Tell me about iodine deficiency for university exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete university-exam level answer.
Iodine Deficiency - Complete University Exam Guide
1. Introduction & Epidemiology
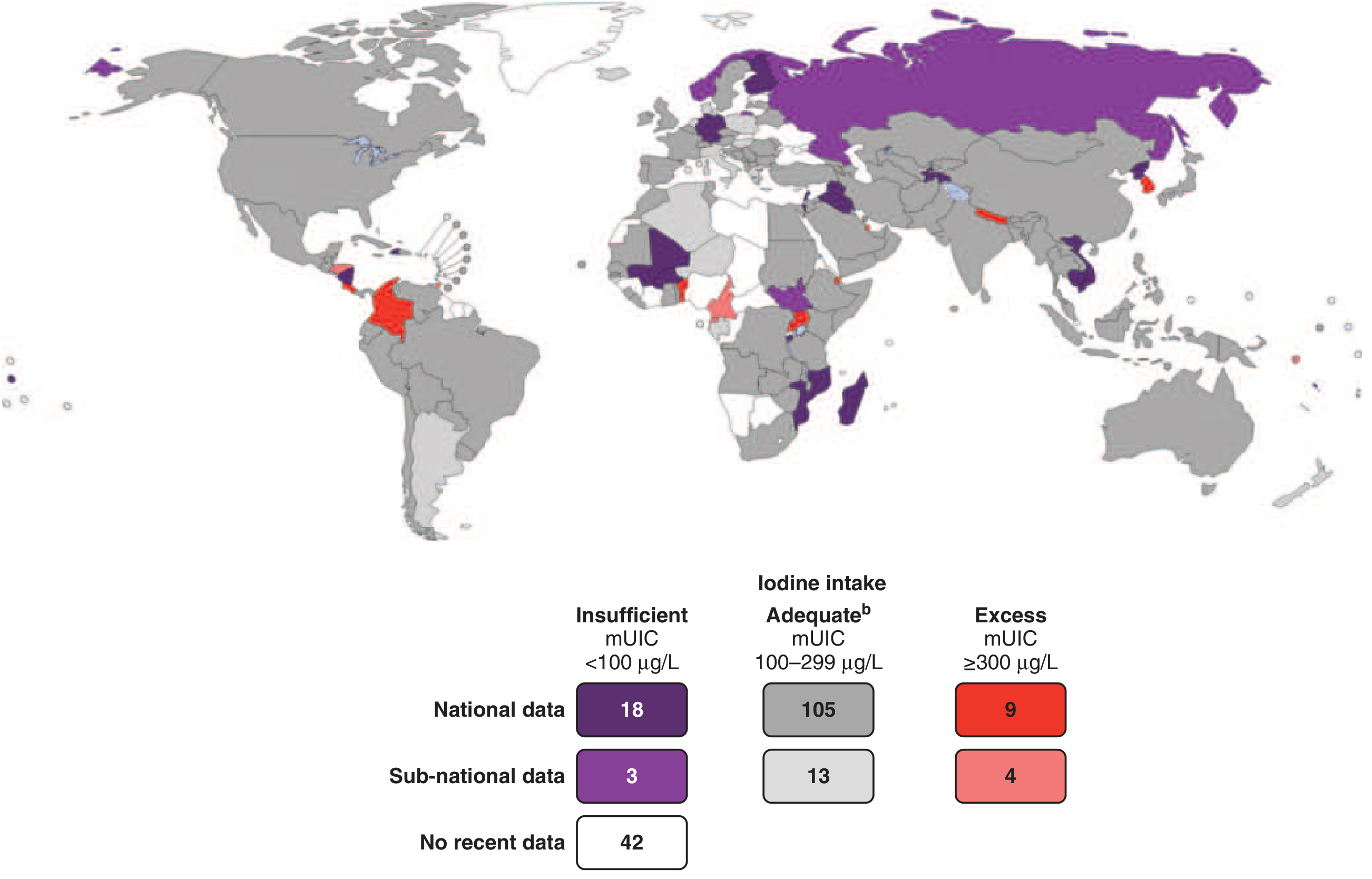
Iodine is a trace element essential for the synthesis of thyroid hormones (T3 and T4). The WHO estimates approximately 2 billion people are iodine-deficient worldwide, including ~285 million school-aged children. Deficiency is most prevalent in:
- Mountainous inland regions (Himalayas, Andes, Alps)
- Central Africa
- Northern and Central Asia
- Southeast Asia
Because seawater and seafood contain large amounts of iodide, deficiency is more common in landlocked populations relying on locally grown foods. Europe remains mildly iodine-deficient, and iodine intake has been falling in the United States and Australia.
The global distribution of iodine nutrition (from Harrison's 22E, 2025):
2. Role of Iodine in Thyroid Hormone Synthesis
Iodine is required for every step of thyroid hormone production:
- Iodide trapping - Active uptake of I⁻ from the blood into follicular cells via Na⁺/I⁻ symporter (NIS)
- Organification - Iodide is oxidized and attached to tyrosine residues on thyroglobulin (by thyroid peroxidase)
- Coupling - Monoiodotyrosine (MIT) + Diiodotyrosine (DIT) couple to form T3 and T4
- Secretion - Thyroglobulin is hydrolyzed and T3/T4 released into circulation
Daily requirement: 150 mcg/day for adults; 250 mcg/day during pregnancy (WHO recommendation).
3. Iodine Deficiency Disorders (IDD) - The Full Spectrum
The term "endemic goitre" has been replaced by Iodine Deficiency Disorders (IDD) because the consequences extend far beyond goitre. The spectrum, in approximate order of increasing severity (Park's Preventive & Social Medicine):
| Disorder | Manifestation/Severity |
|---|---|
| Goitre | Grade I, II, III, Multinodular |
| Hypothyroidism | Varying combinations of clinical signs by age, duration, severity |
| Subnormal intelligence | Variable severity |
| Delayed motor milestones | Variable |
| Mental deficiency | Variable |
| Hearing & speech defects | Variable |
| Strabismus (squint) | Unilateral or bilateral |
| Nystagmus | |
| Spasticity (extrapyramidal) | Muscle weakness, spastic diplegia, spastic quadriplegia |
| Endemic cretinism | Hypothyroid cretinism; Neurological cretinism |
| Intrauterine death | Spontaneous abortion, miscarriage |
Key exam point: The social impact of IDD arises not so much from goitre as from the effect on the central nervous system (Park's Preventive & Social Medicine, p. 720).
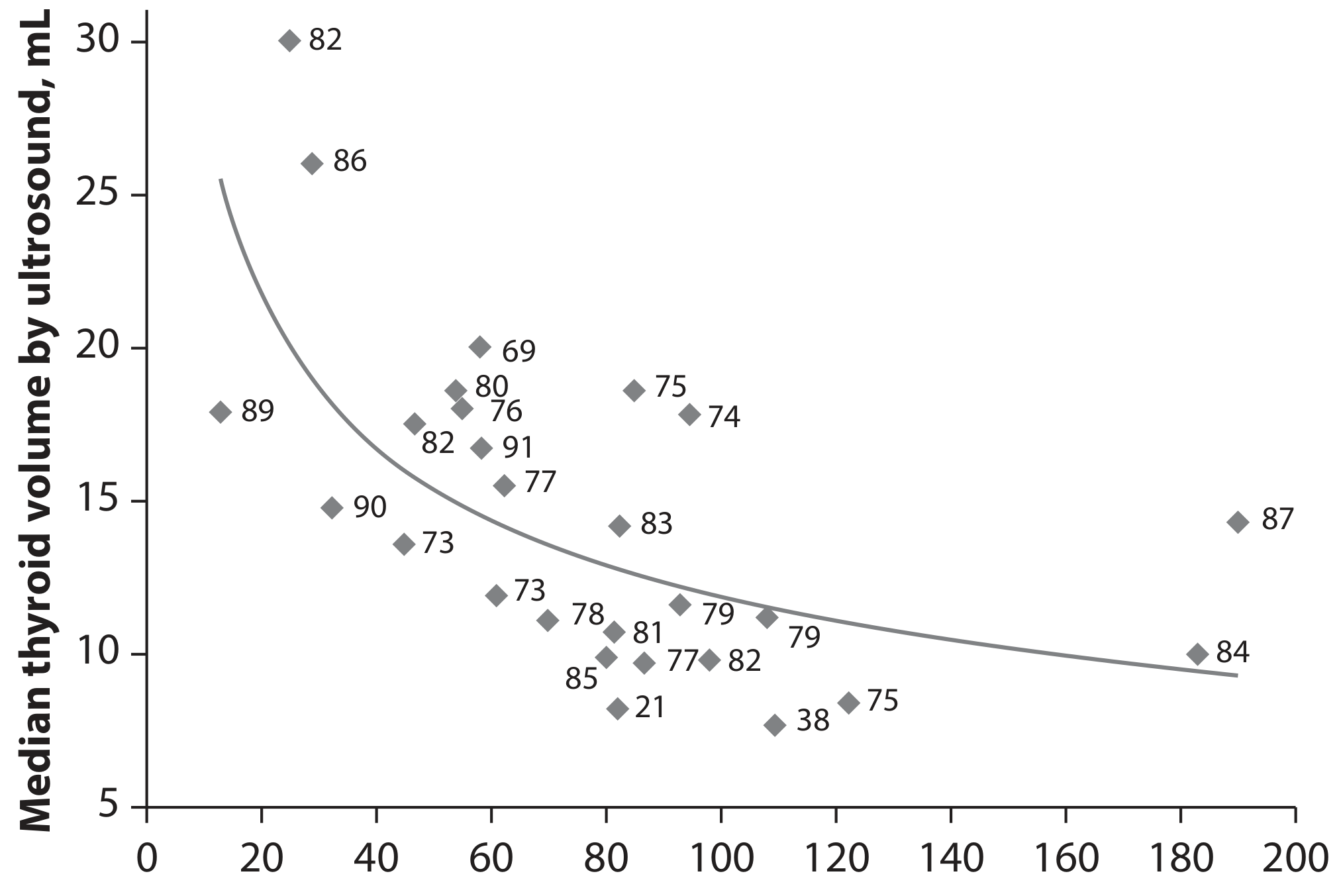
4. Pathophysiology - How Deficiency Causes Goitre
The mechanism follows this sequence:
- Low dietary iodine → ↓ thyroid hormone synthesis
- ↓ T3/T4 → ↓ negative feedback on pituitary
- ↑ TSH secretion (compensatory)
- TSH has a trophic effect on thyroid follicular cells → thyroid enlargement
- If compensation is sufficient → euthyroid goitre
- If compensation fails → goitrous hypothyroidism
This inverse relationship between urinary iodine and thyroid volume is shown below (Scott-Brown's Otorhinolaryngology):
5. Congenital Iodine Deficiency (Cretinism)
Cretinism refers to hypothyroidism developing in infancy/early childhood due to iodine deficiency. Historically common in Himalayas, inland China, Africa, and mountainous regions.
Clinical features (Robbins Pathologic Basis of Disease):
- Severe intellectual disability (mental retardation)
- Short stature
- Coarse facial features
- Protruding tongue
- Umbilical hernia
Pathogenesis of neurological damage:
- Maternal T3 and T4 cross the placenta and are critical for fetal brain development
- If maternal thyroid deficiency occurs before fetal thyroid gland development → severe intellectual disability
- If maternal deficiency occurs after fetal thyroid becomes functional → normal brain development is preserved
Two types of endemic cretinism:
- Neurological cretinism - intellectual disability, deafness, spasticity (predominant where iodine deficiency is severe in early pregnancy)
- Myxoedematous (hypothyroid) cretinism - severe hypothyroidism, dwarfism, puffy features (predominant where deficiency is less severe but persists)
Note: Concomitant selenium deficiency may also contribute to neurological manifestations. Rarely, cretinism results from genetic defects (dyshormonogenetic goitre).
6. Myxoedema (Adult Hypothyroidism from Iodine Deficiency)
In the adult, the condition is insidious and may take years to manifest. Key features include:
- Generalized fatigue, apathy, mental sluggishness (may mimic depression)
- Slowed speech and intellectual function
- Cold intolerance, constipation, decreased sweating
- Cool, pale skin; nonpitting oedema (myxoedema)
- Broadening and coarsening of facial features
- Enlarged tongue, deepening of voice
- ↑ Total cholesterol and LDL (proatherogenic)
- Decreased cardiac output, shortness of breath
- Histology: accumulation of glycosaminoglycans and hyaluronic acid in skin and subcutaneous tissue
Laboratory diagnosis:
- ↑ TSH (most sensitive screening test for primary hypothyroidism)
- ↓ Free T4 (overt hypothyroidism)
- Subclinical hypothyroidism = elevated TSH + normal free T4
7. Assessment of Iodine Deficiency
Epidemiological indicators (Park's):
- Prevalence of goitre
- Prevalence of cretinism
- Urinary iodine concentration (UIC) - best surrogate marker (corrected for creatinine)
- Thyroid function tests (TSH, T3, T4)
UIC cut-offs:
| Status | UIC |
|---|---|
| Sufficient | > 100 μg/L |
| Moderate deficiency | < 50 μg/L |
| Severe deficiency | < 25 μg/L |
Iodine sufficiency in school-age children: median UIC 100-299 μg/L
8. Iodine Deficiency in Pregnancy
Severe iodine deficiency in pregnancy is associated with (Creasy & Resnik's Maternal-Fetal Medicine):
- Increased perinatal and infant mortality
- Pregnancy loss
- Maternal and fetal goitre
- Fetal growth restriction
- Offspring cognitive dysfunction
Even mild iodine deficiency in early gestation is associated with lower verbal IQ, reading accuracy, and reading comprehension in children at age 8. This underscores the multi-generational public health impact.
9. Prevention & Control
Iodized Salt (Primary strategy)
- Most effective and cost-efficient intervention
- Mandatory iodization of salt is the cornerstone of national programmes
- Level: 15-20 ppm potassium iodate added to salt
- Not universally enforced (e.g., UK does not mandate it)
National IDD Control Programme (India)
India's programme started as the Goitre Control Programme in 1962, then expanded to the National IDD Control Programme. Essential components:
- Use of iodized salt in place of common salt
- Monitoring and surveillance
- Manpower training
- Mass communication
- Resurveys every 5 years
India's "Himalayan goitre belt" stretches ~2,400 km from Kashmir to the Naga Hills, affecting numerous northern states. >71 million persons suffer from goitre and IDD in India.
Hazards of Iodization (exam-relevant)
- Mild increase in incidence of thyrotoxicosis following iodization programmes
- Increase in Hashimoto's (lymphocytic) thyroiditis
- Risk of iodism or iodide goitre is very small
10. Quick-Reference Summary Table
| Feature | Detail |
|---|---|
| Daily requirement (adult) | 150 mcg/day |
| Requirement in pregnancy | 250 mcg/day (WHO) |
| Best surrogate marker | Urinary iodine concentration (UIC) |
| Sufficiency threshold (UIC) | >100 μg/L |
| Mechanism of goitre | ↓ T4 → ↑ TSH → thyroid hypertrophy |
| Most sensitive lab test | Serum TSH |
| Best dietary sources | Fish, dairy products |
| Most effective prevention | Iodized salt |
| Neurological damage timing | Maternal deficiency before fetal thyroid develops = severe |
| Selenium co-deficiency | Worsens neurological cretinism |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22E (2025); Park's Textbook of Preventive and Social Medicine; Medical Physiology (Boron & Boulpaep); Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1; Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.