Maggot wound treatment with images
Reading File
Finding Sources
Finding Sources
Searching the Web
maggot wound treatment myiasis clinical images debridement
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the essential images and content. Let me compile the comprehensive answer.
Maggot Wound Treatment (Maggot Debridement Therapy / Larval Therapy)
Maggot Debridement Therapy (MDT) uses sterile blow fly larvae (Lucilia sericata) to clean non-healing wounds. It is one of the oldest and most effective forms of biological debridement, with modern FDA-cleared use for chronic, non-healing wounds.
What Are Maggots Used For?
MDT is indicated for:
- Chronic, non-healing ulcers (diabetic foot ulcers, venous leg ulcers, pressure ulcers)
- Infected wounds with necrotic tissue (especially MRSA or multidrug-resistant organisms)
- Wounds unsuitable for surgical debridement (poor surgical candidates, coagulopathies)
- Wound myiasis - accidental infestation that requires larval removal
How Maggots Work - Three Mechanisms
- Debridement - Maggots secrete digestive enzymes that liquefy and digest necrotic tissue without harming healthy tissue. They also mechanically dislodge dead skin via mouth hooks and body spines.
- Stimulation of healing - Secretions promote granulation tissue and angiogenesis.
- Antimicrobial action - They consume bacteria (including MRSA), and their secretions have direct antimicrobial properties. This is particularly relevant in the era of antibiotic resistance.
Medical-Grade Maggots (Supply)
Medical maggots must be laboratory-bred and sterilized - they are NOT from the wild. In the US, they are supplied by Monarch Labs (250-500 larvae per vial, ~$90). They must be used within 24 hours of receipt.

Wound Types That Benefit from MDT
Before Treatment - Wound Prepared for MDT
This is a classic example of a lower leg ulcer with necrotic and mixed tissue, ready for maggot application:

Step-by-Step Application Technique
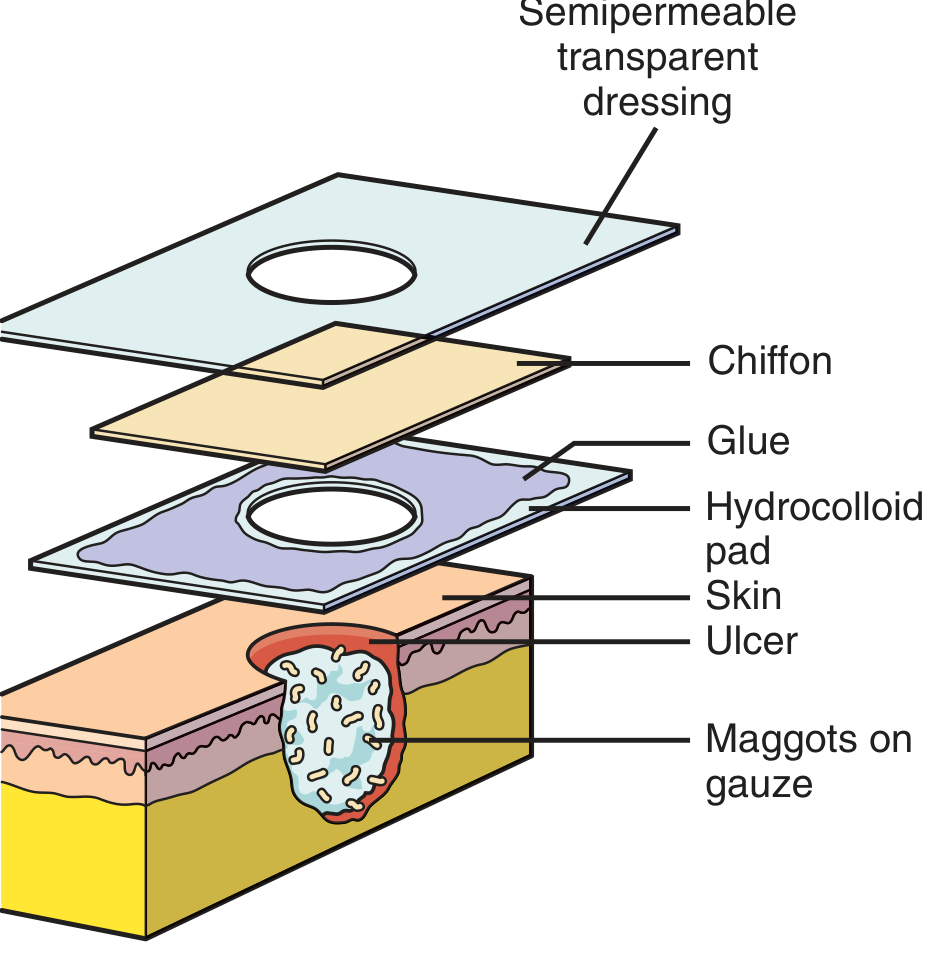
Dressing System Diagram
Step-by-Step Protocol
| Step | Action |
|---|---|
| 1 | Check maggot viability - confirm larvae moving in the vial |
| 2 | Apply protective skin prep (e.g., benzoin) to skin around wound |
| 3 | Cut a hydrocolloid "donut" dressing to fit around the wound perimeter (2-3 cm margin) |
| 4 | Apply hydrocolloid donut securely, wrinkle-free |
| 5 | Apply adhesive (benzoin) to the top of the hydrocolloid |
| 6 | Place plastic trash bag under body part to catch escaped larvae; apply maggots to wound bed using cotton-tipped applicators - dose: 5-8 maggots per cm² of wound area |
| 7 | Cover maggots with damp loosely fluffed gauze to keep wound moist |
| 8 | Apply Dacron/chiffon "cage" fabric over wound, adhered to hydrocolloid - this contains larvae while allowing gas exchange |
| 9 | Cover entire construct with semipermeable transparent dressing (not occlusive - maggots need oxygen) |
| 10 | Change dressing every 48-72 hours |
Do NOT use an occlusive dressing - maggots are aerobic and will die without oxygen access.
Removal of Maggots
- Dressing is changed every 48-72 hours
- Remove entire dressing system carefully
- Maggots will have grown (from ~1 mm to ~5-10 mm) and are usually concentrated in the necrotic tissue
- Apply ethyl chloride to slow/immobilize them before removal
- Count larvae in vs. out to confirm none remain in wound tunnels
- Dispose of larvae in biohazard (red) bags
- Most wounds require 2-3 cycles of maggot treatment; very large wounds may need up to 5-6 treatments
Wound Myiasis (Accidental Infestation)
Wound myiasis is different from therapeutic MDT - it is an accidental infestation of a pre-existing wound or ulcer by blowfly larvae (green/black blowflies, screwworm fly).
Who is at risk: Homeless individuals, those with alcohol use disorder, patients with poor wound care, immunocompromised, elderly
Clinical presentation:
- Painful, malodorous cutaneous or mucosal lesions
- Serosanguinous or purulent discharge
- Visibly motile larvae in wound/ulcer
- Rapidly expanding ulceration and tissue destruction (screwworm)
Treatment of Wound Myiasis:
| Approach | Details |
|---|---|
| Manual removal | Mechanical extraction of all visible larvae - mainstay of treatment |
| Irrigation | Copious wound irrigation to dislodge larvae |
| Surgical debridement | Usually not required unless patient requests; larvae naturally slough within 5-7 weeks |
| Chemical adjuncts | Chloroform in light vegetable oil or ether applied topically before larval removal under local anesthesia |
| Ivermectin | Off-label use - facilitates larval death; particularly useful for non-extractable screwworm larvae |
| Antibiotics | Broad-spectrum antibiotics for secondary pyogenic infection |
Caution: Always extract larvae whole - a fragmented larva causes significant foreign body reaction. Do NOT forcibly pull larvae that use spines/hooks to grip tissue; apply suffocation techniques first (petroleum jelly, chloroform oil).
Contraindications to Therapeutic MDT
- Wounds communicating with body cavities
- Wounds near major blood vessels (maggots can enlarge wound)
- Patients on anticoagulants or with coagulopathy - bleeding from wound bed can be severe
- Dry wounds (maggots need moisture to survive)
- Patient refusal
Evidence Summary
MDT is an effective debridement technique. A multicenter RCT in JAMA (2009) showed MDT achieved faster debridement than hydrogel but did not improve healing time overall. A Cochrane review on larval therapy confirmed its efficacy for removing necrotic tissue. MDT has particular value in antimicrobial-resistant wound infections.
A video overview of the science:
Sources: Pfenninger and Fowler's Procedures for Primary Care, 3rd ed., Ch. 44-45 | Fischer's Mastery of Surgery, 8th ed. | MSD Manual - Cutaneous Myiasis | PMC - Maggot Infestation Treatment Modalities
Maggot wound treatment with images in dogs
Searching the Web
maggot wound treatment dogs fly strike myiasis veterinary clinical images
Searching the Web
maggot debridement therapy dogs veterinary MDT larval therapy wound
Searching PubMed
maggot debridement therapy dogs veterinary wounds
Reading Web Page
https://www.cliniciansbrief.com/article/managing-maggots-bot…
Loading Image
Loading Image
Loading Image
Reading Web Page
https://www.vosd.in/treating-maggot-wounds-in-dogs
Loading Image
Loading Image
I have comprehensive content and images. Now let me compile the full answer.
Maggot Wound Treatment in Dogs
This covers two separate but related topics:
- Wound Myiasis (Fly Strike) - accidental infestation requiring emergency larval removal
- Maggot Debridement Therapy (MDT) - deliberate therapeutic use of sterile maggots to heal chronic wounds
PART 1 - Wound Myiasis (Fly Strike) in Dogs
Myiasis is the medical term for infestation of living tissue by fly larvae (maggots). In dogs, it is most commonly caused by:
- Lucilia sericata (green bottle fly) - facultative myiasis
- Cochliomyia hominivorax (New World screwworm) - obligatory myiasis, more destructive
- Cuterebra spp. (bot flies) - subcutaneous nodular myiasis
- Phormia and Phaenicia spp. (blowflies)
Who Is at Risk?
Dogs most vulnerable to fly strike:
- Open or untreated wounds
- Matted, soiled, or urine/feces-stained hair coats
- Chronic skin disease or skin folds
- Mobility-impaired, recumbent, or debilitated dogs
- Elderly dogs unable to self-groom
- Outdoor dogs in hot, humid weather
Clinical Appearance - Fly Strike in a Dog


Signs and Severity Classification
| Severity | Clinical Signs |
|---|---|
| Mild | Small wound, few visible larvae on surface, dog alert and eating, no systemic signs |
| Moderate | Larger wound, larvae burrowing into tissue, some surrounding necrosis, mild lethargy |
| Severe | Large/deep wound with subcutaneous tunnels, extensive necrosis (grey/black tissue margins), larvae visible as movement from a distance, dog lethargic, febrile, anorexic, possible shock |
Key danger: Larvae secrete proteolytic enzymes that liquefy living tissue, not just necrotic tissue. Crushed or fragmented larvae release these enzymes in large quantities, potentially causing systemic toxaemia and shock.
Emergency First Aid (Before Reaching the Vet)
- Isolate the dog from other animals; move indoors away from flies
- Clip hair around and beyond the wound thoroughly - hair hides larvae and traps moisture
- Remove visible surface larvae using tweezers, but gently - do NOT crush them
- Flush with clean water or dilute chlorhexidine to dislodge surface maggots
- Transport immediately to vet - do not delay based on apparent improvement after surface cleaning
Do NOT ignore tissue adjacent to the main wound. Larvae migrate. A visible wound may have satellite tunnels several centimetres away.
Veterinary Treatment Protocol
| Step | Treatment | Details |
|---|---|---|
| 1 | Sedation/anaesthesia | Most cases require sedation - removal is painful and stressful |
| 2 | Clip and expose | Thorough clipping of the entire region to reveal full extent of infestation |
| 3 | Manual larval removal | Careful hand extraction of all visible larvae - the primary treatment |
| 4 | Antiseptic lavage | Chlorhexidine or povidone-iodine wound cleaning and irrigation |
| 5 | Surgical debridement | Excision of necrotic/non-viable tissue; wound may be larger than it appears |
| 6 | Antiparasitic treatment | To kill remaining larvae not visible/accessible |
| 7 | Antibiotics | Broad-spectrum; continue minimum 14 days beyond clinical resolution |
| 8 | Supportive care | IV fluids, analgesia, anti-inflammatories for systemic cases |
| 9 | Wound management | Regular dressing changes; monitor for gangrene and secondary infection |
Antiparasitic Drugs Used in Dogs for Myiasis
| Drug | Route | Notes |
|---|---|---|
| Ivermectin | Injectable/oral | Kills remaining larvae; first-line systemic option |
| Nitenpyram | Oral | Fast-acting; reported efficacy |
| Spinosad + milbemycin | Oral | Combination product |
| Isoxazolines (fluralaner, sarolaner, afoxolaner) | Oral | Safe at label doses; effective |
| Pyrethrin | Topical | Applied to wound site in dogs only (NOT cats - toxic) |
PART 2 - Therapeutic Maggot Debridement Therapy (MDT) in Dogs
MDT is the deliberate, controlled use of sterile laboratory-bred maggots (Lucilia sericata) to clean chronic non-healing wounds. While common in human medicine, veterinary use is growing, particularly for wounds that fail conventional treatment.
What MDT Does
- Debridement - Larvae secrete proteolytic enzymes that digest necrotic tissue selectively, leaving healthy tissue intact
- Disinfection - Larvae consume bacteria (including MRSA and multidrug-resistant organisms) and secrete antimicrobial compounds
- Healing stimulation - Larval secretions promote granulation tissue and new blood vessel formation
MDT Success Rate in Veterinary Patients
According to a 2016 review published in Veterinary World, MDT achieved a 70-80% success rate in chronic wound treatment. In a 20-case series (7 small animals including 2 dogs, 4 cats, 1 rabbit; 13 horses), MDT was associated with limb salvage in 3 of 5 canines and felines that would otherwise have required amputation or euthanasia. No adverse events were attributed to MDT.
A 2025 case series (PMID 40081468) confirmed safety and efficacy of MDT for problematic wounds in cats and dogs in Mexico.
Dog Wound Healing with MDT - Before and After

Types of Wounds Treated with MDT in Veterinary Practice
- Chronic non-healing wounds post-surgery
- Diabetic foot/limb wounds
- Traumatic wounds with extensive necrosis
- Bite wounds with deep tissue infection
- Wounds with multidrug-resistant bacterial colonisation
- Ischemic wounds at amputation risk
Practical Challenges in Veterinary MDT
| Challenge | Solution |
|---|---|
| Animal removes/chews dressing | Use Elizabethan collar; sedation for dressing changes |
| Maggot containment | Secure cage dressing with chiffon/Dacron and bandaging |
| Animal discomfort | Larvae movement causes itching/irritation; analgesia helps |
| Maggot survival on arrival | Use within 24 hours; keep at room temperature until use |
| Owner acceptance | Educate about controlled, sterile nature of MDT maggots |
Common Sites of Maggot Infestation in Dogs
- Skin folds (facial, vulvar, tail, scrotal)
- Wounds and lacerations anywhere on the body
- Ears (especially dogs with chronic ear disease)
- Perineal region (soiled with feces/urine)
- Back and dorsum (recumbent dogs)
- Eyes and nasal cavities (in severe neglect cases)
Prevention
- Keep all wounds clean and covered
- Regular grooming - remove mats, keep coat dry and clean
- Treat underlying skin disease promptly
- Keep debilitated/mobility-impaired dogs indoors during fly season
- Screen enclosures for outdoor access
- Daily inspection of skin folds and wound sites in at-risk dogs
Sources: Clinician's Brief - Managing Maggots & Bots in Dogs & Cats | PMC - MDT as primary tool for chronic wounds in animals | PMID 40081468 - MDT case series dogs/cats, 2025 | PMID 16386439 - MDT in small animals survey | Pfenninger & Fowler's Procedures for Primary Care, 3rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.