Arterial supply to head and neck
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative sources. Let me compile the complete answer.
Arterial Supply to the Head and Neck
The head and neck receive arterial blood from two main sources: the common carotid arteries (dominant supply) and the subclavian arteries (via the vertebral arteries and thyrocervical/costocervical trunks).
1. Common Carotid Artery (CCA)
- Right CCA - arises from the brachiocephalic (innominate) artery
- Left CCA - arises directly from the arch of the aorta
- Both ascend in the carotid sheath (with the internal jugular vein laterally and vagus nerve posteriorly), covered inferiorly by sternocleidomastoid
- At the level of C6, the CCA can be compressed against the carotid tubercle (Chassaignac's tubercle)
- At the level of C4 (superior margin of the thyroid cartilage), it bifurcates into the Internal Carotid Artery (ICA) and External Carotid Artery (ECA)
- The carotid sinus (baroreceptor) is a dilation at the proximal ICA; the carotid body (chemoreceptor) sits at the bifurcation
- The CCA and ICA give no branches in the neck
(Color Atlas of Human Anatomy Vol. 2, p. 93; Fischer's Mastery of Surgery, p. 1114)
2. External Carotid Artery (ECA)
Initially lies anteromedial to the ICA; superiorly lies anterolateral. It terminates at the neck of the mandible (within the parotid gland) by dividing into two terminal branches. Its branches supply the neck, face, scalp, and cranial meninges.
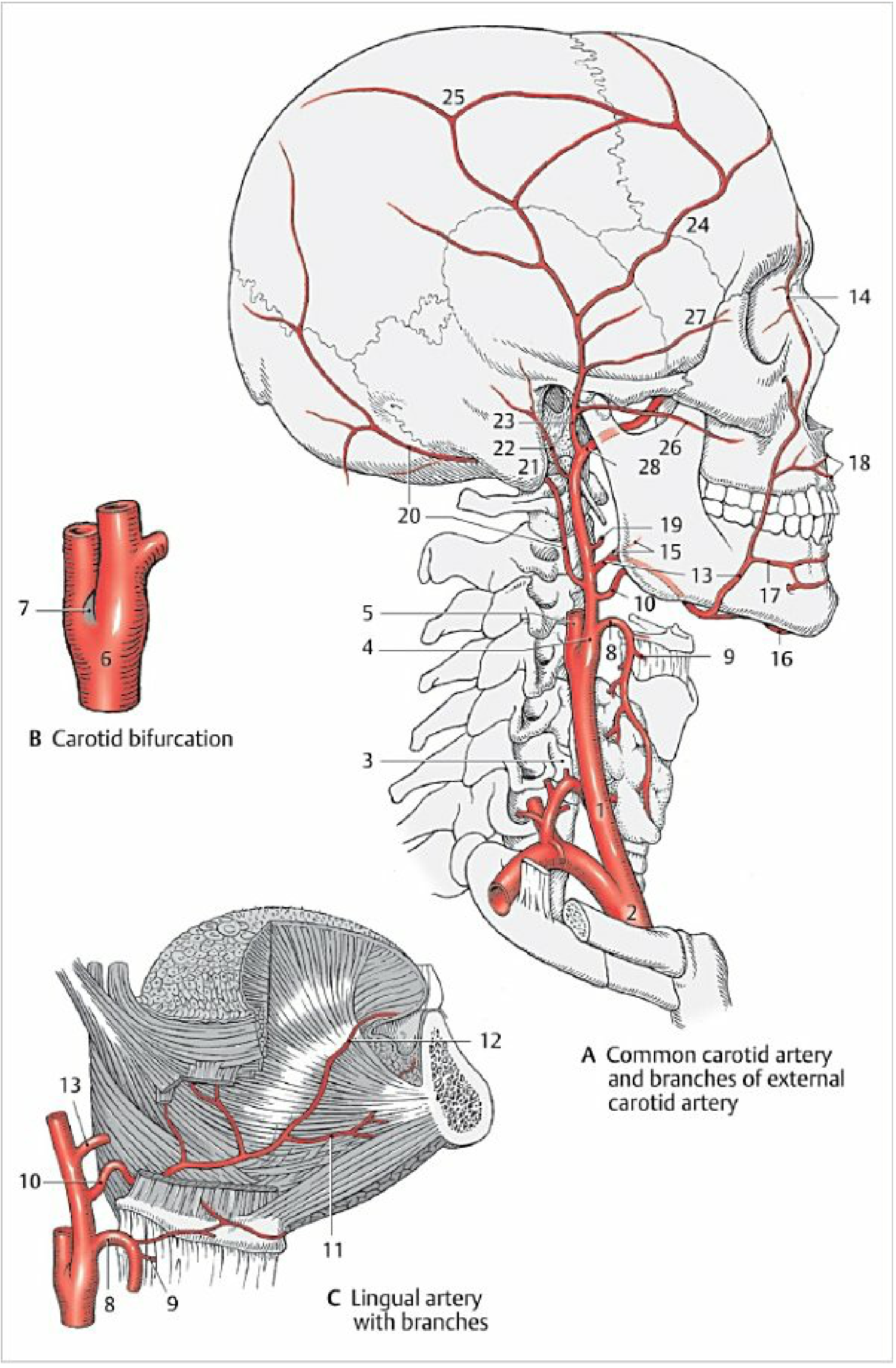
Anterior Branches (3)
| Artery | Origin level | Supply |
|---|---|---|
| Superior thyroid artery | Level of hyoid bone; first branch, close to bifurcation | Thyroid gland (superior), larynx (via superior laryngeal a.), cricothyroid, sternocleidomastoid |
| Lingual artery | Near greater horn of hyoid | Tongue (deep lingual a., sublingual a.) |
| Facial artery | Just above lingual artery | Face from mandible to medial canthus (angular a.); also ascending palatine, submental, inferior and superior labial branches |
Medial Branch (1)
| Artery | Supply |
|---|---|
| Ascending pharyngeal artery | Arises earliest (first or second branch); runs along lateral pharyngeal wall to skull base; supplies pharynx, prevertebral muscles, middle ear, cranial meninges (posterior meningeal a., inferior tympanic a.) |
Posterior Branches (3)
| Artery | Supply |
|---|---|
| Sternocleidomastoid artery | Sternocleidomastoid muscle |
| Occipital artery | Posterior scalp; passes in occipital groove medial to mastoid process |
| Posterior auricular artery | Between mastoid and auricle; supplies parotid gland, facial nerve, temporal bone, auricle, scalp (branches: stylomastoid a., posterior tympanic a.) |
Terminal Branches (2)
| Artery | Supply |
|---|---|
| Superficial temporal artery | Scalp of temporal and frontal regions (frontal and parietal branches); also transverse facial artery and zygomatico-orbital artery |
| Maxillary artery | Deep face, teeth, dura, nasal cavity (see below) |
Memory aid: "Some Anatomists Like Freaking Out Poor Medical Students" = Superior thyroid, Ascending pharyngeal, Lingual, Facial, Occipital, Posterior auricular, Maxillary, Superficial temporal
3. Maxillary Artery (Largest Terminal Branch of ECA)
Arises posterior to the neck of the mandible. Divided into three parts by the lateral pterygoid muscle:
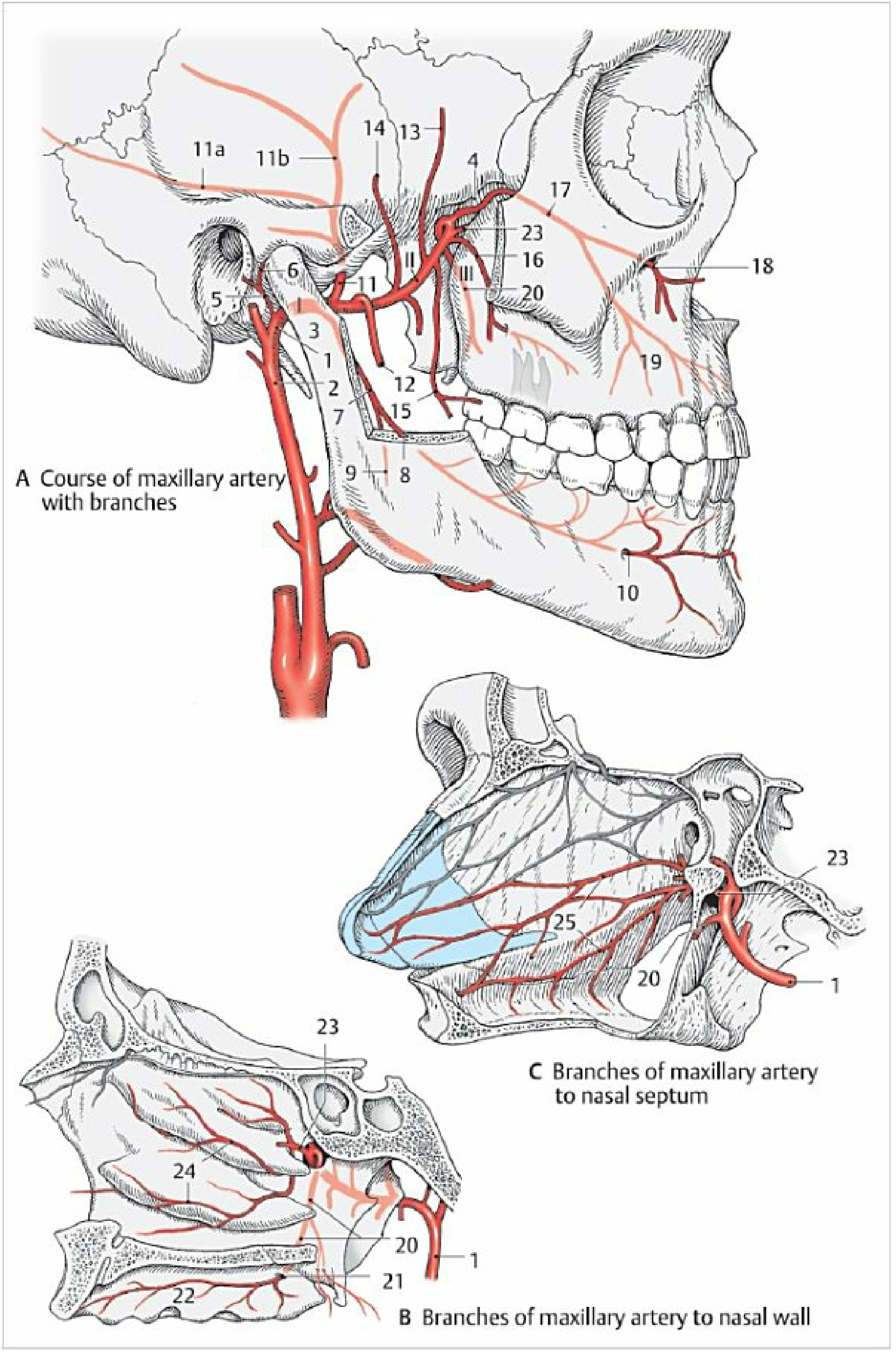
Part I - Mandibular (behind neck of mandible)
- Deep auricular artery - TMJ, external acoustic meatus, tympanic membrane
- Anterior tympanic artery - tympanic cavity
- Middle meningeal artery - passes through foramen spinosum; largest artery to dura mater; frontal and parietal branches
- Inferior alveolar artery - enters mandibular canal; supplies teeth and bone of mandible; terminates as mental branch
Part II - Pterygoid (near masticatory muscles)
- Masseteric artery, deep temporal arteries (anterior + posterior), pterygoid branches - masticatory muscles
- Buccal artery - buccal mucosa; anastomoses with facial artery
Part III - Pterygomaxillary (pterygopalatine fossa)
- Posterior superior alveolar artery - maxillary sinus, upper posterior teeth
- Infraorbital artery - passes through inferior orbital fissure and infraorbital canal; supplies face; gives anterior superior alveolar arteries (upper anterior teeth)
- Descending palatine artery → greater palatine a. (hard palate) + lesser palatine arteries (soft palate)
- Artery of pterygoid canal - auditory tube, pharynx
- Sphenopalatine artery (terminal branch) - nasal cavity (posterior lateral nasal arteries, posterior septal branches)
(Color Atlas of Human Anatomy Vol. 2, pp. 97-98)
4. Internal Carotid Artery (ICA)
Gives no branches in the neck. Divided into four parts:
| Part | Location | Key Branches |
|---|---|---|
| Cervical (I) | Carotid bifurcation → skull base | None |
| Petrous (II) | Carotid canal in petrous bone | Caroticotympanic arteries (tympanic cavity) |
| Cavernous (III) | Within cavernous sinus; forms carotid siphon | Inferior hypophysial artery (neurohypophysis), meningeal branches, branches to trigeminal ganglion |
| Cerebral (IV) | Medial to anterior clinoid process | Ophthalmic artery (first branch - eye, orbit, forehead), posterior communicating artery (to posterior circulation), anterior choroidal artery, then divides into anterior cerebral artery and middle cerebral artery |
(Color Atlas of Human Anatomy Vol. 2, pp. 99-100)
5. Subclavian Artery Contribution
The vertebral artery arises from the subclavian artery and ascends through the foramina transversaria of C6-C1, then passes through the foramen magnum. The two vertebral arteries unite on the clivus to form the basilar artery. Together they supply the posterior circulation (brainstem, cerebellum, posterior cortex) and meet the anterior circulation at the Circle of Willis.
Vertebral artery branches:
- Posterior spinal artery
- Anterior spinal artery
- Posterior inferior cerebellar artery (PICA)
Basilar artery branches:
- Anterior inferior cerebellar artery (AICA)
- Superior cerebellar artery (SCA)
- Pontine branches
- Posterior cerebral artery (terminal) - joins circle of Willis via posterior communicating artery
The thyrocervical trunk (from subclavian) contributes to the neck via the inferior thyroid artery (thyroid, larynx, trachea, esophagus) and superficial cervical/suprascapular arteries (posterior neck muscles and scalp).
6. Circle of Willis (Summary)
The anterior and posterior circulations anastomose at the circle of Willis around the sella turcica:
- Anterior communicating artery - connects the two anterior cerebral arteries
- Posterior communicating artery (bilateral) - connects ICA to posterior cerebral artery
This provides collateral flow if any major vessel is occluded.
Sources: Fischer's Mastery of Surgery 8e, p. 1114; Color Atlas of Human Anatomy Vol. 2, pp. 93-100; Gray's Anatomy for Students; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Wht is artery and how it is formed and uses
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have rich textbook content to compile a complete answer.
What is an Artery?
An artery is a blood vessel that carries blood away from the heart to the tissues and organs of the body. With the exception of the pulmonary arteries (which carry deoxygenated blood to the lungs), arteries carry oxygenated, nutrient-rich blood under high pressure.
How an Artery is Formed (Development / Embryology)
Arteries develop during the third week of embryonic life from mesoderm (the middle germ layer). This happens through two processes:
1. Vasculogenesis
- Mesoderm cells are stimulated by FGF2 (fibroblast growth factor 2) to form hemangioblasts (a common precursor for blood vessels and blood cells)
- Hemangioblasts then respond to VEGF (Vascular Endothelial Growth Factor) and become angioblasts (vessel-forming cells)
- Angioblasts cluster together to form blood islands
- Small cavities open up within these blood islands
- Angioblasts flatten into endothelial cells that line these cavities
- These cavities fuse into networks of endothelial-lined channels - this forms the first primitive vessels
2. Angiogenesis
- New vessels sprout and branch from the already-existing primitive vessels
- Also regulated by VEGF (stimulates endothelial cell proliferation at budding points)
- Final vessel stabilization is achieved by PDGF and TGF-β
3. Wall Formation
- After the initial endothelial tube is formed, surrounding mesenchymal cells differentiate and wrap around it to form the muscular and connective tissue layers of the arterial wall
- The cardiovascular system is the first organ system to become functional - the heart begins beating on day 21-22 of embryonic life
(The Developing Human - Clinically Oriented Embryology; Langman's Medical Embryology)
Structure of an Artery (Wall Layers)
Every artery has three concentric layers (tunics):
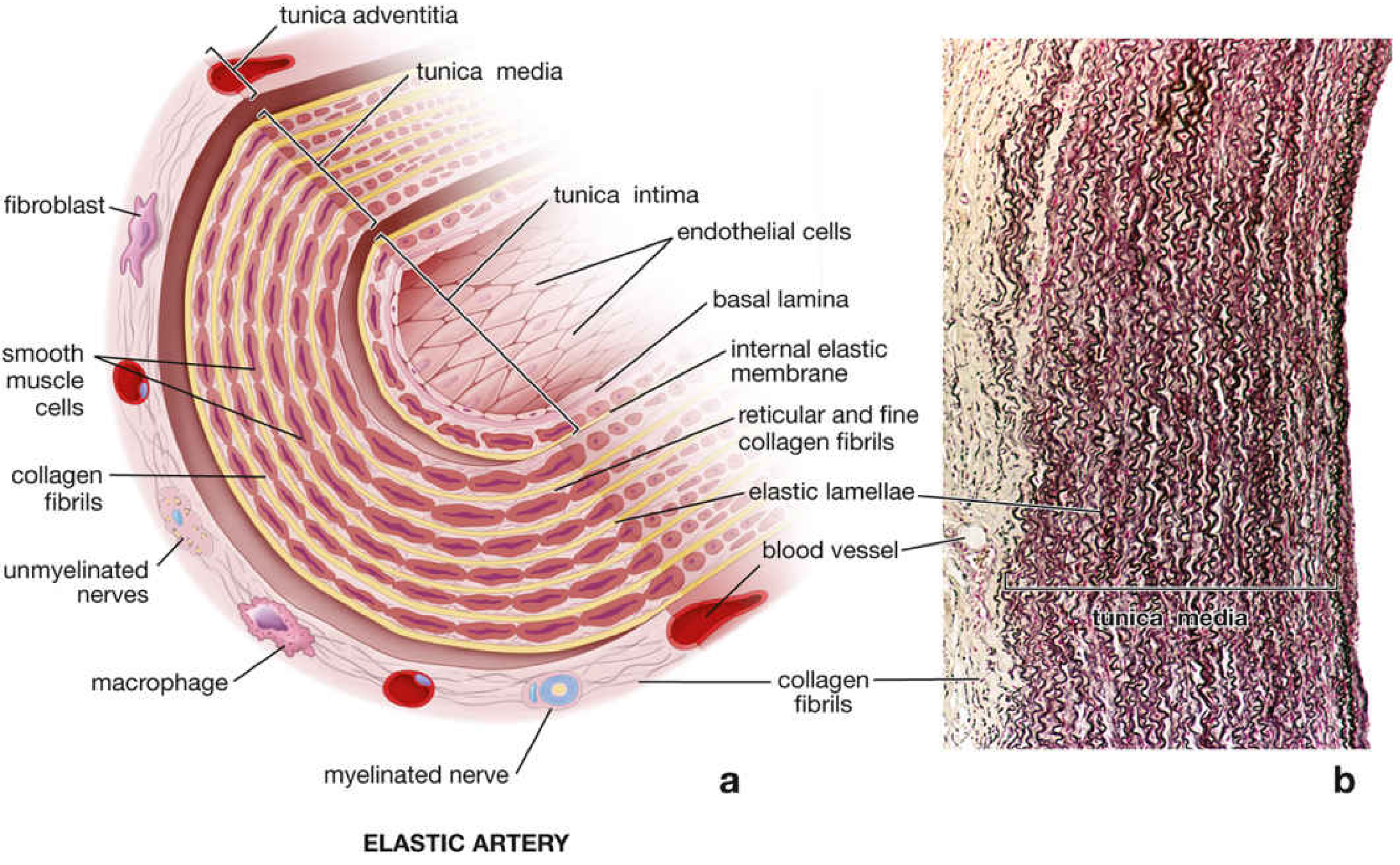
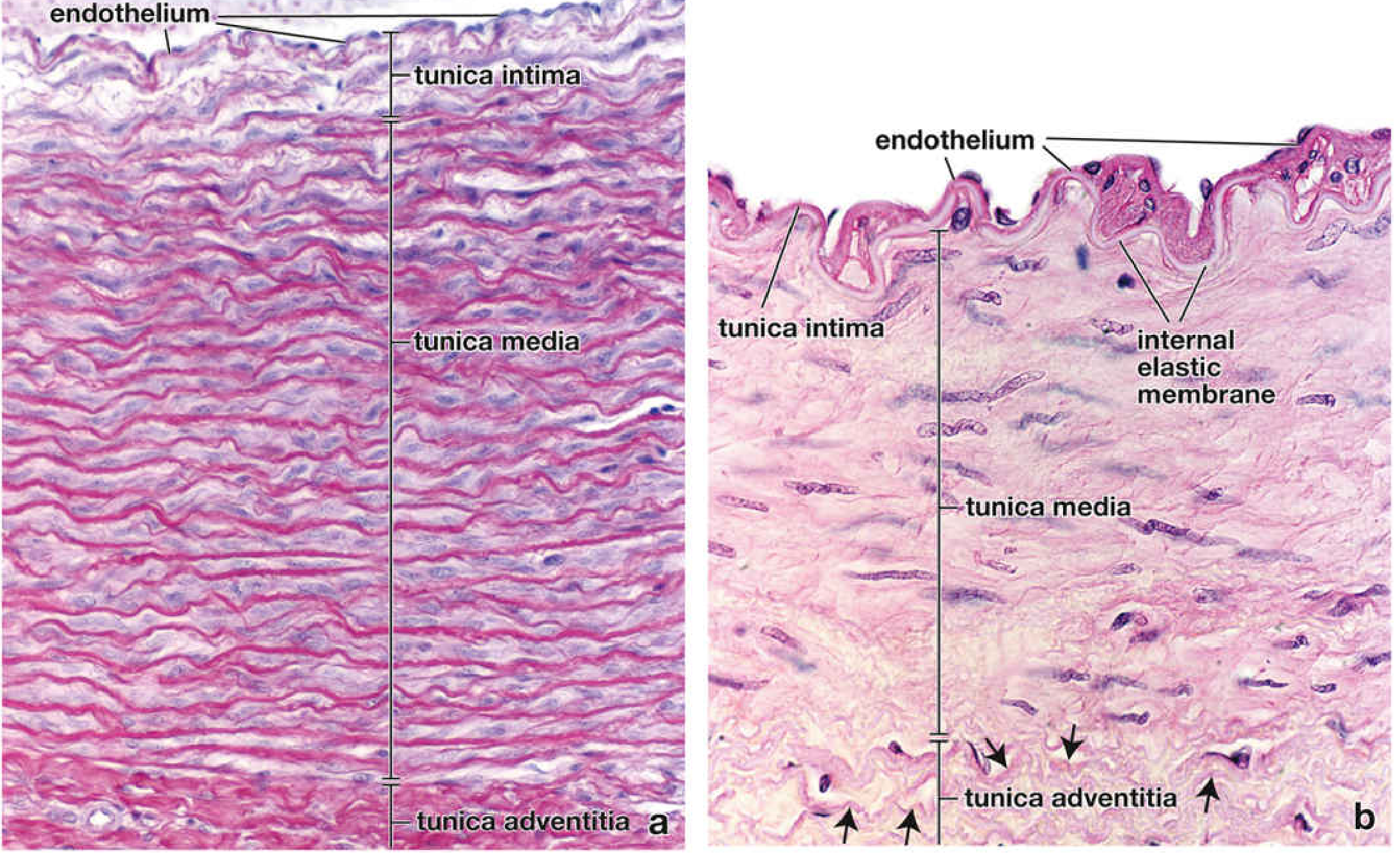
Layer 1 - Tunica Intima (innermost)
- Single layer of endothelial cells (flat, elongated, oriented along blood flow direction)
- Rests on a basal lamina and thin subendothelial connective tissue
- Endothelial cells are joined by tight junctions and gap junctions
- Contains Weibel-Palade bodies (store von Willebrand factor and P-selectin)
- Separated from tunica media by the internal elastic membrane
Layer 2 - Tunica Media (middle - thickest)
- Made of circularly arranged smooth muscle cells (appear spiral in cross-section)
- Contains collagen fibers, elastic fibers/lamellae, and proteoglycans
- Smooth muscle cells synthesize collagen, elastin, and ECM molecules
- Number of elastic lamellae relates to blood pressure (more lamellae = higher pressure)
- Bounded on its outer side by the external elastic membrane (prominent in muscular arteries)
Layer 3 - Tunica Adventitia (outermost)
- Loose connective tissue (collagen + elastic fibers)
- Contains fibroblasts and macrophages
- Contains vasa vasorum - small blood vessels that supply nutrients/oxygen to the arterial wall itself
- Contains nervi vasorum - sympathetic nerve fibers that release norepinephrine to cause vasoconstriction
(Histology: A Text and Atlas, pp. 1088-1094)
Types of Arteries
| Type | Size | Key Feature | Example |
|---|---|---|---|
| Elastic (conducting) arteries | Large | Many elastic lamellae in media; expand during systole and recoil during diastole | Aorta, pulmonary trunk, common carotid |
| Muscular (distributing) arteries | Medium | Prominent smooth muscle in media; prominent internal elastic membrane; regulate blood flow to organs | Coronary, femoral, radial arteries |
| Arterioles | Small (< 0.5 mm) | Mainly smooth muscle; control blood pressure and flow into capillaries | Arterioles in kidney, gut, skin |
Functions / Uses of Arteries
| Function | How |
|---|---|
| Transport oxygenated blood | Carry O₂ and nutrients from heart/lungs to all tissues |
| Maintain blood pressure | Thick muscular walls withstand and sustain high pressure generated by the heart |
| Windkessel effect | Large elastic arteries expand during systole (storing energy) and recoil during diastole (maintaining continuous flow even when heart is relaxed) |
| Regulate blood distribution | Muscular arteries constrict or dilate (via smooth muscle controlled by sympathetic nerves) to direct blood to where it is needed |
| Control peripheral resistance | Arterioles are the main site of blood pressure regulation - their constriction raises BP, dilation lowers it |
| Prevent backflow | Arterial valves (aortic and pulmonary) close when elastic recoil pushes blood backward toward the heart |
| Nutrient supply to wall itself | Vasa vasorum (in larger arteries) supply the arterial wall's own cells |
Artery vs. Vein - Key Differences
| Feature | Artery | Vein |
|---|---|---|
| Blood direction | Away from heart | Toward heart |
| Blood oxygen | Oxygenated (usually) | Deoxygenated (usually) |
| Wall thickness | Thick (high pressure) | Thin (low pressure) |
| Tunica media | Dominant, muscular/elastic | Thin |
| Tunica adventitia | Thinner than media | Dominant layer |
| Valves | None (except at heart) | Present (prevent backflow) |
| Lumen | Smaller, rounder | Larger, irregular |
Sources: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina), pp. 1088-1094; The Developing Human - Clinically Oriented Embryology (Moore), pp. 218-219; Langman's Medical Embryology, p. 104-105
How do arteries control blood pressure and blood flow?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
I now have all the key information needed. Let me compile the full comprehensive answer.
How Arteries Control Blood Pressure and Blood Flow
Arterial control of blood pressure and blood flow operates at multiple levels simultaneously - from the physical properties of the vessel wall, to local chemical signals, to neural reflexes and hormones.
The Core Principle: Ohm's Law for Blood Flow
Blood flow follows a relationship analogous to Ohm's Law in electricity:
Blood Flow (Q) = Pressure Gradient (ΔP) ÷ Vascular Resistance (R)
This means arteries control flow by changing either pressure or resistance. Since resistance is inversely proportional to the 4th power of the vessel radius (Poiseuille's Law), even a small change in arterial diameter produces a huge change in resistance and flow. Arterioles - the smallest muscular arteries - are the main site of resistance regulation.
Mechanism 1 - Elastic Recoil (Windkessel Effect)
Where: Large elastic arteries (aorta, pulmonary trunk, common carotid)
- During systole (heart contraction), blood is ejected at high pressure into the aorta. The elastic walls stretch and store energy like a balloon.
- During diastole (heart relaxation), no blood is ejected from the heart. The elastic walls recoil, converting stored energy back into forward blood flow.
- This converts the pulsatile pump output of the heart into a more continuous, smooth flow through the smaller vessels.
- Without this, blood pressure would drop to zero between heartbeats.
(Histology: A Text and Atlas, p. 1088)
Mechanism 2 - Neural Control (Baroreceptor Reflex)
Where: Arterioles and muscular arteries throughout the body
This is the most important short-term mechanism.
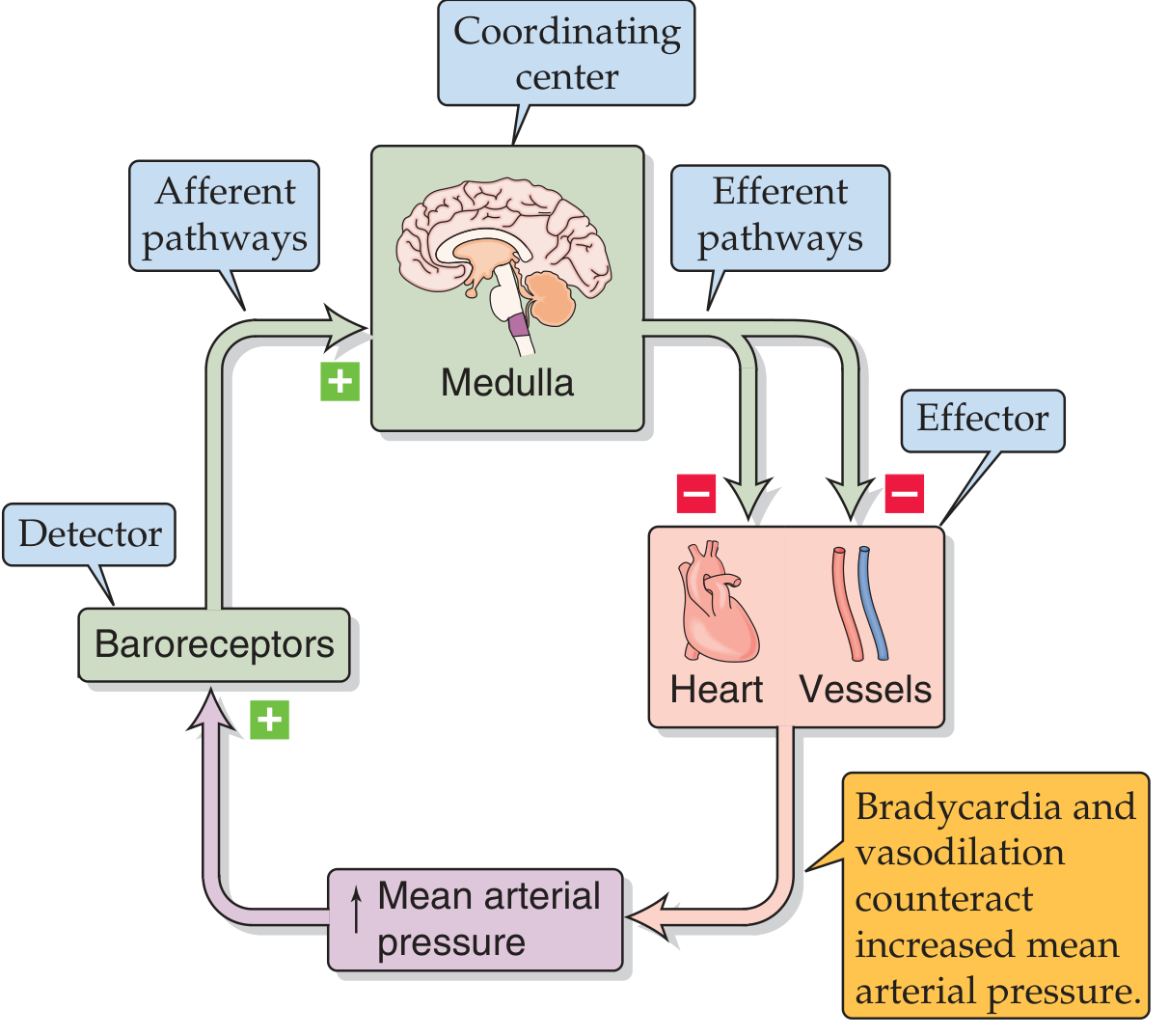
How it works:
- Baroreceptors (stretch receptors) in the carotid sinus and aortic arch detect arterial wall stretch (= pressure change)
- Signals travel via afferent nerves to the medullary cardiovascular center
- The medulla adjusts sympathetic and parasympathetic outflow:
| Situation | Response |
|---|---|
| BP rises | Baroreceptors fire more → medulla inhibits sympathetic output → vasodilation + bradycardia → BP falls back to normal |
| BP falls | Baroreceptors fire less → medulla increases sympathetic output → vasoconstriction + tachycardia → BP rises back to normal |
- Postganglionic sympathetic fibers run alongside blood vessels and innervate both muscular arteries and arterioles
- They release norepinephrine, which binds α1 receptors on smooth muscle → vasoconstriction
- Severing the spinal cord above T1 causes a severe fall in BP because the sympathetic outflow to vessels is cut
(Medical Physiology, p. 781-786)
Mechanism 3 - Local (Intrinsic) Control
These mechanisms allow each organ to regulate its own blood supply independently of the nervous system.
A. Myogenic Mechanism
- Vascular smooth muscle cells (VSMCs) respond directly to stretch from increased pressure
- Increased transmural pressure → VSMCs stretch → vasoconstriction (protects capillaries from pressure damage)
- Decreased pressure → vasodilation (increases flow when supply falls)
- Important in: brain, heart, skeletal muscle, kidneys (autoregulation)
B. Metabolic Mechanism
- Active tissues produce metabolic byproducts that act directly on VSMCs to cause vasodilation, matching blood flow to metabolic demand:
| Metabolic Signal | Effect |
|---|---|
| ↓ PO₂ (low oxygen) | Vasodilation |
| ↑ PCO₂ / ↓ pH | Vasodilation |
| ↑ Extracellular K⁺ | Vasodilation |
| ↑ Adenosine | Vasodilation |
- This is how exercising muscle or an active brain automatically receives more blood
C. Endothelial Mechanism - Nitric Oxide (NO)
- Endothelial cells lining arteries are not passive tubes - they actively release vasoactive substances
- Shear stress from flowing blood → endothelial cells release Nitric Oxide (NO)
- NO is synthesized from L-arginine by NOS3 (endothelial nitric oxide synthase)
- NO diffuses into adjacent smooth muscle → activates soluble guanylyl cyclase → produces cGMP → smooth muscle relaxation → vasodilation
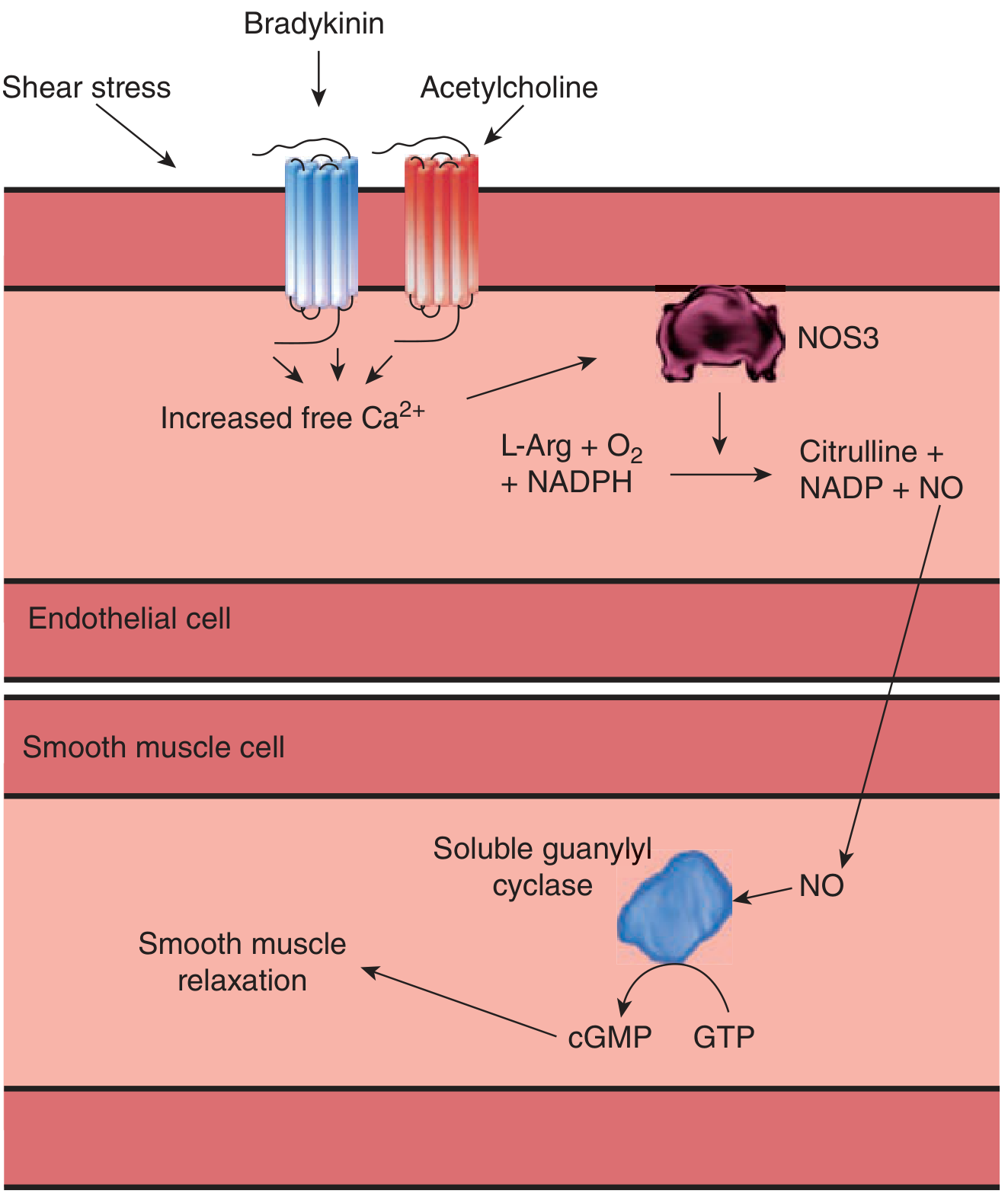
- Stimuli for NO release: shear stress, acetylcholine, bradykinin, VIP, substance P
- Mice lacking NOS3 are chronically hypertensive, proving tonic NO release is essential for normal BP
- Nitroglycerin (used in angina) works by mimicking NO → dilates coronary arteries
(Ganong's Review of Medical Physiology, pp. 594-595)
Mechanism 4 - Hormonal Control (Long-term)
These regulate blood pressure over hours to days.
Renin-Angiotensin-Aldosterone System (RAAS)
- When BP falls, the kidney releases renin → converts angiotensinogen to angiotensin I → ACE converts it to angiotensin II
- Angiotensin II causes direct vasoconstriction of arterioles → raises total peripheral resistance (TPR) → raises BP
- Angiotensin II also stimulates aldosterone release → increases Na⁺ reabsorption in kidney → increases blood volume → raises BP
- ACE inhibitors (e.g. ramipril) and angiotensin receptor blockers (ARBs) block this pathway to treat hypertension
(Costanzo Physiology 7e, p. 739)
Antidiuretic Hormone (ADH / Vasopressin)
- Released by posterior pituitary when BP falls or plasma osmolarity rises
- Acts on V1 receptors in vascular smooth muscle → arteriolar vasoconstriction → raises TPR
- Acts on V2 receptors in kidney → water retention → raises blood volume
Atrial Natriuretic Peptide (ANP)
- Released by atria when blood volume is too high
- Causes vasodilation and promotes Na⁺/water excretion → reduces blood volume and BP
Summary Table
| Mechanism | Location | Trigger | Effect on BP | Time Scale |
|---|---|---|---|---|
| Elastic recoil | Large elastic arteries | Systole/diastole | Smooths pressure waves | Beat by beat |
| Baroreceptor reflex | All arterioles | Stretch (pressure change) | Corrects deviation | Seconds |
| Myogenic | Muscular arteries, arterioles | Wall stretch | Autoregulation | Seconds |
| Metabolic (O₂, CO₂, K⁺) | Local arterioles | Tissue activity | Matches flow to demand | Seconds-minutes |
| Nitric oxide (NO) | All arteries/arterioles | Shear stress, ACh | Vasodilation | Seconds-minutes |
| RAAS (Angiotensin II) | All arterioles | ↓ BP, ↓ renal flow | Vasoconstriction | Hours-days |
| ADH | Arterioles, kidney | ↓ BP, ↑ osmolarity | Vasoconstriction + volume | Hours |
| ANP | Arterioles, kidney | ↑ Blood volume | Vasodilation + diuresis | Hours |
Sources: Medical Physiology (Boron & Boulpaep), pp. 781-786, 816; Ganong's Review of Medical Physiology 26e, pp. 594-595; Costanzo Physiology 7e, pp. 738-742; Histology: A Text and Atlas (Pawlina), p. 1088
Why bp is measured in artery not veins
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed for a thorough, well-sourced answer.
Why is Blood Pressure Measured in Arteries, Not Veins?
There are several deeply interconnected reasons - all rooted in the fundamental differences between how arteries and veins function.
Reason 1 - Arteries Have High, Measurable Pressure; Veins Do Not
The entire cardiovascular system runs on a pressure gradient. Blood flows from high pressure to low pressure:
| Vessel | Typical Pressure |
|---|---|
| Aorta (leaving heart) | ~120 / 80 mmHg |
| Large arteries | ~110 / 70 mmHg |
| Arterioles | ~40-60 mmHg |
| Capillaries | ~15-35 mmHg |
| Venules | ~10-15 mmHg |
| Large veins | ~5-8 mmHg |
| Right atrium (vena cava entry) | ~0-2 mmHg |
By the time blood reaches the veins, almost all the pressure energy generated by the heart has been spent overcoming resistance in the arterioles and capillaries. Venous pressure is so low it cannot even be reliably detected by a standard cuff - there is simply nothing meaningful to measure for clinical purposes.
Reason 2 - Arteries Are Pulsatile; Veins Are Not
The rhythmic contraction of the left ventricle ejects blood into the arterial tree in pulses. This creates two distinct, clinically meaningful values:
- Systolic pressure (peak, during contraction) - ~120 mmHg
- Diastolic pressure (lowest, during relaxation) - ~80 mmHg
- Pulse pressure = Systolic - Diastolic (normally ~40 mmHg)
"The rhythmic contraction of the left ventricle, ejecting blood into the arterial tree, results in pulsatile arterial pressures. The peak left ventricular end-systolic pressure approximates the systolic arterial blood pressure; the lowest arterial pressure during diastolic relaxation is the diastolic blood pressure." (Morgan & Mikhail's Clinical Anesthesiology 7e)
Veins, by contrast, carry blood at steady, non-pulsatile, near-zero pressure back to the heart. There is no systolic/diastolic cycle to detect in a vein. The entire concept of a BP reading (e.g. "120/80") only makes sense in an artery.
Reason 3 - How the BP Measurement Actually Works
Standard BP measurement relies on the pulsatile nature of arterial flow. The sphygmomanometer cuff is placed over an artery (classically the brachial artery) and works as follows:
- The cuff is inflated above systolic pressure → completely blocks blood flow → artery is occluded → no sound
- As cuff pressure is slowly released and falls below systolic pressure → a spurt of blood squirts through with each heartbeat → creates turbulent flow → you hear Korotkoff sounds (tapping) through the stethoscope
- The pressure at which sounds first appear = Systolic BP
- As cuff pressure falls further, sounds change character (louder → muffled)
- The pressure at which sounds disappear = Diastolic BP
"The sounds of Korotkoff are produced by turbulent flow in the brachial artery. When the artery is narrowed by the cuff, the velocity of flow exceeds the critical velocity and turbulent flow results." (Ganong's Review of Medical Physiology 26e)
This entire mechanism depends on:
- The artery having enough pressure to be occluded by the cuff then reopened
- Intermittent pulsatile blood flow producing identifiable sounds
- Neither of these things happens in a vein - veins have too little pressure to be meaningfully occluded and reopened, and produce no audible turbulent pulse
Reason 4 - Arteries Reflect the Heart's Actual Output
Arterial BP is a direct indicator of cardiac function and organ perfusion:
- Systolic BP reflects: stroke volume, ejection force of the heart, arterial stiffness
- Diastolic BP reflects: peripheral vascular resistance and arterial compliance
- Mean Arterial Pressure (MAP) = (SBP + 2×DBP) / 3 = best predictor of organ perfusion
- Pulse pressure = reflects stroke volume and large-artery stiffness
Venous pressure (measured as Central Venous Pressure / CVP) is a completely separate measurement done invasively via a catheter in a large central vein - and it tells you about venous return and right heart filling, not cardiac output or systemic BP.
Reason 5 - Practical Accessibility
The brachial artery (in the upper arm) is ideal for BP measurement because:
- It is large, superficial, and easily accessible
- It lies directly under the BP cuff
- Its pressure closely reflects central aortic pressure
- Korotkoff sounds are clearly audible over it
Veins in the same location (e.g. cephalic, basilic veins) have such low, near-zero pressure that no meaningful occlusion or sound production is possible with a standard cuff.
Summary: Arteries vs. Veins for BP
| Feature | Artery | Vein |
|---|---|---|
| Pressure | High (80-120 mmHg) | Very low (2-10 mmHg) |
| Flow pattern | Pulsatile (systole/diastole) | Steady, non-pulsatile |
| Wall thickness | Thick - resists high pressure | Thin |
| Measurable with cuff? | YES - can be occluded and released | NO - pressure too low |
| Korotkoff sounds? | YES - turbulent flow audible | NO - no turbulence |
| Clinical information | Cardiac output, vascular resistance, organ perfusion | Venous return, right heart filling |
| Standard BP measurement | Brachial artery (indirect) or radial artery (direct) | Not used for standard BP |
Sources: Ganong's Review of Medical Physiology 26e, pp. 2298-2320; Morgan & Mikhail's Clinical Anesthesiology 7e, p. 154; Schwartz's Principles of Surgery 11e, pp. 462-463; Comprehensive Clinical Nephrology 7e, p. 495
This is a shared conversation. Sign in to Orris to start your own chat.