tachycardia
Reading File
Asking for Preferences
Finding Sources
Searching the Web
tachycardia classification overview types 2024
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a thorough overview. Let me compile the full response.
Tachycardia - Overview & Classification
Definition: Heart rate ≥ 100 beats/min. It can be a normal physiological response (sinus tachycardia) or reflect underlying pathology (arrhythmic tachycardia).
Classification Framework
The primary ECG-based framework divides all tachycardias by QRS width and rhythm regularity:
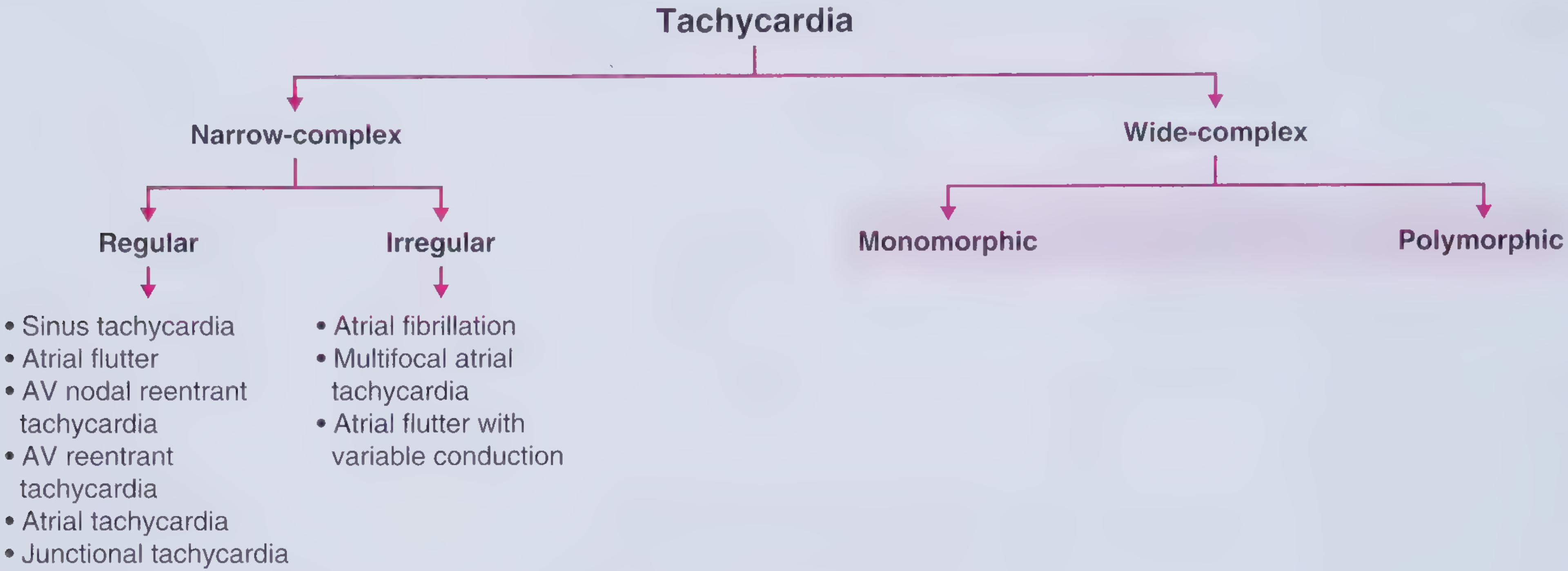
1. Narrow-Complex Tachycardia (QRS < 120 ms)
Reflects rapid activation via the normal His-Purkinje system, so the origin is at or above the His bundle (supraventricular).
A. Regular Narrow-Complex Tachycardias
| Type | Key Features |
|---|---|
| Sinus Tachycardia | Normal P waves before each QRS; rate rarely >170 bpm in adults; gradual onset/offset; usually a physiological response |
| Atrial Flutter | Sawtooth flutter waves ~300/min; 2:1, 3:1, or 4:1 AV block gives regular ventricular rate |
| AVNRT (AV nodal reentrant tachycardia) | Most common paroxysmal SVT; reentry circuit within AV node; P waves buried in or just after QRS |
| AVRT (AV reentrant tachycardia) | Requires accessory pathway (e.g., WPW); P wave after QRS in the ST segment |
| Atrial Tachycardia | Abnormal P wave morphology; focus outside sinus node; rate 100-240/min |
| Junctional Tachycardia | Origin in AV junction; inverted or absent P waves |
B. Irregular Narrow-Complex Tachycardias
| Type | Key Features |
|---|---|
| Atrial Fibrillation | Most common sustained arrhythmia; irregularly irregular rhythm; no distinct P waves; 300-600 atrial impulses/min; ventricular rate typically ≤150-170/min |
| Multifocal Atrial Tachycardia (MAT) | ≥3 distinct P-wave morphologies; classically seen with COPD |
| Atrial Flutter with variable conduction | Flutter waves with changing AV block ratio |
2. Wide-Complex Tachycardia (QRS ≥ 120 ms)
Indicates abnormally slow ventricular activation. Three major causes:
- Origin below the His bundle (ventricular tachycardia)
- SVT with pre-existing bundle branch block
- SVT with rate-dependent aberrant conduction
A. Monomorphic Wide-Complex (uniform QRS morphology)
Regular:
- Monomorphic VT - most often from myocardial scar (ischemic heart disease); H-V interval shorter than normal on EPS
- SVT with BBB - same SVT as above but QRS widens due to baseline or rate-related bundle branch block
- Pacemaker-mediated tachycardia
Irregular:
- AF with aberrancy (BBB or accessory pathway)
- AF with WPW - ventricular rate can exceed 200/min; AV nodal blockers are contraindicated
B. Polymorphic Wide-Complex (variable QRS morphology)
- Torsades de Pointes - associated with prolonged QT interval; twisting QRS axis around baseline
- Polymorphic VT - often in setting of acute ischemia or channelopathies (Brugada, catecholaminergic)
- Ventricular fibrillation - chaotic, no organized QRS; cardiac arrest
Mechanism Categories
| Mechanism | Examples |
|---|---|
| Reentry | AVNRT, AVRT, atrial flutter, most VT |
| Enhanced automaticity | Sinus tachycardia, atrial tachycardia, accelerated idioventricular rhythm |
| Triggered activity | Torsades de Pointes (EADs), digoxin toxicity (DADs) |
Physiological vs. Pathological Sinus Tachycardia
Sinus tachycardia is almost always a compensatory response - treating it without addressing the underlying cause is counterproductive. Common causes include:
- Sympathetic excess: pain, anxiety, fever, hyperthyroidism, drugs/stimulants
- Reduced perfusion: hypovolemia, anemia, hypoxemia, sepsis
- Cardiac: decompensated heart failure, PE, tamponade
Key Diagnostic Tool: QRS Width + Regularity on ECG
- Is QRS narrow or wide? → Narrows to SVT vs. VT
- Is the rhythm regular or irregular? → Identifies AF, flutter, MAT
- What do the P waves look like? → Determines atrial origin
- What is the P:QRS relationship? → Distinguishes AVNRT, AVRT, AT
- EPS (electrophysiology study): H-V interval distinguishes SVT (normal or prolonged H-V) from VT (short or absent H-V) when ECG is equivocal - per Braunwald's Heart Disease
Sources: Frameworks for Internal Medicine | ROSEN's Emergency Medicine 10e | Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.