Direct vertebral rotation in Orthopaedics 10marks pg answer with flow chart and images
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Searching the Web
direct vertebral rotation DVR technique scoliosis Lee Suk pedicle screw derotation 3D correction
I now have all the information needed for a comprehensive 10-mark answer. Let me compile the full response with flowchart and images.
Direct Vertebral Rotation (DVR) in Orthopaedics
Source: Campbell's Operative Orthopaedics, 15th Ed 2026 | Lee SM, Suk SI, Chung ER. Spine 2004;29:343
Definition
Direct Vertebral Rotation (DVR) is a three-dimensional deformity correction technique in scoliosis surgery, introduced by Lee, Suk, and Chung (2004), which directly derotates each vertebra in the transverse plane using bilateral pedicle screws and dedicated derotator instruments - rather than relying on indirect derotation through rod rotation alone.
Background / Historical Context
Traditional scoliosis correction with Harrington rods corrected only the coronal (frontal) plane. The Cotrel-Dubousset (CD) technique introduced the concept of rod derotation (rod rotation maneuver, RRM) to achieve 3D correction. However, rod rotation offers limited and inconsistent rotational correction - the actual vertebral derotation depends on friction between pedicle screws and the rod.
DVR was developed to overcome this limitation by applying direct forces to individual vertebral bodies through pedicle screw handles (derotators), enabling true transverse plane correction.
Indication
- Adolescent Idiopathic Scoliosis (AIS) - primary indication
- All curve types where transverse plane (axial rotation) correction is desired
- Especially useful in rigid or severe curves where rod rotation alone fails
- Thoracic curves with prominent rib hump (cosmetic deformity driven by vertebral rotation)
Prerequisites
- Bilateral pedicle screws at every level to be fused in the thoracic spine (all-pedicle-screw construct)
- Neuromonitoring: baseline motor-evoked potentials (MEPs) before any maneuver
- Mean arterial pressure (MAP) ≥ 70 mmHg during correction (to maintain spinal cord perfusion)
- Screw derotators (SUK tubes / derotation handles) attached to pedicle screw heads
Technique (Campbell's TECHNIQUE 40.14)
Step-by-Step
-
Insert bilateral pedicle screws at every thoracic level to be fused.
-
Establish baseline MEPs and maintain MAP ≥ 70 mmHg throughout.
-
Identify the neutral vertebra - the least rotated vertebra distally. Begin derotation proximal to this level.
-
Attach screw derotators (derotation handles/SUK tubes) onto the pedicle screws of the juxta-apical vertebrae on both concave and convex sides.
-
Derotate the vertebrae: For a right thoracic curve, rotate the apical and juxta-apical vertebrae clockwise in the transverse plane (opposite to the direction of vertebral rotation in the thoracic curve).
-
This can be done:
- En bloc: multiple levels rotated simultaneously
- Segmental: each individual level derotated separately
-
Rod insertion: A pre-contoured rod (for sagittal plane correction) is placed on the concave side first.
-
Rod rotation maneuver (RRM) is performed first (translates apex toward midline, corrects coronal plane), then DVR is performed on top of it for transverse plane correction.
-
After derotation, tighten all set screws and check MEPs again.
-
Place convex rod, apply compression/distraction as needed for final balancing.
Mechanism of Action
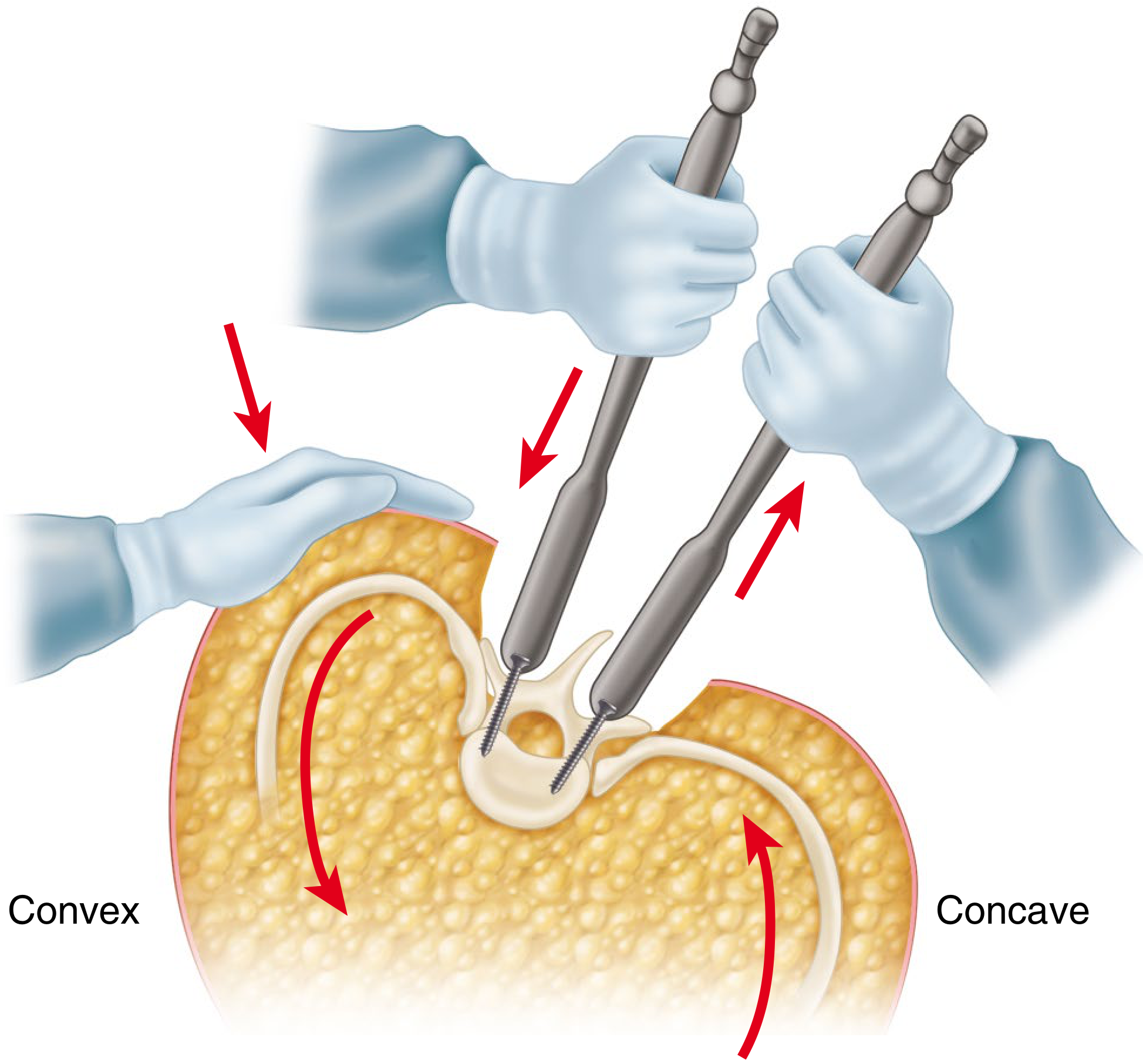
FIGURE 40.67 - Direct Vertebral Rotation. Derotation instruments on bilateral pedicle screws; arrows show convex side pushed down and concave side elevated to achieve vertebral derotation. (Campbell's Operative Orthopaedics 15th Ed, Technique 40.14)
The derotation force is applied directly to the vertebral body through the pedicle screw-derotator assembly:
- On the convex side: downward force applied to the screw (pushing the prominent transverse process/rib posteriorly down)
- On the concave side: upward lifting force applied
- Net result: the vertebral body rotates back toward neutral, reducing the rib hump
DVR vs. Simple Rod Derotation (Rod Rotation Maneuver)
| Parameter | DVR | Simple Rod Rotation |
|---|---|---|
| Mechanism | Direct force on vertebral body via screws | Indirect via rod-screw friction |
| Rotational correction | 42.5% improvement | Only 2.4% improvement |
| Coronal correction | 79.6% (thoracic), 80.5% (lumbar) | 68.9% (thoracic), 62.2% (lumbar) |
| LIV tilt correction | 80.6% | 66.3% |
| 3D correction | Yes (all 3 planes) | Mainly coronal and sagittal |
| Implant requirement | All-pedicle-screw construct (bilateral) | Single rod with hooks/screws possible |
| Stress on screws | Higher | Lower |
| Operation time | Longer | Shorter |
(Data: Lee SM, Suk SI, Chung ER. Spine 2004;29:343 - 38 AIS patients, min 2-yr follow-up)
Advantages of DVR
- True 3D correction - addresses the transverse plane (axial rotation) which rod rotation alone cannot reliably correct
- Significantly better rotational correction (42.5% vs. 2.4%)
- Better coronal plane correction
- Reduces the rib hump - the most visible cosmetic deformity in thoracic scoliosis
- Can be performed en bloc or segmentally depending on curve flexibility
- Applicable to rigid and severe curves
Disadvantages / Complications
- Requires bilateral all-pedicle-screw construct - technically demanding
- Longer operative time and greater blood loss
- Higher stress on pedicle screws - risk of screw pullout or plow
- Neurological risk if MAP drops or MEPs are not monitored
- Some recent studies (2023) suggest DVR may not offer superior clinical/radiological results compared to Differential Rod Contouring (DRC) in all patients
Flowchart: DVR Technique
PATIENT WITH AIS (Thoracic Curve with Rotational Deformity)
|
▼
Decision for Posterior Spinal Fusion
|
▼
Insert BILATERAL PEDICLE SCREWS at all levels to be fused
|
▼
Establish Baseline MEPs + Maintain MAP ≥ 70 mmHg
|
▼
Identify NEUTRAL VERTEBRA (least rotated) — begin derotation proximal to this level
|
▼
Place PRE-CONTOURED ROD on concave side (sagittal contour)
|
▼
Perform ROD ROTATION MANEUVER (RRM) — corrects coronal plane
|
▼
Attach SCREW DEROTATORS (SUK tubes) to bilateral pedicle screws
at apical + juxta-apical vertebrae
|
▼
┌─────────────────────────────┐
│ DIRECT VERTEBRAL │
│ ROTATION (DVR) │
│ │
│ Right thoracic curve → │
│ Rotate CLOCKWISE │
│ (opposite to vertebral │
│ rotation direction) │
│ │
│ En Bloc OR Segmental │
└─────────────────────────────┘
|
▼
Tighten all SET SCREWS
|
▼
Check MEPs (post-maneuver)
|
▼
Place CONVEX ROD — compression/distraction
|
▼
Final balancing + lock all screws
|
▼
POST-OP: Early mobilization (POD#1), pain control (PCA/gabapentin/ketorolac)
|
▼
RESULT: 3D Correction — Coronal + Sagittal + TRANSVERSE PLANE
Key Points for Exam
| Point | Detail |
|---|---|
| Introduced by | Lee SM, Suk SI, Chung ER (2004) |
| Publication | Spine 2004;29:343 |
| Indication | AIS (primarily thoracic curves) |
| Key requirement | Bilateral all-pedicle-screw construct |
| Direction of rotation | Opposite to vertebral rotation (clockwise for right thoracic) |
| MAP requirement | ≥ 70 mmHg |
| Rotational correction | 42.5% (vs 2.4% with rod rotation) |
| En bloc vs segmental | Both methods described |
| Instruments | SUK derotation tubes / screw derotators |
| Start level | Proximal to neutral vertebra distally |
| Main advantage | True 3D correction, transverse plane derotation |
| Monitoring | MEPs before and after each maneuver |
Reference: Campbell's Operative Orthopaedics 15th Ed 2026, Technique 40.14 - Lee SM, Suk SI, Chung ER. Direct vertebral rotation: a new technique of three-dimensional deformity correction with segmental pedicle screw fixation in adolescent idiopathic scoliosis. Spine 2004;29:343
This is a shared conversation. Sign in to Orris to start your own chat.