiflexion and radial deviation) and arrange urgent orthopaedic follow-up within 1 week. If facilities allow, perform early MRI or CT for definitive diagnosis rather than serial immobilisation/re-examination.
The traditional protocol of immobilise-and-re-examine at 10-14 days is still used where advanced imaging is not readily available. (Rosen's EM; Bailey & Love)
Confirmed Fractures
Non-operative (stable, non-displaced):
- Below-elbow thumb spica cast
- Thumb inclusion is no longer considered mandatory as routine
- Duration varies by location: distal pole heals fastest; proximal pole fractures need longer immobilisation (up to 12-20 weeks)
Surgical (displaced or unstable):
- Displacement ≥ 1 mm or instability = consider open reduction and internal fixation (ORIF) with a headless compression screw (e.g., Herbert screw)
- Approach: dorsal approach for proximal pole fractures; volar approach for waist/distal fractures
- Percutaneous screw fixation is increasingly used for non-displaced waist fractures to allow earlier return to activity
- 2025-2026 meta-analyses (PMID 41267607) confirm surgical fixation results in faster functional recovery compared to casting for waist fractures, though union rates are similar
Emerging technique: Robot-assisted screw fixation has been shown in recent 2026 meta-analyses (PMID 41931267) to improve accuracy of screw placement compared to free-hand fluoroscopy-guided techniques.
Complications
| Complication | Notes |
|---|---|
| Avascular necrosis (AVN) | Due to retrograde blood supply; up to 80% risk in proximal fractures; leads to collapse and arthritis |
| Non-union | Most common complication of missed/untreated fractures; requires bone grafting ± fixation |
| Malunion | "Hump-back" deformity; results in altered wrist mechanics |
| Carpal instability | DISI (dorsal intercalated segment instability) pattern; results from scapholunate ligament disruption |
| Scaphoid non-union advanced collapse (SNAC wrist) | Progressive arthritis from chronic non-union |
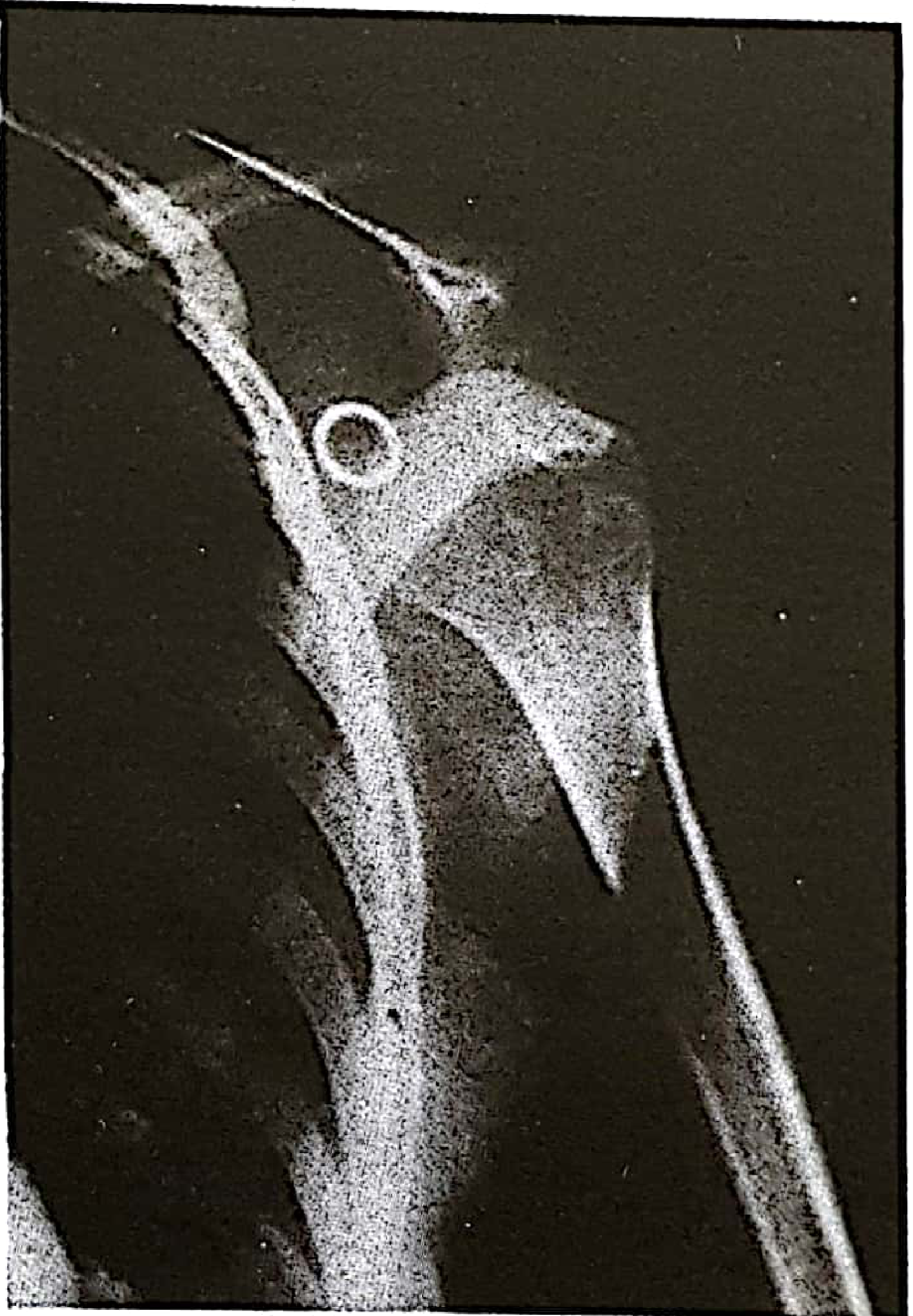
AVN of the scaphoid (X-ray showing sclerosis/collapse):

ED Summary (Tintinalli's)
- Diagnosed fracture: Long arm thumb spica splint in dorsiflexion + radial deviation, urgent orthopaedic referral
- Suspected fracture (normal X-ray): Short arm thumb spica splint in dorsiflexion + radial deviation, orthopaedic follow-up within 1 week ± early advanced imaging
Sources
- Bailey and Love's Short Practice of Surgery, 28th ed.
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
- Rosen's Emergency Medicine: Concepts and Clinical Practice
- Schwartz's Principles of Surgery, 11th ed.
- Gray's Anatomy for Students
Shoulder dislocation
Finding Sources
Searching PubMed
"shoulder dislocation" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer.
Shoulder Dislocation
Overview
The shoulder (glenohumeral joint) is the most commonly dislocated large joint in the body. The glenoid fossa is inherently shallow, providing mobility at the expense of stability. The joint relies on the glenoid labrum, capsule, ligaments, and rotator cuff for dynamic and static stabilisation. (Tintinalli's Emergency Medicine)
Types
| Type | Frequency | Mechanism |
|---|---|---|
| Anterior (subcoracoid) | ~95% | Abduction + extension + external rotation |
| Posterior | <5% | Seizure, electric shock, forced internal rotation |
| Inferior (luxatio erecta) | Very rare | Hyperabduction force |
| Superior | Extremely rare | Massive upward force |
Anterior subtypes: subcoracoid (most common), subglenoid, subclavicular, intrathoracic (very rare).
Anatomy
The glenohumeral joint is a ball-and-socket articulation between the glenoid fossa of the scapula and the humeral head. Because the socket is shallow, stability depends on:
- The glenoid labrum - deepens the socket, provides a suction cup effect
- The inferior glenohumeral ligament - primary restraint against anterior dislocation
- The rotator cuff - dynamic stabiliser (SITS muscles)
- The capsule - reinforced by glenohumeral ligaments
X-ray: anterior subcoracoid dislocation (PA view)
Clinical Features
Anterior Dislocation
- Arm held in slight abduction and external rotation
- Shoulder "squared off" - loss of normal rounded deltoid contour
- Visible/palpable step deformity; humeral head palpable anteriorly
- Patient resists adduction and internal rotation
- Cannot touch the contralateral shoulder with the affected hand
Posterior Dislocation (the "great masquerader")
- Arm held in internal rotation with limited external rotation
- Often missed on AP X-ray - the classic "light bulb sign" on AP view
- Clue in the history: epileptic fit, electric shock, or forceful restraint
- The axillary view is essential and will show posterior displacement
Pre-reduction Imaging
Pre-reduction radiographs should be obtained when there has been significant trauma, unless circulation is threatened. They are essential because fracture-dislocations and simple dislocations look similar clinically but require very different management approaches.
Risk factors that predict clinically important associated fractures:
- Age > 40 years
- First episode of dislocation
- Traumatic mechanism (fall >1 flight of stairs, assault, or motor vehicle collision)
- If any of these 3 are present: sensitivity 97.7% for significant fracture
Recurrent atraumatic dislocations in young patients with a clearly known mechanism may not require pre-reduction films.
Views:
- AP - detects most anterior dislocations and humeral neck fractures
- Axillary view - the single most important view; confirms direction of dislocation; essential for posterior dislocation
- Scapular Y - useful supplement when axillary view cannot be obtained
Associated Injuries (Bony & Soft Tissue)
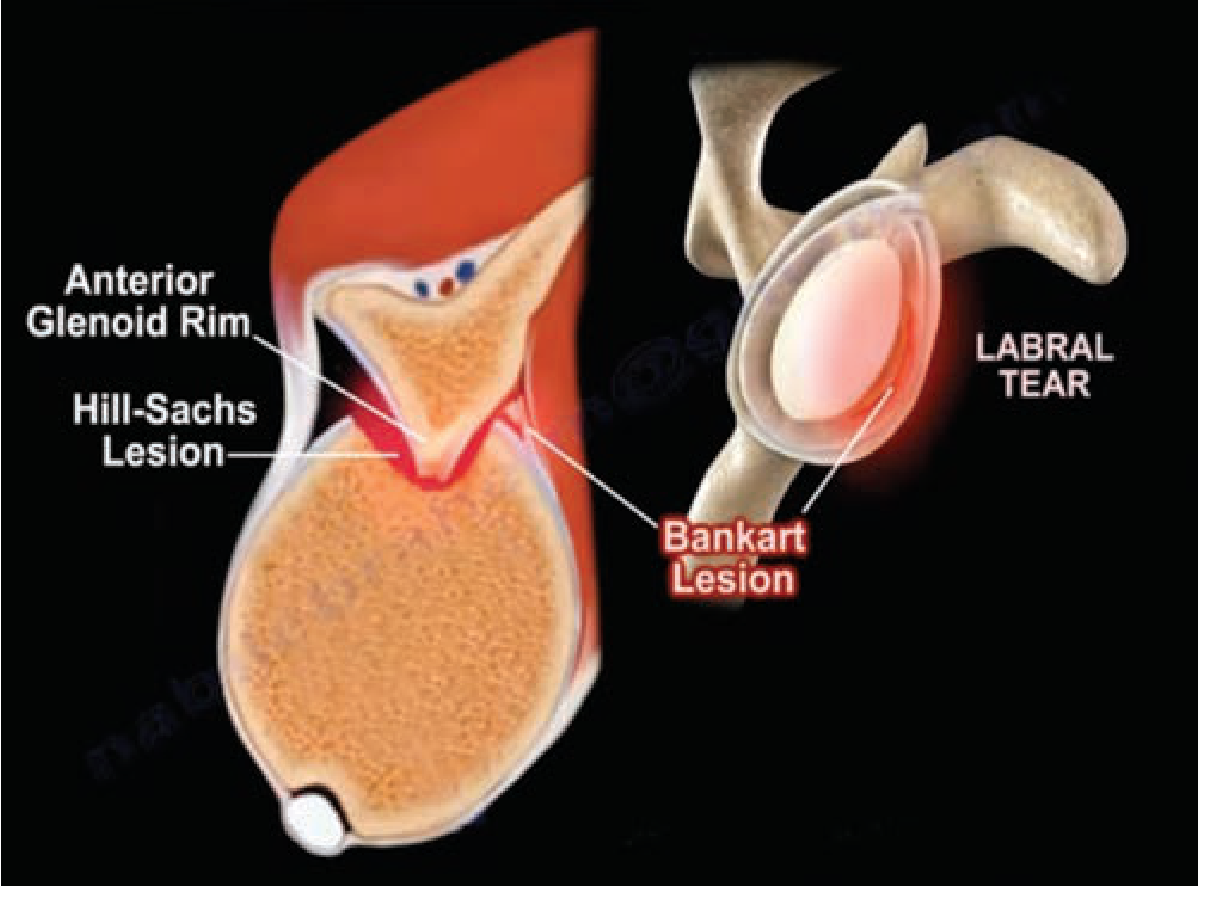
Hill-Sachs Lesion
- Impaction fracture of the posterolateral humeral head
- Caused by the humeral head striking the anterior glenoid rim during dislocation
- Found in up to 50% of anterior dislocations
- Often seen only on post-reduction films
- Rarely has clinical significance in isolation; can become "engaging" (catches on glenoid rim) if large
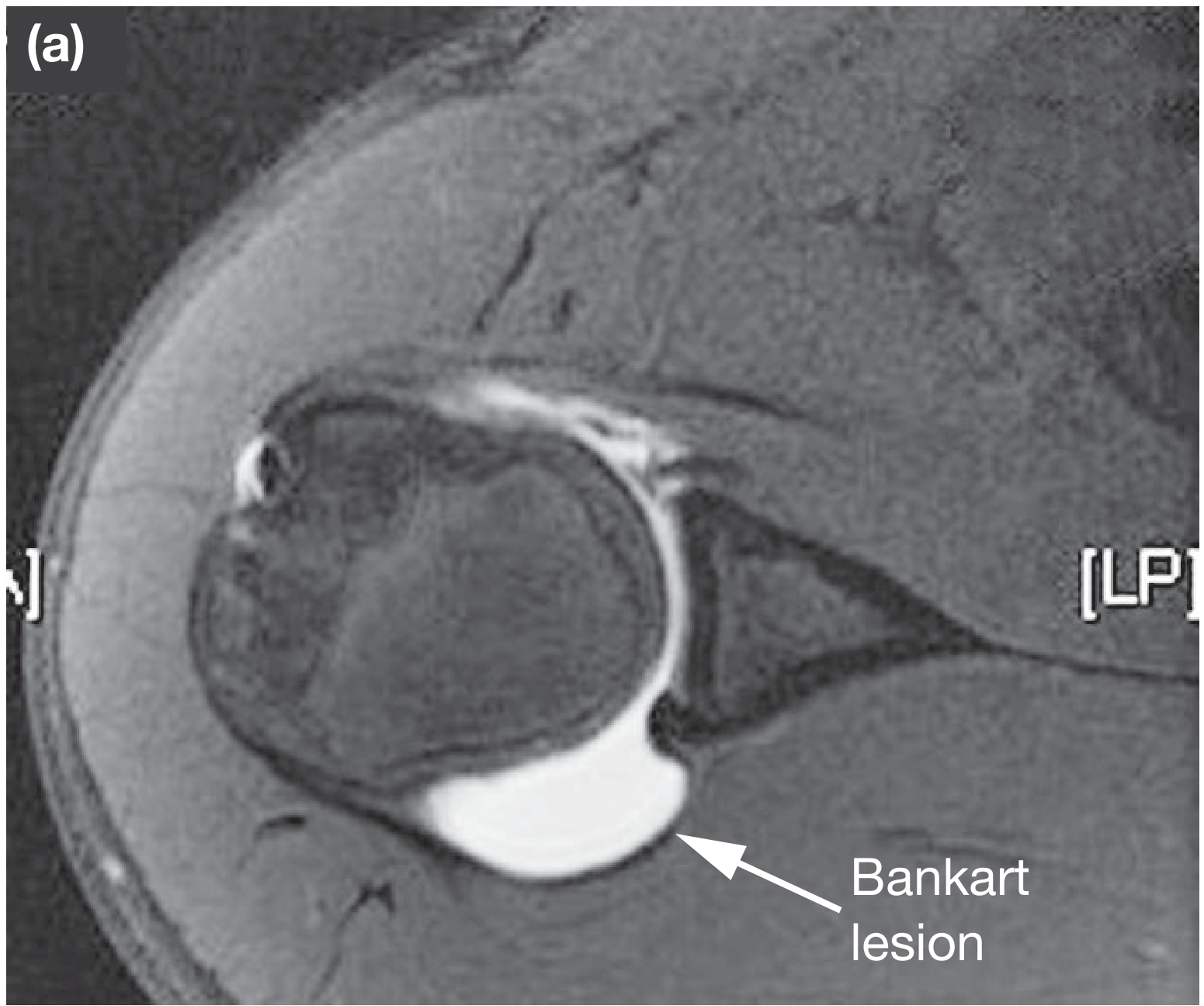
Bankart Lesion
- Avulsion of the anteroinferior glenoid labrum from the glenoid rim
- The fundamental pathology underlying recurrent instability
- Soft Bankart = labral detachment alone
- Bony Bankart = labral avulsion with a fragment of the anterior glenoid rim
- Implicated as a primary cause of recurrent anterior dislocation
CT scan of shoulder showing Bankart lesion (frontal view):

MR arthrogram showing anteroinferior Bankart lesion:
Other Associated Injuries
| Structure | Injury |
|---|---|
| Greater tuberosity | Avulsion fracture (common in elderly) |
| Humeral neck | Fracture - MUST identify before reduction to avoid AVN |
| Glenoid rim | Bony Bankart |
| Rotator cuff | Tear - especially in patients > 40 years old |
| Axillary nerve | Neuropraxia (10-25% of dislocations) |
| Axillary artery | Rare; more common in elderly |
One prospective study found associated injuries in up to 60% of patients with anterior shoulder dislocation, higher than previously thought. (Roberts & Hedges' Clinical Procedures in Emergency Medicine)
Neurovascular Assessment (Mandatory Before and After Reduction)
Always perform before and after reduction:
- Axillary nerve (most commonly injured) - test pinprick sensation over the "regimental badge" area (lateral deltoid). Motor testing (deltoid contraction) is unreliable because pain prevents it.
- Radial nerve - check wrist extension
- Axillary artery - palpate radial pulse; look for axillary hematoma, bruising of lateral chest wall, axillary bruit
If unable to raise the arm after reduction: in the young - suspect axillary nerve injury; in the elderly - suspect rotator cuff tear.
Reduction Techniques
Adequate analgesia and muscle relaxation are the prerequisite for all methods. Options include IV opioids ± procedural sedation, or intra-articular lidocaine injection (10-20 mL of 1% plain lidocaine into the joint via the lateral sulcus, allow 15-20 minutes - reported to be effective and avoids sedation risks).
1. Stimson Maneuver (Gravity-Assisted)
- Patient prone on elevated stretcher
- 2.5-5 kg weight suspended from the wrist
- Slow steady traction over 20-30 minutes allows gradual muscle relaxation and reduction
- Advantage: no assistant needed, minimal force applied
- Success rate ~91%; increases to 96% when combined with scapular manipulation
- Disadvantages: time-consuming; prone positioning has airway implications
2. Scapular Manipulation Technique
- Combined with Stimson positioning (prone, arm dependent)
- Operator applies traction on the arm while rotating the scapular tip medially and superiorly with the thumbs
- Success rate >90% in experienced hands; no reported complications in literature
- Works by repositioning the glenoid fossa rather than forcing the humeral head
3. External Rotation Method (Hennepin Technique)
- Patient seated or supine
- Elbow flexed to 90°, arm adducted
- Slowly externally rotate the arm while maintaining gentle traction - reduction often occurs with a palpable clunk
- Gentle, low-force technique; well tolerated
4. Traction-Countertraction
- Assistant applies countertraction via sheet across the chest
- Operator applies steady longitudinal traction along the arm with slight lateral traction
- Classic and reliable; requires two people
5. Hippocratic Method (historical)
- Operator uses foot in the axilla for countertraction while pulling on the arm
- Largely replaced by safer modern techniques due to risk of neurovascular damage
Key principle: Reduction is easier the sooner it is attempted - early reduction is always preferred.
Post-Reduction Care
- Confirm reduction clinically (restored rounded contour, range of motion) and radiographically
- Repeat neurovascular examination
- Immobilise in a broad arm sling (internal rotation) for 2-3 weeks - though there is ongoing debate about whether immobilisation in external rotation reduces recurrence
- Orthopaedic follow-up - especially important in first-time dislocations (to address recurrence risk and Bankart lesion)
- Physiotherapy - progressive rotator cuff and shoulder girdle strengthening
Recurrence
Recurrence is the most common complication and is strongly age-dependent:
| Age at First Dislocation | Recurrence Rate |
|---|---|
| < 20 years | ~90% |
| 20-40 years | ~50-60% |
| > 40 years | Lower (but rotator cuff tear risk increases) |
Recurrent dislocations require progressively less force to occur. After multiple episodes, patients may self-reduce.
Surgical Management (Recurrent Instability)
Surgical repair is indicated for recurrent instability and is increasingly considered after a first-time dislocation in young athletes.
Arthroscopic Bankart Repair
- Reattaches the detached anteroinferior labrum to the glenoid rim with suture anchors
- Success rate up to 90-95% for recurrence prevention
- A 2024 systematic review (PMID 39428642) confirms good outcomes with arthroscopic Bankart repair
- Knotless vs. knotted techniques: 2025 meta-analysis (PMID 40483425) found comparable recurrence rates
- Inevitably causes some restriction of external rotation
Open Stabilisation (Latarjet / Putti-Platt / Bristow)
- Latarjet procedure: transfers the coracoid process to the anterior glenoid - preferred when there is significant bony glenoid loss (> 20-25%)
- Putti-Platt / Bankart operations: tighten and reinforce the anterior capsular structures
- A 2026 network meta-analysis (PMID 41945260) compared arthroscopic vs. open approaches - both effective; open procedures (particularly Latarjet) offer lower recurrence when significant bone loss is present
Remplissage
- Fills the Hill-Sachs defect with posterior capsule/infraspinatus tendon to prevent engagement
- Used in addition to Bankart repair when Hill-Sachs lesion is large ("engaging")
- Recent RCT data shows significant reduction in recurrence with remplissage + Bankart vs. Bankart alone
Posterior Dislocation - Special Notes
- Often missed - reported delay in diagnosis is common because the AP X-ray can look deceptively normal
- Classic signs: light bulb sign (AP) and trough sign (impaction fracture of anteromedial humeral head = reverse Hill-Sachs)
- Axillary view is diagnostic and must always be obtained if posterior dislocation is suspected
- CT indicated if axillary view cannot be obtained
- Associated with seizures and electric shock because of forceful bilateral muscle contraction in internal rotation
Complications Summary
| Complication | Notes |
|---|---|
| Recurrent dislocation | Most common; up to 90% in young patients |
| Hill-Sachs lesion | Up to 50% of anterior dislocations |
| Bankart lesion | Key cause of recurrence |
| Rotator cuff tear | Common in >40 age group; suspect if weak external rotation after reduction |
| Axillary nerve injury | 10-25%; usually neuropraxia - recovery expected |
| Axillary artery injury | Rare; elderly patients; high morbidity |
| Fracture-dislocation | Humeral neck/head, greater tuberosity; requires pre-reduction imaging |
| Missed posterior dislocation | Leads to significant disability if not treated promptly |
Sources
- Bailey and Love's Short Practice of Surgery, 28th ed.
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
- Rosen's Emergency Medicine: Concepts and Clinical Practice
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Schwartz's Principles of Surgery, 11th ed.
- Pye's Surgical Handicraft, 22nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.