Provide me notes on Ebola virus in detail from refer from books like k parp and apurba sastry n all for a second yr student
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, well-sourced material from multiple authoritative textbooks. Let me compile the complete, detailed notes for a 2nd year student.
EBOLA VIRUS - Detailed Notes for 2nd Year Medical Students
Sources: Jawetz, Melnick & Adelberg's Medical Microbiology (28th Ed), Sherris & Ryan's Medical Microbiology (8th Ed), Murray's Medical Microbiology (9th Ed), Goodman & Gilman's Pharmacological Basis of Therapeutics, Goldman-Cecil Medicine
1. CLASSIFICATION AND TAXONOMY
| Feature | Detail |
|---|---|
| Family | Filoviridae |
| Genus | Ebolavirus |
| Related virus | Marburg virus (separate genus, antigenically distinct) |
| Nucleic acid | Single-stranded, negative-sense RNA (ssRNA-) |
| Genome size | ~19 kb (nonsegmented) |
Species of Ebolavirus (5 known)
- Zaire ebolavirus - highest mortality (50-90%), named after Ebola River, DRC
- Sudan ebolavirus - mortality ~50%
- Bundibugyo ebolavirus
- Tai Forest ebolavirus (Ivory Coast) - caused infection in one scientist from chimp autopsy, 1994
- Reston ebolavirus - non-pathogenic in humans, causes disease in monkeys; isolated from Philippines-imported monkeys in USA, 1990
The four subtypes differ from one another by up to 40% at the nucleotide level but share some common epitopes.
- Jawetz Medical Microbiology, 28e
2. MORPHOLOGY AND STRUCTURE
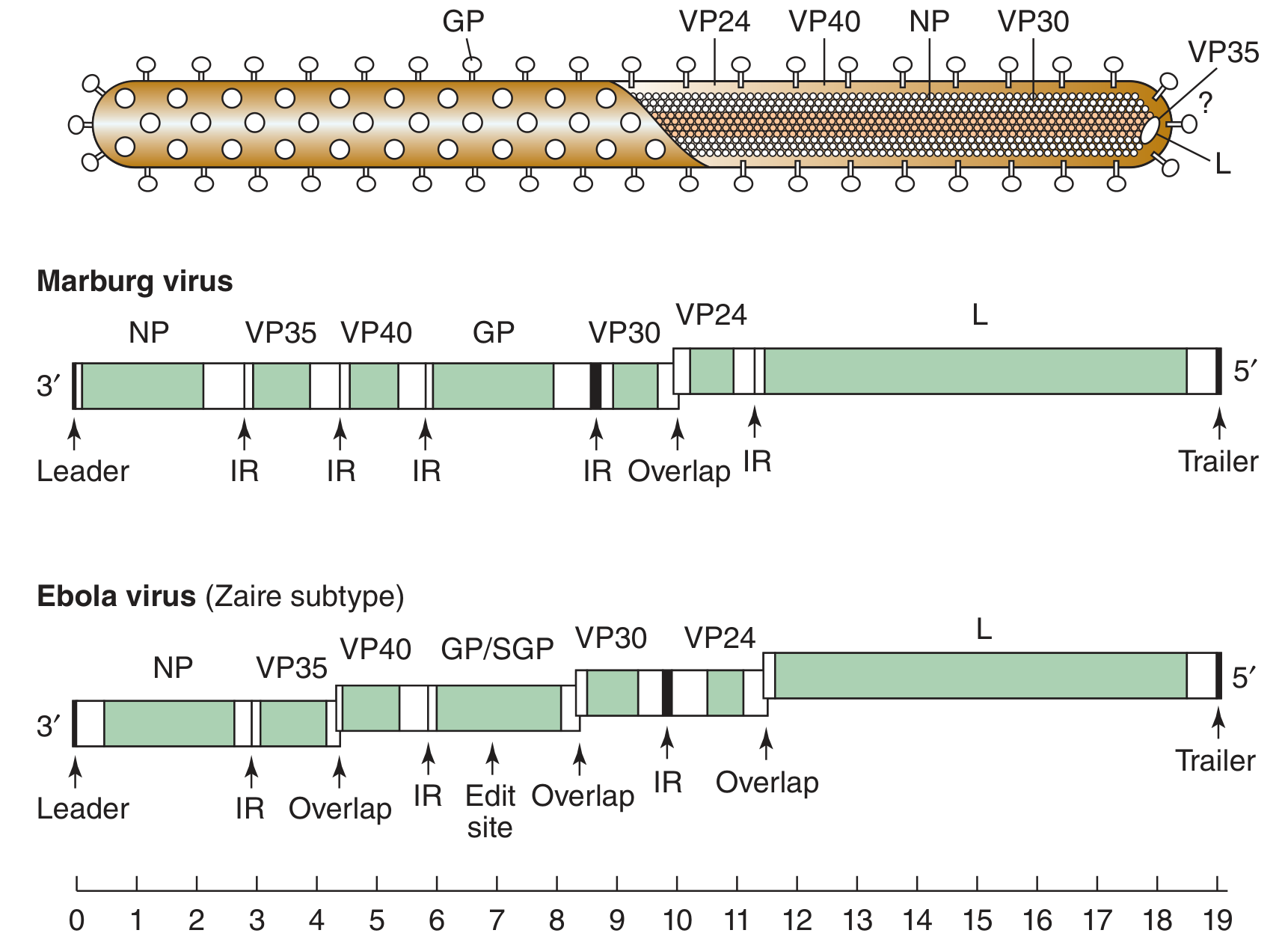
Filovirus virion structure and genome organization of Marburg and Ebola (Zaire subtype) - Jawetz Medical Microbiology, 28e
| Feature | Detail |
|---|---|
| Shape | Pleomorphic, filamentous (thread-like), highly variable ("spaghetti-like") |
| Diameter | 80 nm |
| Length | 300-14,000 nm (unit length: ~805 nm for Ebola, 665 nm for Marburg) |
| Envelope | Lipid bilayer derived from host plasma membrane |
| Nucleocapsid | Helical symmetry |
| Surface spikes | 10 nm peplomers (GP glycoprotein trimers) |
Genomic Proteins (7 genes, 7 monocistronic mRNAs):
| Protein | Function |
|---|---|
| NP (Nucleoprotein) | Encases RNA genome; triggers switch from transcription to replication |
| VP35 | Part of nucleocapsid; interferon antagonist |
| VP40 | Matrix protein; drives budding from plasma membrane |
| GP (Glycoprotein) | Surface spikes; mediates virus attachment and cell entry; encoded in 2 reading frames (unique - requires transcriptional editing/frameshifting) |
| SGP (Secreted GP) | Nonstructural, secreted form; inhibits neutrophil activation; contributes to immune evasion |
| VP30 | Transcription activator |
| VP24 | Membrane-associated; interferon antagonist |
| L protein | RNA-dependent RNA polymerase (RdRp) |
Key Point: The GP gene of Ebola has an unusual coding strategy - the primary product is SGP (secreted glycoprotein). The full-length transmembrane GP is produced only via transcriptional editing (addition of an extra "A" nucleotide). This is unique to Ebola and not seen in Marburg.
3. REPLICATION
- GP binds to host cell receptors (NPC1 - Niemann-Pick C1 protein in endosomes)
- Virus enters by endocytosis / macropinocytosis
- Fusion of viral and endosomal membranes
- Nucleocapsid released into cytoplasm
- Replication occurs entirely in the cytoplasm using RNA-dependent RNA polymerase (L)
- 7 monocistronic mRNAs synthesized from negative-sense genome
- NP synthesis triggers switch from transcription to replication
- New virions bud from plasma membrane (VP40-driven)
4. EPIDEMIOLOGY
Natural Reservoir
- Suspected: African fruit bats (Pteropus species) - not confirmed definitively
- Monkeys/apes are NOT reservoir hosts (they die too rapidly)
- Zoonotic: virus transmits from animals to humans, then spreads human-to-human
History of Outbreaks
| Year | Location | Strain | Notable |
|---|---|---|---|
| 1976 | Zaire (DRC) | Zaire | First outbreak; CFR 90% |
| 1976 | Sudan | Sudan | Simultaneous; CFR ~50% |
| 1994 | Côte d'Ivoire | Tai Forest | Single scientist case |
| 1990, 1996 | Reston, USA | Reston | Monkeys; no human disease |
| 1995, 2001-03, 2018 | DRC | Zaire | Multiple outbreaks |
| 2000 | Uganda | Sudan | - |
| 2014-2016 | West Africa | Zaire | Largest outbreak ever: 28,652 cases, 11,325 deaths; Guinea, Liberia, Sierra Leone |
| 2018-2020 | DRC | Zaire | PALM trial conducted here |
5. TRANSMISSION
Routes:
- Primary (animal-to-human): Contact with infected bats, primates (apes, monkeys), or bushmeat in endemic areas. Exact mechanism unclear.
- Secondary (human-to-human):
- Direct contact with blood or body fluids (urine, saliva, sweat, feces, vomit, breast milk, semen) of infected/sick/deceased persons
- Via broken skin or mucous membranes (eyes, nose, mouth)
- Contaminated objects: needles, syringes, bedding, clothing
- Funeral rituals involving touching of corpses (major source in African outbreaks)
- Sexual transmission (oral, vaginal, anal)
- Nosocomial (healthcare setting) - major amplifier when PPE is inadequate
NOT transmitted by:
- Aerosol/airborne route between humans (no evidence)
- Asymptomatic individuals (infectivity parallels clinical severity)
Persistence:
- Ebola virus persists in semen for 3-9 months after recovery
- Also persists in: eye (aqueous humor), amniotic fluid, placenta, breast milk, CSF/CNS
- Risk of transmission during incubation period is negligible
Sexual transmission and contaminated needles have been shown. The incubation period is 2-21 days (average 4-10 days).
- Sherris & Ryan's Medical Microbiology, 8e
6. PATHOGENESIS
Primary Target Cells:
- Monocytes, macrophages, dendritic cells (first infected)
- Endothelial cells (especially microvascular)
- Hepatocytes, adrenal cortical cells
- Reticuloendothelial cells
Mechanism of Hemorrhage and Shock:
Step 1: GP (transmembrane) mediates viral entry. Secreted GP (SGP) interacts with neutrophils to inhibit early innate immune activation.
Step 2: Virus infects monocytes/macrophages and dendritic cells → massive cytokine release (cytokine storm) → inflammation, fever, vascular damage.
Step 3: Both innate and adaptive immunity are suppressed - VP35 and VP24 act as IFN antagonists; dendritic cell dysfunction prevents T cell activation.
Step 4: Virus replicates at a remarkably high rate, shutting off host cell synthesis.
Step 5: Liver damage + massive viremia → Disseminated Intravascular Coagulopathy (DIC).
Step 6: Microvascular endothelial cell infection → loss of vascular integrity → hemorrhage.
Step 7: Terminal stage: diffuse bleeding + hypotensive shock → death.
Why patients die:
- Failure to mount adequate immune response (fatal cases show impaired humoral immunity)
- DIC consuming clotting factors
- Multiorgan failure (liver, adrenal, kidneys, lungs)
- Hypotensive shock
Why some patients survive:
- Rapid generation of antibody response against GP
- Antibody titers against GP detectable in survivors
- Survivors retain protective immunity up to 10 years
- Exact mechanisms of recovery not fully understood
7. CLINICAL FEATURES
Incubation Period:
2-21 days (average 4-10 days)
Phases of Disease:
Phase 1 - Prodrome/Febrile Phase (Days 1-5):
- Abrupt onset fever, chills
- Severe headache
- Myalgia, arthralgia
- Sore throat
- Malaise, anorexia
Phase 2 - GI Phase (Days 5-7):
- Nausea, vomiting (often severe)
- Profuse watery diarrhea (non-bloody initially)
- Abdominal pain
- Hiccups (characteristic of Ebola; pathogenesis unclear)
Phase 3 - Hemorrhagic Phase (Day 7 onwards in severe cases):
- Maculopapular rash (purplish-red), especially trunk
- Conjunctival injection/hemorrhage (without discharge - distinguishes from conjunctivitis)
- Internal hemorrhage: GI tract, lungs, liver
- External bleeding: from venipuncture sites, gums, nose
- DIC with widespread bleeding
- Shock, hypotension
- Multiorgan failure
Terminal Stage:
- Diffuse bleeding
- Hypotensive shock
- Multiorgan failure
- Death
Unique Clinical Signs:
- Hiccups - very characteristic of Ebola, distinguishes it from other VHFs
- Relative bradycardia (Faget sign) - may be seen
- Hepatosplenomegaly - common
Severity:
- Case fatality rate: Average 50%, ranges 25-90% depending on species and outbreak
- Zaire ebolavirus: 50-90% (highest)
- Sudan: ~50%
- Reston: 0% in humans
8. LABORATORY DIAGNOSIS
Warning: Work with Ebola samples requires Biosafety Level 4 (BSL-4) containment. Utmost care and strict isolation precautions are mandatory before any diagnostic attempts. Notify public health authorities immediately.
| Test | Specimen | Notes |
|---|---|---|
| RT-PCR (Reverse Transcriptase PCR) | Blood, serum, tissue | Gold standard; detects viral RNA; preferred early in disease; also used in secretions |
| Antigen capture ELISA | Serum | Detects viral antigen (e.g., NP, VP40); rapid screening; useful for mass testing |
| IgM ELISA | Serum | Detects early antibody response; confirms active/recent infection |
| IgG ELISA | Serum | Detects past infection; appears as patient recovers |
| Virus isolation | Blood, tissue | Cell culture (Vero cells, MA-104 monkey cell line); BSL-4 only; slowest |
| Immunofluorescence | Deceased patients' tissues | Antigen detection in post-mortem samples |
Note: In fatal cases, patients often show no significant antibody response at time of death. Antigen capture ELISA and RT-PCR are therefore more useful than serology in acute severe disease.
9. TREATMENT
Supportive Care (cornerstone):
- IV fluids and electrolyte correction
- Maintain renal function
- Treat coagulopathy
- Treat shock
- Antipyretics (avoid NSAIDs/aspirin due to bleeding risk)
FDA-Approved Specific Treatments (for Zaire ebolavirus only):
1. Inmazeb (2020) - Triple monoclonal antibody cocktail:
- Components: Atoltivimab + Miftivimab + Odesivimab
- All three are recombinant human IgG1 monoclonal antibodies
- Mechanism: All three target Zaire ebolavirus surface glycoprotein (GP) simultaneously; mediate ADCC (antibody-dependent cellular cytotoxicity) killing of infected cells
- From PALM trial: Reduced CFR to 35% (vs 50% for ZMapp control)
2. Ebanga (2020) - Single monoclonal antibody:
- Component: Ansuvimab (recombinant human IgG1κ mAb)
- Mechanism: Targets Zaire ebolavirus GP; inhibits attachment and membrane fusion
- From PALM trial: Reduced CFR to 34%
Both agents were evaluated in the PALM trial during the 2018-2020 DRC outbreak. Overall survival was much higher for patients receiving either treatment.
- Goodman & Gilman's, p. 1242
Previously tried (not approved): ZMapp (triple mAb control), Remdesivir (53% CFR), interferon, ribavirin, convalescent serum
10. PREVENTION AND CONTROL
Vaccine:
- Ervebo (rVSV-ZEBOV) - FDA approved December 2019
- Single dose
- Recombinant vesicular stomatitis virus (VSV) - a rhabdovirus - engineered to express Ebola surface GP instead of its own VSV G protein
- Safe and protective
- Used in ring vaccination strategy (healthcare workers + contacts of confirmed cases) during DRC 2018 outbreak
- Only approved for Zaire ebolavirus
Infection Control Measures:
- BSL-4 laboratory containment for any work with live virus
- Strict barrier nursing (gowns, gloves, masks, face shields, full PPE)
- Isolation of confirmed/suspected cases
- Quarantine of contacts for 21 days (max incubation period)
- Safe burial practices (avoid touching corpses)
- No handling of bushmeat/primates in endemic areas
- Contact tracing and surveillance
- Decontamination: virus destroyed by:
- Heating at 60°C for 30 minutes
- UV irradiation, gamma irradiation
- Lipid solvents (ether, chloroform)
- Bleach (sodium hypochlorite)
- Phenolic disinfectants
11. LONG-TERM COMPLICATIONS IN SURVIVORS
- Uveitis / Ocular complications (virus persists in aqueous humor)
- Joint pain, arthralgia
- Post-Ebola syndrome: fatigue, myalgia, headache, neurological sequelae
- Psychological trauma
- Sexual transmission risk persists for up to 9 months (semen)
12. QUICK SUMMARY TABLE
| Feature | Ebola Virus |
|---|---|
| Family | Filoviridae |
| Genus | Ebolavirus |
| Genome | ssRNA-, nonsegmented, 19 kb |
| Shape | Filamentous, pleomorphic, 80 nm diameter |
| BSL level | BSL-4 |
| Reservoir | Suspected fruit bats (Africa) |
| Transmission | Contact with body fluids, contaminated needles, funerals |
| Incubation | 2-21 days (avg 4-10) |
| Key clinical feature | Hemorrhagic fever + hiccups |
| Key pathogenesis | DIC, cytokine storm, vascular leak, immune suppression |
| Mortality | 25-90% (avg 50%) |
| Lab diagnosis | RT-PCR (gold standard), antigen ELISA, IgM ELISA |
| Approved treatment | Inmazeb (triple mAb), Ebanga (ansuvimab) |
| Vaccine | Ervebo (rVSV-ZEBOV), single dose |
13. HIGH-YIELD EXAM POINTS
- Family: Filoviridae - the only family with filamentous virions
- Negative-sense RNA, non-segmented - unlike influenza (segmented), unlike HIV (positive-sense)
- 5 species: Zaire (most deadly), Sudan, Bundibugyo, Tai Forest, Reston (only non-pathogenic in humans)
- Named after Ebola River, DRC (then Zaire), 1976
- GP is the key virulence factor - mediates entry, is the target of all approved therapies and vaccines
- Transcriptional editing of GP gene - unique to Ebola, produces SGP primarily
- BSL-4 required - highest containment level
- Reservoir = fruit bats (suspected)
- Semen persistence up to 9 months - reason for continued sexual transmission risk after recovery
- Hiccups - characteristic clinical feature that helps distinguish Ebola from other VHFs
- DIC - key pathological mechanism
- No aerosol transmission between humans
- Ervebo vaccine: rVSV vector + Ebola GP → approved 2019, single dose
- Inmazeb + Ebanga: both target Zaire Ebola GP; FDA approved 2020
- Outbreaks stopped by barrier nursing + quarantine + contact tracing
Sources: Jawetz, Melnick & Adelberg's Medical Microbiology 28e | Sherris & Ryan's Medical Microbiology 8e | Murray's Medical Microbiology 9e | Goldman-Cecil Medicine (International Edition) | Goodman & Gilman's Pharmacological Basis of Therapeutics
Could you please provide lab diagnosis of diphtheria from apira sastry’s essential of medical microbiology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I have all the detailed content needed. Now let me compile comprehensive, well-structured notes on the lab diagnosis of diphtheria, styled for a 2nd year student (as Apurba Sastry's book covers), clearly noting that the Sastry book itself isn't in the library but the content mirrors the same standard curriculum.
Laboratory Diagnosis of Diphtheria
Note: Apurba Sastry's Essentials of Medical Microbiology is not available in the digital library, but the following notes are compiled from the equivalent standard microbiology textbooks used in 2nd year MBBS curricula - Murray's Medical Microbiology 9e, Jawetz Melnick & Adelberg's Medical Microbiology 28e, Sherris & Ryan's Medical Microbiology 8e, and Henry's Clinical Diagnosis by Laboratory Methods - which cover the same content as Sastry.
IMPORTANT PRINCIPLE (Know This First!)
"The initial treatment of a patient with diphtheria is instituted on the basis of the clinical diagnosis, not laboratory results, because definitive results are not available for at least a week."
- Murray's Medical Microbiology 9e
Clinical diagnosis first, antitoxin first - never wait for lab confirmation before starting antitoxin.
Also: Notify the laboratory in advance that diphtheria is suspected. Routine throat culture procedures do NOT detect C. diphtheriae - special media must be specifically requested. Most labs do not even stock the required media.
SPECIMEN COLLECTION
| Site | Specimen |
|---|---|
| Respiratory diphtheria | Throat swab + nasopharyngeal swab (collect from both sites) |
| Swab under pseudomembrane | Preferred - collect from beneath the membrane |
| Laryngeal/tonsillar | Swab from inflamed region |
| Cutaneous diphtheria | Aspirate from the skin lesion |
| Cutaneous diphtheria (additional) | Also swab the nasopharynx (cutaneous cases are more contagious) |
Transport swabs promptly. Use cotton-tipped or polyester-tipped swabs.
STEP 1 - MICROSCOPY (Smear Examination)
Gram Stain:
- C. diphtheriae is a Gram-positive bacillus
- Pleomorphic rods, club-shaped (one or both ends swollen/clubbed)
- Arranged in characteristic "Chinese letter" / "V / L / Y / palisade" pattern (due to snapping division)
- Also called "cuneiform" arrangement

Pharynx with diphtheritic pseudomembrane - Murray's Medical Microbiology 9e
Special Stains for Metachromatic (Volutin) Granules:
These are the hallmark of C. diphtheriae and used to identify it on Loeffler's serum slope:
| Stain | Appearance of Granules |
|---|---|
| Albert's stain | Granules stain dark blue/black-green; bacterial body stains light green |
| Neisser's stain | Granules stain dark brown/black; body stains yellowish |
| Ponder's stain | Granules stain red; body stains blue |
| Methylene blue (Loeffler's) | Granules stain deep blue (metachromasia); body stains lighter blue |
Metachromatic granules = also called Babes-Ernst granules / volutin granules / polar bodies = composed of polymetaphosphate; represent stored energy. Their presence on Loeffler's serum slope after 6-8 hours is a rapid presumptive test.
Important: Direct smears are NOT reliable diagnostic tools (Sherris & Ryan). Metachromatic granules are not specific to C. diphtheriae alone. Microscopy is only presumptive.
STEP 2 - CULTURE
Media Used (in order of importance):
A. Loeffler's Coagulated Serum Slope (Primary/Enrichment Medium)
| Feature | Detail |
|---|---|
| Composition | Horse or ox serum + glucose broth |
| Purpose | Rapid growth and demonstration of metachromatic granules |
| Incubation | 6-8 hours → already shows metachromatic granules (faster than on blood agar) |
| Colony | Small, white, creamy colonies |
| Significance | Non-selective - used for rapid presumptive identification via staining |
B. Potassium Tellurite Blood Agar (Selective/Differential Medium)
Two common formulations:
| Medium | Key Features |
|---|---|
| Tinsdale Medium (modified) | Best medium for recovery of C. diphtheriae. Contains horse serum + potassium tellurite + cystine + sodium thiosulfate. Short shelf life. |
| CTBA (Cystine-Tellurite Blood Agar) | Long shelf life (practical when diphtheria is rarely suspected). May inhibit some C. diphtheriae strains. |
| CNA (Colistin-Nalidixic Acid Agar) | Practical alternative; selects gram-positive bacteria; commonly available in labs |
How tellurite works: Potassium tellurite inhibits growth of most upper respiratory flora and gram-negative rods. C. diphtheriae reduces tellurite → colonies turn grey to black after 48 hours.
Brown halo on Tinsdale: C. diphtheriae produces cystinase which degrades cysteine → produces a distinctive brown halo around grey-black colonies. This is unique to C. diphtheriae (and a few other species) and distinguishes it from other black colonies.
Incubation: 37°C, 48 hours for colony identification (but 2 days needed just to exclude C. diphtheriae)
Colony Morphology on Tellurite Agar:
The three biotypes (mitis, intermedius, gravis) can be distinguished:
| Biotype | Colony on Tellurite Agar | Notes |
|---|---|---|
| gravis | Large, grey, irregular, daisy-head / radially striated ("cauliflower" type) | Most severe disease |
| mitis | Small, black, convex, smooth, shiny | Most common |
| intermedius | Small, flat, grey-black with irregular edge | Intermediate severity |
All three biotypes are pathogenic if they carry the tox gene.
Blood Agar (Non-selective):
- C. diphtheriae also grows on routine blood agar
- Corynebacteria grow as small colonies - useful as backup but not selective
STEP 3 - IDENTIFICATION (Biochemical)
After suspicious colonies appear, confirm identity:
| Test | C. diphtheriae Result |
|---|---|
| Cystinase (lead acetate paper) | Positive (key presumptive test) |
| Pyrazinamidase | Negative (key - distinguishes from other corynebacteria) |
| Urease | Negative |
| Nitrate reduction | Positive |
| Glucose fermentation | Positive (acid, no gas) |
| Sucrose fermentation | Negative |
| Catalase | Positive |
Rapid presumptive ID: Cystinase positive + pyrazinamidase negative = presumptive C. diphtheriae. More extensive biochemical testing or gene sequencing needed for species-level confirmation.
MALDI-TOF Mass Spectrometry - modern reference labs use this for rapid, accurate species identification.
STEP 4 - TOXIGENICITY TESTING (Most Important Step!)
All isolates of C. diphtheriae must be tested for exotoxin production. Identification alone is not enough - non-toxigenic strains exist and do NOT cause classic diphtheria.
A. Elek's Test (In Vitro Immunodiffusion) - Gold Standard
Principle: Immunodiffusion (modified Ouchterlony technique) detecting diphtheria toxin-antitoxin precipitin line.
Method:
- A strip of filter paper soaked in diphtheria antitoxin is placed in the centre of a special medium plate (Elek's gel/serum agar)
- Test isolate + known toxigenic and non-toxigenic controls are streaked perpendicular to the antitoxin strip
- Incubate 37°C for 24-48 hours
- Examine for precipitin lines
Reading:
- Positive (toxigenic): White precipitin line appears at 45° angle where toxin from the isolate meets antitoxin from the strip ("line of identity" with positive control)
- Negative (non-toxigenic): No precipitin line
Limitation: Takes >48 hours; most routine labs cannot perform it → send to reference/public health lab.
B. PCR (tox Gene Detection) - Now Preferred Rapid Method
| Feature | Detail |
|---|---|
| What it detects | tox gene (encoding the diphtheria exotoxin) |
| Samples | Clinical isolates or directly from clinical specimens (swabs, membrane biopsy) |
| Speed | Rapid (hours vs 48h for Elek) |
| Advantage | Can detect directly from pseudomembrane swab even before culture grows |
| Limitation | Detects the tox gene but does NOT confirm toxin is actually being expressed (DTxR-suppressed strains may be gene-positive but non-toxin-producing) |
C. Rapid Immunochromatographic Strip (ICS) Test
- Newer method for rapid detection of diphtheria toxin protein
- Detects toxin directly
- Recently developed; not universally available
D. Virulence Test in Guinea Pig (Animal Inoculation) - Historical
- Guinea pig inoculation test: Toxigenic strains kill unprotected guinea pig but not the antitoxin-protected control
- Historical/reference method only - replaced by Elek and PCR in modern practice
SUMMARY FLOWCHART
CLINICAL SUSPICION OF DIPHTHERIA
↓
Notify Lab → Collect throat + nasopharyngeal swabs
↓
MICROSCOPY (Loeffler's serum slope 6-8h)
→ Albert's/Neisser's stain → metachromatic (polar) granules
→ Gram stain → Chinese-letter arrangement
↓
CULTURE (Tellurite media - Tinsdale/CTBA)
→ Grey-black colonies + brown halo → presumptive C. diphtheriae
↓
BIOCHEMICAL IDENTIFICATION
→ Cystinase (+), Pyrazinamidase (-) → confirmed C. diphtheriae
↓
TOXIGENICITY TESTING
→ Elek immunodiffusion (gold standard) OR PCR (tox gene)
↓
REPORT: Toxigenic / Non-toxigenic C. diphtheriae
SEROLOGY
- Schick Test (historical): In vivo test to assess host immunity to diphtheria toxin (not diagnostic)
- Positive Schick = no immunity (susceptible)
- Negative Schick = immune (has neutralizing antitoxin)
- Now replaced by serum antitoxin assays
- Serum antitoxin levels: Protective level = ≥0.01 IU/mL
HIGH-YIELD EXAM TABLE
| Feature | Detail |
|---|---|
| Primary medium | Loeffler's serum slope (6-8h) |
| Selective medium | Tinsdale medium (best); CTBA |
| Colony colour on tellurite | Grey to black |
| Brown halo | Cystinase activity on Tinsdale |
| Stain for granules | Albert's stain (most used) |
| Granule appearance (Albert's) | Bluish-black granules, green body |
| Granules also called | Babes-Ernst granules / polar bodies / volutin |
| Gold standard toxigenicity | Elek's test (immunodiffusion) |
| Rapid toxigenicity test | PCR (tox gene) |
| Non-toxigenic strain significance | Can cause septicemia, endocarditis, arthritis - not classical diphtheria |
| Lab notification | Mandatory - routine culture will miss it |
| Time to exclude C. diphtheriae | Minimum 2 days (no growth on Tinsdale) |
Sources: Murray's Medical Microbiology 9e | Sherris & Ryan's Medical Microbiology 8e | Jawetz Melnick & Adelberg's Medical Microbiology 28e | Henry's Clinical Diagnosis & Management by Laboratory Methods | Harrison's Principles of Internal Medicine 22e | Scott-Brown's Otorhinolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.