
An 8-year-old boy reported with a chief complaint of crooked front teeth the pediatric dental clinic for routine control. On Intraoral examination the maxillary left central incisor wasfound to be in crossbite. Following is the intra-oral picture.With the above clinical condition, address the following: B 4.1 Discuss the difference between skeletal and dental anterior cross bite. (2 marks) B 4.2 Describe the design of any appliance of choice for correction of the above malocclusion. (3 marks) B 4.3 Discuss the treatment plan for anterior and posterior cross bite had this patient reported in permanent dentition stage. (5 mark
skeletal vs dental anterior crossbite diagnosis classification
anterior crossbite correction appliance design removable fixed orthodontics
Anterior Crossbite in an 8-Year-Old: Clinical Structured Answer
B 4.1 — Skeletal vs. Dental Anterior Crossbite (2 marks)
| Feature | Dental Anterior Crossbite | Skeletal Anterior Crossbite |
|---|---|---|
| Definition | One or more maxillary incisors occlude lingual to mandibular incisors due to a tooth position anomaly | Maxillary incisors occlude lingual to mandibular incisors due to an underlying jaw discrepancy (maxillary deficiency and/or mandibular prognathism) |
| Cause | Aberrant eruption path, tooth size/arch length discrepancy, retained deciduous tooth, trauma | Maxillary hypoplasia (Class III skeletal base), mandibular prognathism, or both |
| Skeletal pattern | Class I skeletal base (ANB angle normal: ~2°) | Class III skeletal base (ANB angle reduced or negative) |
| Jaw relationship | Normal; no jaw discrepancy | Retrognathic maxilla (SNA reduced) and/or prognathic mandible (SNB increased) |
| Facial profile | Straight or slightly convex | Concave ("dish-face" appearance) |
| Chin-point deviation | Absent | May show chin prominence |
| Number of teeth involved | Usually 1–2 teeth | Multiple anterior teeth involved |
| Mandibular shift | May show functional shift (anterior displacement of mandible on closure) — common | Less functional shift; true skeletal discrepancy |
| Freeway space / AFMH | Normal | May be reduced |
| Cephalometric findings | Normal ANB, normal jaw lengths | Reduced SNA, reduced ANB, elongated mandibular body |
| Treatment | Orthodontic tipping/movement of teeth (simpler) | Orthopedic (facemask/reverse headgear) in growing patients; orthognathic surgery in adults |
B 4.2 — Appliance Design for Correction (3 marks)
Option A: Upper Removable Appliance with Z-spring
-
Baseplate
- Acrylic plate covering the palate
- Extends from behind the upper incisors to the posterior teeth
- Must have adequate retention and not impinge on soft tissues
-
Retention (clasps)
- Adams clasps (arrowhead clasps) on the upper first permanent molars (if erupted) or upper first deciduous molars — provides primary retention
- May supplement with ball-end clasps or C-clasps on deciduous canines
-
Active component — Z-spring (Double cantilever/coffin spring)
- Made from 0.5 mm hard stainless steel wire
- Located in the acrylic labial to the palatally displaced maxillary left central incisor
- The Z-configuration provides a labially directed force to tip the incisor forward (procline it)
- Activated by opening the Z-loops by approximately 0.5–1 mm at each visit (every 3–4 weeks)
- Springs must be covered by acrylic posteriorly to prevent impingement and allow force delivery
-
Posterior bite plane (bite raising)
- Flat posterior acrylic bite plane — raises the occlusion by 1–2 mm (approximately the freeway space minus 1 mm)
- Essential: disengages the occlusion so the palatally displaced incisor has room to move labially without being blocked by the mandibular incisors
- Without this, the mandibular incisor acts as a physical block
-
Labial bow (optional)
- 0.7 mm stainless steel wire
- Helps retain the appliance and controls any upper incisor flaring
Option B: Fixed inclined plane (Catalan's appliance)
- A simple acrylic inclined plane cemented to the lower incisors
- The inclined surface guides the upper incisor labially on every bite
- Suitable when cooperation is a concern (no patient activation required)
- Limitation: can only be used if there is sufficient freeway space and the incisor has adequate room to tip
B 4.3 — Treatment Plan for Anterior and Posterior Crossbite in Permanent Dentition (5 marks)
A. Anterior Crossbite in Permanent Dentition
- Cephalometric analysis — determine if skeletal (Class III) or purely dental
- CBCT/study models — assess root positions, bone levels, arch lengths
- Check for functional shift — ask patient to close in centric relation vs. habitual occlusion
(i) Dental Anterior Crossbite
- Fixed orthodontic appliance (full fixed therapy) is the treatment of choice
- Upper fixed appliance with appropriate bracket prescription to procline the palatally placed incisors
- Use of reverse curve of Spee / torque auxiliaries to achieve labial root torque and tip the crown labially
- Lower anterior bite plate or glass ionomer build-up on posterior teeth temporarily to disengage the occlusion if needed
- May use Class III elastics (worn from upper anterior to lower posterior) to bring the upper incisors forward
- Duration: 12–24 months typically; retain with Hawley or vacuum-formed retainer post-treatment
(ii) Skeletal Anterior Crossbite (Class III)
- Camouflage orthodontic treatment with fixed appliances
- Procline upper incisors (dental compensation) + retrocline lower incisors to achieve an edge-to-edge or positive overjet
- Suitable when ANB is not severely negative (typically > −2°) and facial aesthetics are acceptable
- Limitations: creates dental compensation that may compromise periodontium if carried too far
- Combined orthodontic-orthognathic surgical approach
- Pre-surgical orthodontic phase: Decompensate teeth (reverse camouflage) — upper incisors retroclined to upright, lower incisors proclined; align and level arches; coordinate arches
- Surgical phase: Le Fort I osteotomy (maxillary advancement) ± bilateral sagittal split osteotomy (BSSO) for mandibular setback depending on the discrepancy
- Post-surgical orthodontic phase: final detailing of occlusion, settling, root parallelism
- Retention: long-term fixed/removable retention post-surgery
B. Posterior Crossbite in Permanent Dentition
- Determine unilateral vs. bilateral crossbite
- Identify if functional shift is present (mandibular lateral displacement on closure)
- Cephalometric + CBCT to assess whether transverse discrepancy is dental, skeletal (true maxillary constriction), or both
- Measure inter-molar/inter-canine widths (upper and lower)
(i) Dental/Functional Posterior Crossbite
- Fixed orthodontic expansion using:
- Transpalatal arch (TPA) with lateral expansion activation
- Quad helix appliance (four-helix palatal spring cemented to upper molars) — provides slow continuous expansion; suitable for mild dental crossbites
- Slow maxillary expansion (SME) with a removable expansion plate
- Correct any functional shift by eliminating premature contacts (selective occlusal adjustment if minor)
(ii) Skeletal Posterior Crossbite (True Maxillary Transverse Deficiency)
-
Rapid Maxillary Expansion (RME) is the gold standard in adolescents (midpalatal suture still partially patent):
- Hyrax expander or Haas expander cemented to upper first premolars and first molars
- Activation: 2 turns/day (~0.5 mm/day) for 2–3 weeks until overcorrection is achieved
- Retention in situ for 3–6 months for bone consolidation
- Success rate is reduced after 16–18 years when the suture begins to interdigitate
-
Surgically Assisted Rapid Palatal Expansion (SARPE) — indicated when:
- Patient is skeletally mature (fused or nearly fused midpalatal suture)
- Skeletal crossbite is significant (>5 mm transverse discrepancy)
- Procedure: Le Fort I down-fracture or paramedian osteotomies release the suture; RME appliance then expands the maxilla post-surgically
- Followed by standard fixed orthodontics to align teeth and coordinate arches
-
Combined orthognathic surgery (Le Fort I with transverse expansion) — for cases requiring simultaneous AP correction (Class III + transverse deficiency) in fully grown patients
Summary Table — Permanent Dentition Crossbite Treatment
| Type | Severity | Treatment |
|---|---|---|
| Anterior crossbite | Dental | Fixed orthodontics ± lower bite plate, Class III elastics |
| Anterior crossbite | Skeletal mild | Orthodontic camouflage (fixed appliances) |
| Anterior crossbite | Skeletal severe | Pre-surgical ortho → Orthognathic surgery (Le Fort I ± BSSO) → Post-surgical ortho |
| Posterior crossbite | Dental/functional | Quad helix / TPA / slow expansion + occlusal adjustment |
| Posterior crossbite | Skeletal (adolescent) | RME (Hyrax/Haas) + fixed orthodontics |
| Posterior crossbite | Skeletal (adult) | SARPE + fixed orthodontics |
diagrams
anterior crossbite dental skeletal classification cephalometric
removable orthodontic appliance Z-spring design anterior crossbite correction
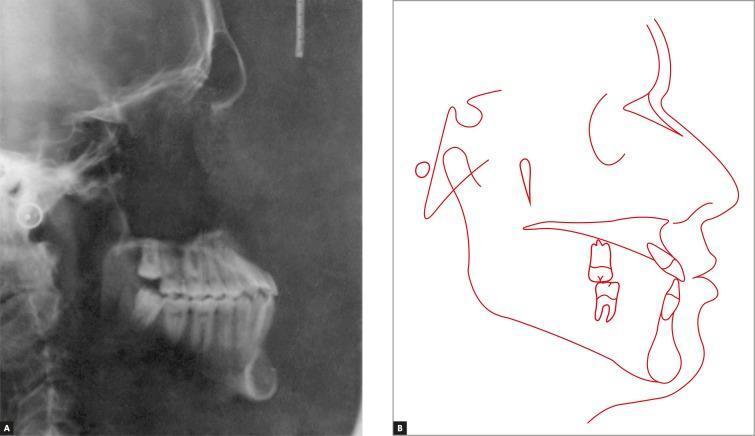
1. Skeletal Class III Anterior Crossbite — Lateral Cephalometric Radiograph & Tracing
2. Removable Upper Appliance with Z-springs — Appliance Design

- Pink acrylic baseplate covering the palate
- Two Z-springs (0.5 mm SS wire) positioned labial to the palatally displaced upper central incisors — these apply a controlled labial tipping force
- Four Adams clasps (thicker SS wire) on primary and permanent first molars bilaterally for firm retention
- A posterior bite plane would be incorporated into the acrylic to disengage the occlusion and allow free labial movement of the crossed incisors