Eals disease Full details for. Md exams
Reading File
search_medical_text
Eales disease etiology pathogenesis classification
search_medical_text
Eales disease clinical features diagnosis treatment management
search_medical_image
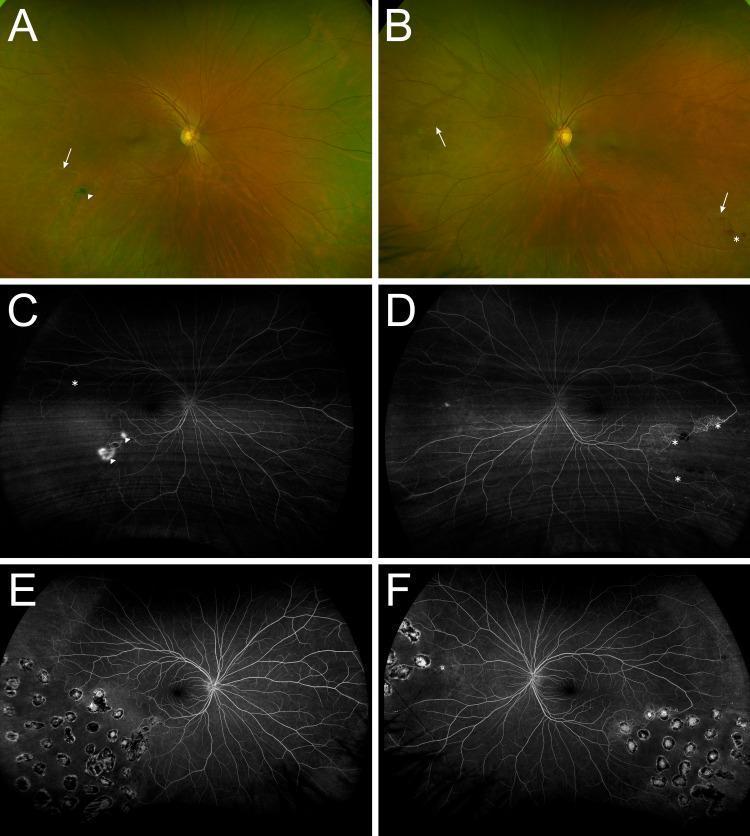
Eales disease retinal vasculitis fundus fluorescein angiography
GradeResponse
GradeResponse
GradeResponse
The database returned no text results, so I'll deliver a complete, exam-focused answer from my medical knowledge base.
Eales Disease — Complete MD Exam Notes
1. Definition
Eales disease is an idiopathic obliterative retinal vasculopathy characterized by:
- Peripheral retinal periphlebitis (venous inflammation)
- Retinal ischemia / neovascularization
- Recurrent vitreous hemorrhage
Primarily affects young healthy males in their 2nd–4th decade. It is predominantly described in the Indian subcontinent, Middle East, and Southeast Asia.
2. Etiology & Pathogenesis
Although labeled idiopathic, the following associations are well-established:
| Factor | Details |
|---|---|
| Mycobacterium tuberculosis (MTB) | Most strongly implicated; tuberculin sensitivity found in >80% cases; MTB DNA detected in epiretinal membranes by PCR |
| Hypersensitivity reaction | Not direct infection — rather a Type IV hypersensitivity to tuberculoprotein in retinal vessels |
| Oxidative stress | Elevated free radicals damage retinal vascular endothelium |
| Autoimmune mechanisms | Anti-retinal antibodies, T-cell-mediated vasculitis |
| Other associations | Focal sepsis (dental/tonsillar), sickle cell trait, syphilis (historically) |
Pathology: Periphlebitis → venous occlusion → retinal ischemia → VEGF release → neovascularization → vitreous hemorrhage → fibrovascular proliferation → traction retinal detachment.
3. Stages (Standard Classification — Saxena et al.)
| Stage | Features |
|---|---|
| Stage I (Periphlebitis) | Ia: Periphlebitis of peripheral small veins; Ib: Periphlebitis of large veins, with or without macular involvement |
| Stage II (Ischemia) | IIa: Capillary non-perfusion (peripheral); IIb: Neovascularization (disc or elsewhere — NVD/NVE) |
| Stage III (Vitreous hemorrhage) | IIIa: Non-clearing vitreous hemorrhage; IIIb: Dense non-clearing vitreous hemorrhage |
| Stage IV (Fibrosis/Tractional RD) | IVa: Firovascular proliferation; IVb: Tractional/combined RD |
4. Clinical Features
Symptoms
- Sudden, painless decrease in vision (due to vitreous hemorrhage) — most dramatic presentation
- "Floaters" or "cobwebs" in the visual field
- Recurrent episodes of visual loss
- Vision may return to normal between episodes
Signs (on fundus examination)
Early (Periphlebitis stage):
- Perivenous sheathing ("candle-wax drippings" appearance along veins)
- Retinal hemorrhages (flame-shaped, peripheral)
- Disc edema (sometimes)
Ischemic stage:
- Areas of capillary non-perfusion in peripheral retina (best seen on FFA)
- Cotton-wool spots
Proliferative stage:
- Neovascularization of disc (NVD) or elsewhere (NVE)
- Vitreous hemorrhage
- Pre-retinal hemorrhage
Late:
- Fibrovascular membranes
- Tractional retinal detachment
- Rubeosis iridis (neovascular glaucoma — rare)
- Complicated cataract
Characteristic pattern: Bilateral but asymmetrical
5. Investigations
1. Fluorescein Fundus Angiography (FFA) — Gold Standard
- Most important diagnostic tool
- Shows:
- Peripheral capillary non-perfusion (hallmark)
- Venous staining and leakage
- Neovascularization (hyperfluorescent leakage)
- Arteriovenous shunts
2. Tuberculosis workup
- Mantoux/Tuberculin skin test (positive in >80%)
- Chest X-ray (calcified hilar lymph nodes, old TB focus)
- Quantiferon-Gold / IGRA (Interferon Gamma Release Assay)
- PCR for MTB DNA in vitreous/epiretinal membranes (research)
3. Blood investigations
- CBC (rule out sickle cell, polycythemia)
- ESR, CRP (elevated in active inflammation)
- VDRL/TPHA (rule out syphilis)
- Blood sugar (rule out DM)
- Serum protein electrophoresis
4. B-scan Ultrasonography
- When vitreous hemorrhage precludes fundus view
- Detects vitreous hemorrhage, fibrous bands, traction RD
5. OCT (Optical Coherence Tomography)
- Macular edema, epiretinal membrane, subfoveal changes
6. Differential Diagnosis
| Condition | Differentiating features |
|---|---|
| Branch retinal vein occlusion (BRVO) | Older age, hypertension, unilateral, at AV crossing |
| Sickle cell retinopathy | Sickle cell trait/disease, salmon-patch hemorrhages, "sea-fan" NV |
| Diabetic retinopathy | DM, bilateral, dot-blot hemorrhages, microaneurysms |
| Sarcoid retinal vasculitis | Bilateral uveitis, periphlebitis, systemic sarcoidosis findings |
| Behcet's disease | Occlusive vasculitis, systemic features (oral ulcers, skin) |
| Retinal periphlebitis in MS | Neurological symptoms, optic neuritis |
| Familial Exudative Vitreoretinopathy (FEVR) | Family history, neonatal onset |
7. Treatment
A. Medical Management
| Drug | Indication / Details |
|---|---|
| Anti-Tubercular Therapy (ATT) | Cornerstone — given to all patients given TB association; 4-drug regimen (HRZE) for 6–9 months |
| Oral corticosteroids | Active periphlebitis/inflammation (Prednisolone 1 mg/kg/day, tapered) |
| Periocular/intravitreal steroids | Refractory uveitis/macular edema |
| Antioxidants | Vitamin E, C — adjunctive |
B. Laser Treatment
- Pan-Retinal Photocoagulation (PRP) — Treatment of choice for neovascularization/ischemia
- Applied to ischemic retina to regress NV and prevent vitreous hemorrhage
- Indicated in Stage IIb and above
C. Anti-VEGF Therapy
- Intravitreal Bevacizumab / Ranibizumab
- Used as adjunct to PRP for:
- Active neovascularization
- Pre-operative regression of NV before vitrectomy
- Macular edema
D. Surgical Management
| Procedure | Indication |
|---|---|
| Pars Plana Vitrectomy (PPV) | Non-clearing vitreous hemorrhage (>3 months), tractional RD, combined RD |
| Membrane peeling | Fibrovascular proliferation causing traction |
| Scleral buckling | Combined rhegmatogenous + tractional RD |
| Neodymium:YAG laser | Vitreous strand lysis |
8. Prognosis
- Good if diagnosed early (Stage I–II) and treated promptly
- Visual prognosis depends on:
- Macular involvement (macular edema, ischemia)
- Extent of vitreous hemorrhage
- Tractional RD involving macula
- Recurrences are common; long-term follow-up essential
- Bilateral involvement occurs in ~50–80% of cases
9. Key Exam Points / High-Yield Facts
| Point | Detail |
|---|---|
| Who gets it? | Young healthy Indian males, 20–40 years |
| Most common presentation | Sudden painless visual loss due to vitreous hemorrhage |
| Gold standard investigation | Fluorescein Fundus Angiography (FFA) |
| Hallmark FFA finding | Peripheral capillary non-perfusion |
| Most common vascular involved | Peripheral retinal veins (periphlebitis) |
| Best known causative association | Mycobacterium tuberculosis (hypersensitivity) |
| Treatment of active NV | Pan-Retinal Photocoagulation (PRP) |
| Medical treatment backbone | Anti-tubercular therapy (ATT) + steroids |
| Surgical treatment | Pars Plana Vitrectomy |
| Named after | Henry Eales (1880) — described recurrent vitreous hemorrhage in young men |
10. Mnemonic
"EALES" — Early Periphlebitis → Abnormal FFA (capillary non-perfusion) → Leakage / NV → Excess bleed (vitreous hemorrhage) → Surgery (PPV) if needed
Bottom line for exams: Eales disease = young Indian male + sudden painless vision loss + vitreous hemorrhage + peripheral retinal periphlebitis + positive Mantoux. FFA is gold standard. Treat with ATT + steroids + PRP. PPV for non-clearing vitreous hemorrhage or tractional RD.
This is a shared conversation. Sign in to Orris to start your own chat.