Hormones invovled for eaarly onset of puberty
Reading File
Finding Sources
Searching PubMed
"precocious puberty"[MeSH Terms] AND hormones
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Now I have comprehensive information from multiple authoritative textbooks. Here is a thorough answer:
Hormones Involved in Early Onset of Puberty (Precocious Puberty)
Precocious puberty is defined as the appearance of secondary sexual characteristics before age 8 years in girls and 9 years in boys. It is classified into two major types based on which hormones are involved.
1. Central (GnRH-Dependent) Precocious Puberty
This is premature activation of the hypothalamic-pituitary-gonadal (HPG) axis - the same hormonal sequence as normal puberty, just too early.
Key Hormones
| Hormone | Source | Role |
|---|---|---|
| GnRH (Gonadotropin-Releasing Hormone) | Hypothalamus | Pulsatile release triggers the entire cascade |
| Kisspeptin | Hypothalamic neurons | The master "switch" that stimulates GnRH neurons; elevated kisspeptin is directly associated with precocious puberty |
| LH (Luteinizing Hormone) | Anterior pituitary | Stimulates gonadal sex steroid production |
| FSH (Follicle-Stimulating Hormone) | Anterior pituitary | Promotes gonadal maturation |
| Estradiol (girls) | Ovaries | Drives breast development (thelarche), uterine growth, and bone maturation |
| Testosterone (boys) | Testes (Leydig cells) | Drives penile/testicular growth, pubic hair, muscle mass |
Genetic regulators implicated:
- KISS1 (kisspeptin gene) - activating mutations cause precocious puberty
- KISS1R (kisspeptin receptor / GPR54) - activating mutations cause precocious puberty
- MKRN3 (Makorin ring finger protein 3) - loss-of-function mutations remove the "brake" on pulsatile GnRH secretion, allowing premature HPG axis activation
- DLK1 (Delta-like homolog 1) - a kisspeptin regulator; loss-of-function mutations associated with precocious puberty
Kisspeptin and its receptor GPR54 are essential regulators of GnRH-induced gonadotropin secretion and pubertal onset. Elevated kisspeptin levels are directly associated with precocious puberty. - Goldman-Cecil Medicine
2. Peripheral (GnRH-Independent) Precocious Puberty
Sex steroids are produced autonomously, without LH/FSH stimulation. LH and FSH are actually suppressed or low.
Key Hormones & Their Sources
| Hormone | Source | Condition |
|---|---|---|
| Estrogen | Ovarian cysts/tumors, McCune-Albright syndrome | Autonomous estrogen production |
| Androgens (DHEA, androstenedione, testosterone) | Adrenal glands | Congenital Adrenal Hyperplasia (CAH) - due to 21α-hydroxylase or 11β-hydroxylase deficiency |
| hCG (human Chorionic Gonadotropin) | hCG-secreting tumors | Acts like LH to stimulate testicular testosterone |
| Testosterone | Leydig cell tumors, adrenal tumors | Autonomous androgen secretion |
| Adrenal androgens (DHEAS) | Adrenal cortex | Premature adrenarche |
Key diagnostic clue: High testosterone + suppressed LH = gonadotropin-independent (peripheral) type.
Hormone Axis Summary
HYPOTHALAMUS
↓ GnRH (pulsatile) — driven by Kisspeptin (KISS1/KISS1R)
inhibited by MKRN3, DLK1
ANTERIOR PITUITARY
↓ LH + FSH
GONADS / ADRENALS
↓ Estradiol (girls) / Testosterone (boys) / Androgens
PERIPHERAL EFFECTS
→ Breast development, pubic hair, growth spurt, bone maturation
Additional Hormones That Modulate Pubertal Timing
- IGF-1 / Growth Hormone: Accelerated linear growth is a hallmark of precocious puberty; GH/IGF-1 axis amplifies the pubertal growth spurt
- Adrenal androgens (DHEA, DHEAS): Drive premature adrenarche (pubic/axillary hair) independently of the HPG axis
- Leptin: Body fat-derived; acts as a permissive signal for GnRH release; higher adiposity/leptin may lower the age of pubertal onset
- RFamide-related peptides (RFRPs): Act as endogenous inhibitors of GnRH neurons; reduced RFRP signaling may contribute to earlier pubertal activation
Diagnostic Hormone Measurements
When precocious puberty is suspected, the following are measured:
- Serum LH, FSH - to distinguish central vs. peripheral
- Testosterone or Estradiol - to confirm sex steroid excess
- 17α-hydroxyprogesterone - elevated in 21α-hydroxylase CAH
- DHEAS - elevated in adrenal causes
- GnRH stimulation test - LH rise confirms central (GnRH-dependent) puberty
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Goldman-Cecil Medicine | Textbook of Family Medicine 9e
Define spermatogensis regulation and stages
Finding Sources
Searching PubMed
"spermatogenesis"[MeSH Terms] AND regulation
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete, textbook-based answer:
Spermatogenesis: Definition, Stages, and Regulation
Definition
Spermatogenesis is the entire process by which primitive diploid germ cells (spermatogonia) are transformed into mature haploid spermatozoa within the seminiferous tubules of the testes. It begins at puberty (average age 13) and continues throughout most of adult life. The complete process takes approximately 74 days in humans.
Anatomical Setting
The seminiferous tubules house two key cell types:
- Sertoli cells - "nurse cells" that support, nourish, and regulate germ cell development
- Leydig cells - interstitial cells that produce testosterone under LH stimulation
Stages of Spermatogenesis
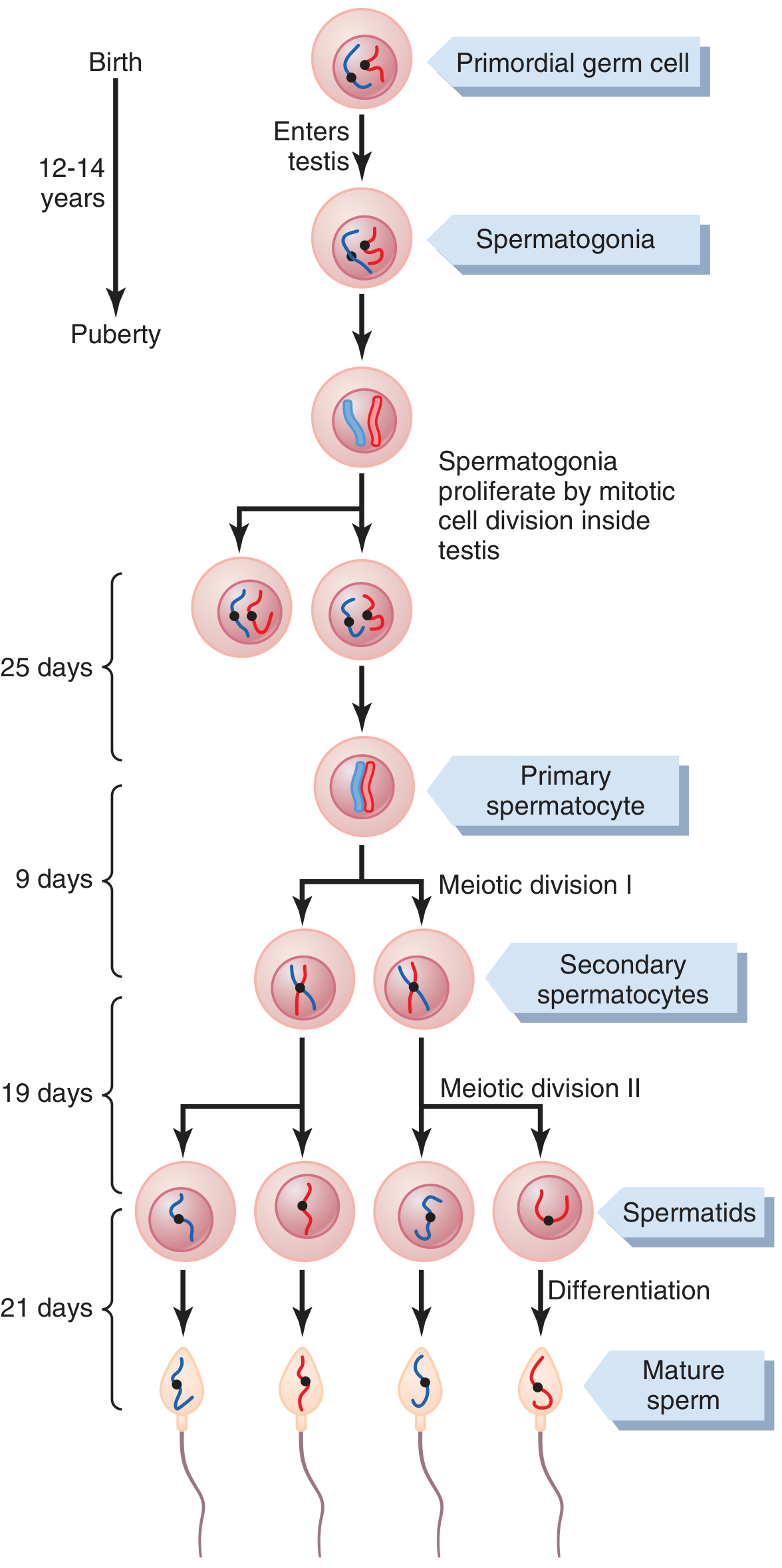
Stage 1 - Proliferative (Mitotic) Phase (~25 days)
Spermatogonia lie on the basal lamina of the seminiferous tubules. They are of two main types:
| Type | Fate |
|---|---|
| Type A (dark) | Self-renewing stem cells - maintain the germ cell pool |
| Type A (pale) | Committed progenitors - divide mitotically |
| Type B | Differentiate into primary spermatocytes |
- Type B spermatogonia undergo mitosis to produce primary spermatocytes (still diploid, 46 chromosomes)
- Descendants remain connected by cytoplasmic bridges, ensuring synchrony of differentiation
- One spermatogonium ultimately yields ~512 spermatids
Stage 2 - Meiotic Phase
Meiosis I (~9 days)
- Primary spermatocytes (2n, 4C) undergo the first meiotic division (reductional division)
- Homologous chromosome pairs separate
- Result: 2 secondary spermatocytes (haploid, 23 chromosomes each, but still with 2 chromatids each)
- Crossing over (genetic recombination) occurs during prophase I, generating genetic diversity
Meiosis II (~19 days)
- Secondary spermatocytes undergo the second meiotic division rapidly (equational division)
- Sister chromatids separate
- Result: 4 spermatids (23 chromosomes, haploid, 1C each)
- 1 primary spermatocyte → 4 genetically distinct spermatids
Stage 3 - Spermiogenesis (~21 days)
This is the morphological transformation of round spermatids into mature spermatozoa - no further cell division occurs.
Key changes:
- Acrosome formation - from the Golgi apparatus; cap-like structure over the anterior 2/3 of the nucleus; contains hyaluronidase and proteolytic enzymes needed for ovum penetration
- Nuclear condensation - chromatin condenses tightly; nucleus elongates
- Tail (flagellum) formation - from the centriole; composed of:
- Central axoneme (11 microtubule arrangement: 9+2)
- Mitochondrial sheath around the midpiece (energy source via ATP)
- Cytoplasm shedding - excess cytoplasm discarded as residual bodies, phagocytosed by Sertoli cells
- Spermiation - mature spermatozoa released from Sertoli cell cytoplasm into the tubule lumen
Stage 4 - Epididymal Maturation
Spermatozoa leaving the testis are not yet motile. During passage through the epididymis they acquire:
- Progressive forward motility (via CatSper Ca²⁺ channels)
- Capacitation potential (final activation in the female tract)
- Zona-binding ability
Summary of Cell Progression
Spermatogonia (2n)
↓ Mitosis (×several rounds)
Primary Spermatocyte (2n, 4C)
↓ Meiosis I
Secondary Spermatocyte (n, 2C) × 2
↓ Meiosis II
Spermatids (n, 1C) × 4
↓ Spermiogenesis (morphological differentiation)
Mature Spermatozoa × 4
Regulation of Spermatogenesis
Hormonal Control (Endocrine)
The Hypothalamic-Pituitary-Gonadal axis is the master regulator:
Hypothalamus
↓ GnRH (pulsatile)
Anterior Pituitary
↓ LH + FSH
Testes
LH → Testosterone (via Leydig cells)
- LH binds to Leydig cells in the interstitial tissue
- Stimulates synthesis of testosterone via the cAMP-PKA pathway
- Testosterone diffuses into the seminiferous tubules
- Testosterone (and DHT) has a strong tropic effect on spermatogenesis, particularly on the spermatid → spermatozoa maturation step
- Essential for maintaining the blood-testis barrier
FSH → Sertoli cell activation
- FSH binds to Sertoli cells (FSH receptors are exclusive to Sertoli cells)
- Activates adenylyl cyclase → ↑cAMP → PKA → gene transcription
- Sertoli cells then produce critical regulatory products:
| Product | Function |
|---|---|
| Androgen-Binding Protein (ABP) | Keeps testosterone concentration high in tubular fluid near developing sperm |
| Aromatase (CYP19) | Converts testosterone to estradiol; estrogen receptors (ERα) in rete testis help concentrate sperm |
| Inhibin B | Negative feedback on FSH secretion at the pituitary |
| Growth factors, cytokines | Paracrine support of germ cell development |
| Mullerian Inhibiting Substance (MIS) | Causes regression of Mullerian ducts in male development |
"FSH and androgens maintain the gametogenic function of the testis. Both FSH and testosterone are necessary to initiate spermatogenesis." - Ganong's Review of Medical Physiology
Negative Feedback Loops
Two parallel feedback loops prevent over- or under-production:
Loop 1 - Testosterone feedback:
- ↑Testosterone → acts on hypothalamus to ↓GnRH → ↓LH → ↓testosterone production
- Also inhibits LH directly at the pituitary level
Loop 2 - Inhibin feedback:
- When spermatogenesis is excessive → Sertoli cells secrete more Inhibin B → directly inhibits FSH at the pituitary
- When seminiferous tubules fail → Inhibin falls → FSH rises markedly
- Inhibin B is a glycoprotein heterodimer (α + β subunit), member of the TGF-β superfamily
Paracrine Regulation (Local)
- Sertoli-to-germ cell crosstalk: Sertoli cells provide direct physical support, nutrients, and paracrine signals throughout all stages of development
- Leydig-to-Sertoli crosstalk: Testosterone from Leydig cells signals Sertoli cells; Sertoli-derived growth factors in turn regulate Leydig cell function
- Activins: Counterbalance inhibins; stimulate FSH secretion and spermatogonial proliferation
Temperature Requirement
Spermatogenesis requires testicular temperature of ~32°C (about 5°C below core body temperature). This is maintained by:
- Scrotal position outside the body cavity
- Countercurrent heat exchange between spermatic arteries and veins
- Cryptorchidism (undescended testes) results in infertility due to heat-induced damage to germ cells
Key Regulatory Hormones at a Glance
| Hormone | Source | Target | Effect |
|---|---|---|---|
| GnRH | Hypothalamus | Anterior pituitary | Stimulates LH + FSH release |
| LH | Anterior pituitary | Leydig cells | Stimulates testosterone synthesis |
| FSH | Anterior pituitary | Sertoli cells | Activates spermatogenesis support functions |
| Testosterone | Leydig cells | Sertoli cells + germ cells | Essential for spermatid maturation; negative feedback on GnRH/LH |
| Estradiol | Sertoli cells (via aromatase) | Rete testis | Fluid reabsorption; sperm concentration |
| Inhibin B | Sertoli cells | Anterior pituitary | Negative feedback - inhibits FSH |
| ABP | Sertoli cells | Tubule lumen | Concentrates testosterone near germ cells |
| DHT | Converted from testosterone | Sertoli/germ cells | Strong androgen effect (more potent than testosterone) |
Sources: Guyton & Hall Textbook of Medical Physiology | Ganong's Review of Medical Physiology 26e | Medical Physiology (Boron & Boulpaep) | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.