Chloroquine
Reading File
Finding Sources
Searching PubMed
chloroquine pharmacology mechanism
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Here is a comprehensive overview of Chloroquine based on authoritative pharmacology textbooks.
Chloroquine
Class: Synthetic 4-aminoquinoline
Formulation: Chloroquine phosphate (oral)
Mechanism of Action
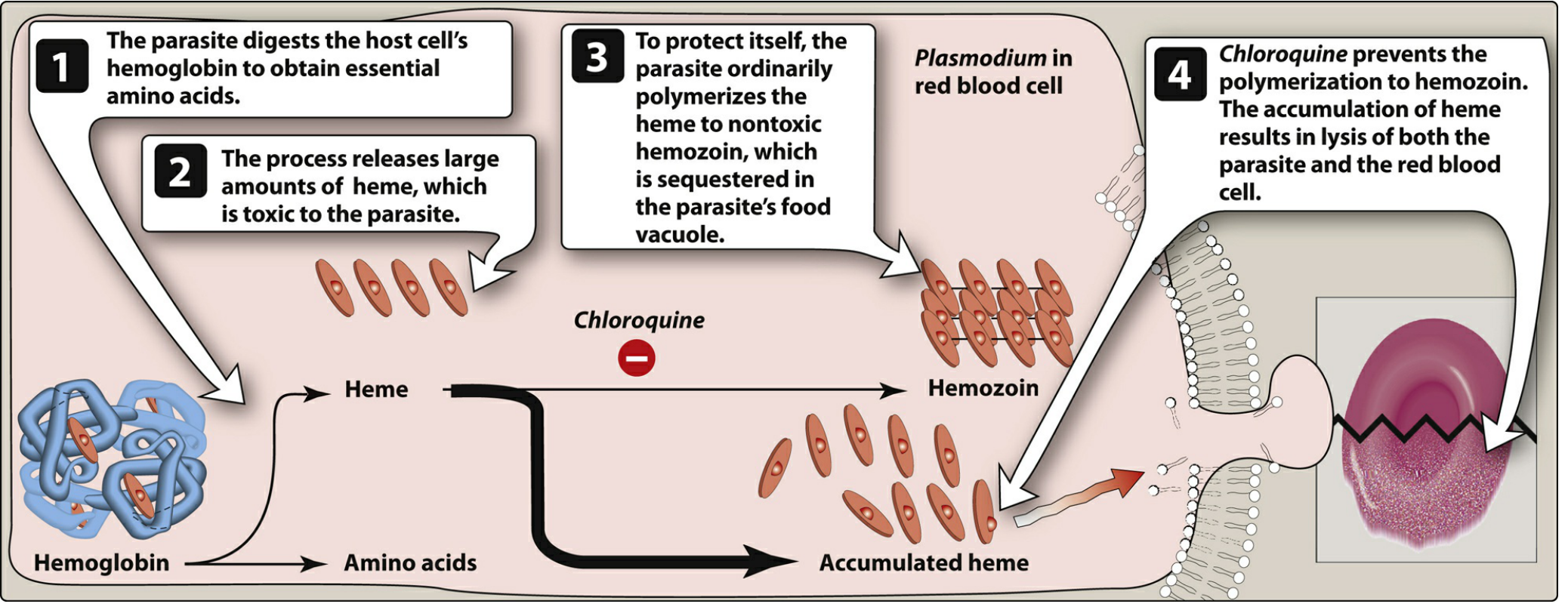
The parasite digests host red cell hemoglobin to extract amino acids, releasing large amounts of free heme as a byproduct. Free heme is toxic to the parasite, so it normally polymerizes heme into the inert crystal hemozoin in its food vacuole. Chloroquine, being a diprotic weak base, concentrates in the acidic food vacuole via ion trapping and specifically binds to heme, blocking its polymerization to hemozoin. The resulting accumulation of free heme causes oxidative damage to phospholipid membranes, leading to lysis of both the parasite and the red blood cell.
- Chloroquine is a blood schizonticide - it is NOT active against liver stage parasites or gametocytes.
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Rapid and nearly complete after oral dosing; peak plasma concentration ~3 hours |
| Volume of distribution | Very large: 100-1,000 L/kg |
| Distribution | Concentrates in erythrocytes, liver, spleen, kidney, lung, melanin-containing tissues (eye, skin), leukocytes |
| CNS penetration | Yes; also crosses the placenta |
| Metabolism | Hepatic dealkylation (mixed-function oxidase); metabolites retain some activity |
| Excretion | Primarily renal |
| Half-life | Initial: 3-5 days; terminal elimination: 1-2 months (slow tissue release) |
Clinical Uses
- Treatment of malaria - drug of choice for uncomplicated non-falciparum and chloroquine-sensitive P. falciparum malaria. Rapidly terminates fever (24-48 hours) and clears parasitemia (48-72 hours).
- Chemoprophylaxis - preferred agent in malarious regions without chloroquine-resistant P. falciparum.
- Amebic liver abscess - used for abscesses failing initial metronidazole therapy, because chloroquine reaches high liver concentrations.
- Rheumatologic diseases - used for rheumatoid arthritis and systemic lupus erythematosus (at higher, prolonged doses - though hydroxychloroquine is now generally preferred).
Important: Chloroquine does not eliminate dormant liver stages (hypnozoites) of P. vivax and P. ovale. Primaquine or tafenoquine must be added for radical cure of these species.
Resistance
Widespread resistance among P. falciparum (most endemic areas) and increasing in P. vivax. In P. falciparum, mutations in PfCRT (a putative transporter protein) are the primary mediators of resistance. Resistance can be partially reversed by verapamil, desipramine, and chlorpheniramine, though clinical value is unestablished.
Adverse Effects
At prophylactic (low) doses - generally very well tolerated.
Dose-dependent effects:
- GI: nausea, vomiting, abdominal pain, anorexia (reduced by taking with food)
- Pruritus (particularly common in Africans)
- Headache, blurred vision, malaise, urticaria
With prolonged high-dose use (e.g., for rheumatologic disease):
- Retinopathy (irreversible) - routine ophthalmologic exams required
- Ototoxicity (irreversible)
- Myopathy
- Peripheral neuropathy
- Discoloration of nail beds and mucous membranes
- Bleaching of hair
Serious/rare:
- QT prolongation - avoid combining with other QT-prolonging drugs
- Hemolysis in G6PD-deficient patients
- Hypotension, cardiac arrest (IV/IM route - should be avoided)
- Agranulocytosis, exfoliative dermatitis, psychosis, seizures
Contraindications
- Psoriasis - may precipitate acute attacks
- Porphyria - may provoke attacks
- Retinal/visual field abnormalities
- Pre-existing myopathy
- Caution in liver disease, neurologic disorders, hematologic disorders
Safe in: pregnancy and young children (at standard doses)
Drug Interactions
- Kaolin and antacids (calcium/magnesium) - impair chloroquine absorption; do not coadminister
- QT-prolonging drugs - additive risk of arrhythmia
Overdose / Toxicity (Emergency)
Toxicity typically begins within 3 hours of ingestion:
- Nausea, vomiting, diarrhea
- Cardiovascular collapse (QRS prolongation, AV block)
- Hypotension (more severe than quinine overdose)
- Respiratory depression, hypokalemia
- Neurologic: headache, obtundation, seizures
Management: Early intubation, gastric lavage, deep sedation with benzodiazepines, vasopressor support with epinephrine (target systolic BP ≥100 mmHg) - this regimen has demonstrated reduced mortality.
Sources: Lippincott Illustrated Reviews: Pharmacology, 7th ed.; Katzung's Basic and Clinical Pharmacology, 16th ed.; Tintinalli's Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.