Cardiac output and venous return mbbs 1st year physiology notes
Reading File
search_medical_text
cardiac output definition determinants heart rate stroke volume
search_medical_text
venous return factors affecting mean systemic filling pressure Guyton
search_medical_image
cardiac output venous return curve Starling Frank Starling mechanism
GradeResponse
GradeResponse
GradeResponse
search_medical_text
Frank Starling law of heart preload afterload contractility stroke volume regulation
search_medical_text
cardiac output measurement Fick principle thermodilution normal values 5 liters
GradeResponse
GradeResponse
Here are comprehensive MBBS 1st year physiology notes on Cardiac Output and Venous Return:
Cardiac Output & Venous Return
MBBS 1st Year Physiology Notes
1. CARDIAC OUTPUT (CO)
Definition
Cardiac Output is the volume of blood pumped by each ventricle per minute.
CO = Heart Rate (HR) × Stroke Volume (SV)
| Parameter | Normal Value |
|---|---|
| Cardiac Output | 5 L/min (at rest) |
| Heart Rate | 72 beats/min |
| Stroke Volume | ~70 mL/beat |
| Cardiac Index | 3.2 L/min/m² (CO / BSA) |
| End-Diastolic Volume (EDV) | ~120–130 mL |
| End-Systolic Volume (ESV) | ~50–60 mL |
| Ejection Fraction (EF) | 60–70% (SV/EDV × 100) |
2. DETERMINANTS OF CARDIAC OUTPUT
CO is determined by Heart Rate and Stroke Volume. Stroke volume itself is controlled by three factors:
A. PRELOAD
- The ventricular filling pressure (or end-diastolic fiber length/volume) just before contraction
- Reflects the stretch on myocardial fibers at the end of diastole
- Equivalent to Left Ventricular End-Diastolic Pressure (LVEDP) or LVEDV
- Increased by: ↑ venous return, bradycardia, hypervolemia
- Decreased by: venodilation, blood loss, tachycardia
B. AFTERLOAD
- The resistance/load the ventricle must overcome to eject blood
- For left ventricle → Total Peripheral Resistance (TPR) / Systemic Vascular Resistance (SVR)
- For right ventricle → Pulmonary Vascular Resistance (PVR)
- ↑ Afterload → ↓ Stroke Volume (heart works harder, ejects less)
- ↓ Afterload → ↑ Stroke Volume
C. MYOCARDIAL CONTRACTILITY (Inotropy)
- The intrinsic ability of the heart to contract at a given preload and afterload
- Independent of preload and afterload
- Increased by: sympathetic stimulation, catecholamines, digoxin, Ca²⁺, thyroid hormones
- Decreased by: heart failure, acidosis, hypoxia, beta-blockers, calcium channel blockers
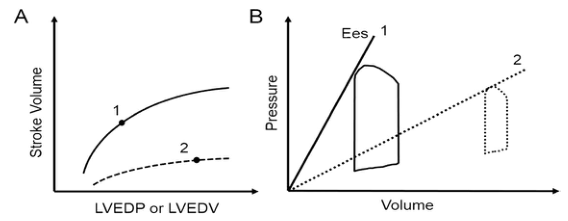
3. FRANK-STARLING LAW OF THE HEART
"The energy of contraction is proportional to the initial length of the cardiac muscle fiber."
- ↑ Preload → ↑ stretch of myocardial fibers → ↑ actin-myosin overlap → ↑ force of contraction → ↑ Stroke Volume → ↑ CO
- This is an intrinsic autoregulatory mechanism
- The heart automatically adjusts its output to match venous return
- Operates within physiological limits — excessive stretch causes decline (descending limb in failing heart)
Clinical Significance:
- Explains why both ventricles pump equal volumes despite different pressures
- Basis for use of IV fluids in shock (↑ preload → ↑ CO)
(Harrison's Principles of Internal Medicine, 21st Ed., p. 6724)
4. HEART RATE AND ITS EFFECT ON CO
| Condition | HR | SV | CO |
|---|---|---|---|
| Moderate tachycardia | ↑ | Slight ↓ (less filling time) | ↑ |
| Severe tachycardia (>180/min) | ↑↑ | ↓↓ (very short diastole) | ↓ |
| Bradycardia | ↓ | ↑ (more filling) | May ↓ |
| Trained athlete at rest | ↓ (50–60) | ↑ (100–120 mL) | Normal/↑ |
Regulators of HR:
- Autonomic NS: Sympathetic (↑ HR via β₁) / Parasympathetic (↓ HR via M₂ receptors)
- Bainbridge Reflex: ↑ venous return → ↑ atrial stretch → ↑ HR (via vagal afferents and sympathetic efferents)
- Chemicals: Epinephrine (↑ HR), ACh (↓ HR), thyroid hormones (↑ HR)
5. MEASUREMENT OF CARDIAC OUTPUT
A. Fick's Principle
CO = O₂ Consumption / (Arterial O₂ content – Venous O₂ content)
- Uses oxygen as the indicator substance
- Most reliable in low-output states and tricuspid regurgitation
- Normal A-V O₂ difference: ~5 mL/100 mL blood
Example:
- O₂ consumption = 250 mL/min
- Arterial O₂ = 20 mL/100 mL; Venous O₂ = 15 mL/100 mL
- CO = 250 / (20-15) × 100 = 5000 mL/min = 5 L/min
(Harrison's Principles of Internal Medicine, 21st Ed., p. 6907)
B. Thermodilution Method
- Cold saline injected into right atrium via Swan-Ganz catheter
- Temperature change measured at pulmonary artery
- Area under temperature-time curve is inversely proportional to CO
- Most commonly used in ICU settings
C. Doppler Echocardiography
- Non-invasive
- Measures flow velocity across aortic valve
6. VENOUS RETURN
Definition
Venous return (VR) is the volume of blood flowing back to the right heart per minute. Under steady state: Venous Return = Cardiac Output = 5 L/min
(Bailey & Love's Short Practice of Surgery, 28th Ed., p. 1047)
7. FACTORS AFFECTING VENOUS RETURN
A. Mean Systemic Filling Pressure (MSFP)
- The pressure that drives blood from periphery to right atrium
- Normal MSFP ≈ 7 mmHg; Right atrial pressure ≈ 0–2 mmHg
- VR = (MSFP – Right Atrial Pressure) / Venous Resistance
- ↑ MSFP (e.g., blood transfusion, sympathetic venoconstriction) → ↑ VR
B. Blood Volume
- ↑ Blood volume → ↑ venous pressure → ↑ VR (e.g., IV fluid infusion)
- ↓ Blood volume → ↓ VR (e.g., hemorrhage)
C. Venous Tone (Venomotor Tone)
- Veins contain ~60–70% of total blood volume (act as capacitance vessels)
- Sympathetic stimulation → venoconstriction → ↑ MSFP → ↑ VR
- Venodilation (e.g., nitroglycerin) → ↓ VR
D. Skeletal Muscle Pump
- Muscular contractions compress veins → pushes blood toward heart
- Venous valves ensure one-way flow
- Important during exercise — ↑ VR by up to 4–5 times
E. Respiratory Pump (Thoracic Pump)
- Inspiration → ↓ intrathoracic pressure → ↑ venous filling of right atrium → ↑ VR
- Positive pressure ventilation (mechanical) → ↑ intrathoracic pressure → ↓ VR
F. Gravity / Posture
- Upright posture → blood pools in lower limbs → ↓ VR (orthostatic hypotension)
- Supine / head-down position → ↑ VR
G. Right Atrial Pressure (RAP)
- ↑ RAP (e.g., right heart failure, cardiac tamponade) → ↓ venous pressure gradient → ↓ VR
8. GUYTON'S CONCEPT: CO-VR EQUILIBRIUM
Guyton described the interaction using two curves plotted on the same graph:
| Curve | What it shows |
|---|---|
| Cardiac Function Curve (Starling curve) | ↑ Right atrial pressure → ↑ CO (up to a limit) |
| Venous Return Curve | ↑ Right atrial pressure → ↓ VR (less gradient) |
- Equilibrium Point = where both curves intersect = normal operating point (CO = VR = 5 L/min, RAP ≈ 0 mmHg)
- Changes in contractility shift the cardiac function curve
- Changes in blood volume / venomotor tone shift the venous return curve
9. REGULATION OF CARDIAC OUTPUT
Short-term (Beat-to-beat)
| Mechanism | Effect |
|---|---|
| Frank-Starling (Heterometric) | ↑ EDV → ↑ SV |
| Sympathetic stimulation | ↑ HR + ↑ Contractility |
| Parasympathetic stimulation | ↓ HR |
| Bainbridge Reflex | ↑ Venous return → ↑ HR |
Long-term
| Mechanism | Effect |
|---|---|
| Renin-angiotensin-aldosterone (RAAS) | ↑ Blood volume → ↑ CO |
| ADH (Vasopressin) | ↑ Water retention → ↑ CO |
| Atrial Natriuretic Peptide (ANP) | ↓ Blood volume → ↓ CO |
10. CHANGES IN CO IN PHYSIOLOGICAL & PATHOLOGICAL STATES
| Condition | CO Change | Mechanism |
|---|---|---|
| Exercise | ↑ (up to 25–30 L/min) | ↑ HR + ↑ SV + skeletal muscle pump |
| Pregnancy | ↑ by 40–50% | ↑ blood volume, ↓ SVR |
| Fever | ↑ | ↑ HR, ↑ metabolic demand |
| Anaemia | ↑ | ↓ viscosity, ↑ HR |
| Sleep | ↓ | ↓ HR, ↓ metabolic demand |
| Heart failure | ↓ | ↓ Contractility |
| Hemorrhagic shock | ↓↓ | ↓ Venous return, reflex tachycardia |
| Hyperthyroidism | ↑ | ↑ HR, ↑ contractility |
11. QUICK SUMMARY TABLE
| Term | Definition | Normal Value |
|---|---|---|
| CO | HR × SV | 5 L/min |
| CI | CO / BSA | 3.2 L/min/m² |
| SV | EDV − ESV | ~70 mL |
| EF | SV/EDV × 100 | 60–70% |
| Preload | LVEDP/LVEDV | ↑ → ↑ SV |
| Afterload | SVR/PVR | ↑ → ↓ SV |
| MSFP | Driving pressure for VR | ~7 mmHg |
| Venous blood volume | % in venous system | ~60–70% |
Key One-Liners for Exams
- CO = HR × SV
- Frank-Starling law: length–tension relationship of cardiac muscle
- Veins are capacitance vessels; arteries are resistance vessels
- At equilibrium, VR always equals CO in steady state
- Fick's method is gold standard for CO measurement
- The biggest reservoir of blood: venous system (60–70%)
- Most important intrinsic regulator of CO: Frank-Starling mechanism
- Most important extrinsic regulator of CO: Sympathetic nervous system
This is a shared conversation. Sign in to Orris to start your own chat.