I now have rich, comprehensive content from multiple authoritative textbooks and real CT images. Let me compile the complete, detailed response.
Radiology of Interstitial Lung Disease (ILD): A Complete Guide
Sources: Grainger & Allison's Diagnostic Radiology, Murray & Nadel's Textbook of Respiratory Medicine, Goldman-Cecil Medicine, Fishman's Pulmonary Diseases & Disorders
Part 1: Framework - How to Approach ILD Radiology
Imaging Modality Hierarchy
Chest X-ray (CXR) is the first step but is insensitive. It may be normal in up to 10% of ILD patients. Its main value is suggesting a category and assessing progression. It cannot replace HRCT.
High-Resolution CT (HRCT) is the gold standard. It:
- Increases diagnostic accuracy from 27% (clinical alone) to 61% when added to clinical data and CXR
- Distinguishes reversible (ground-glass, active inflammation) from irreversible (honeycombing, fibrosis) changes
- Guides bronchoalveolar lavage (BAL) and biopsy site selection
- Monitors treatment response
- In UIP/IPF, a typical pattern on HRCT can obviate surgical lung biopsy
Technical points: Use 1-mm thin sections. Prone images help distinguish posterior fibrosis from gravitational atelectasis. Expiratory images reveal air trapping (reflecting small airways disease).
Part 2: The HRCT Pattern Dictionary
Before going disease by disease, you must master these key HRCT patterns:
| Pattern | What it looks like | What it means |
|---|
| Ground-glass opacity (GGO) | Hazy increased density, vessels still visible | Active inflammation, usually reversible |
| Reticular pattern | Network of fine lines (intralobular septa) | Fibrosis, thickened septa |
| Honeycombing | Clustered thick-walled cysts (3-10mm), subpleural, stacked layers | Irreversible end-stage fibrosis (UIP hallmark) |
| Traction bronchiectasis | Dilated, irregular airways within fibrotic lung | Irreversible fibrosis pulling airways open |
| Consolidation | Complete airspace opacification, air bronchograms | Alveolar filling (COP, AIP, eosinophilic pneumonia) |
| Centrilobular nodules | Small nodules <5mm, not reaching pleura | Cellular bronchiolitis, HP, RB-ILD |
| Perilymphatic nodules | Along bronchovascular bundles, fissures, septa | Sarcoidosis, lymphangitic carcinomatosis |
| Mosaic attenuation | Geographic areas of different density | Air trapping, vascular disease, or infiltration |
| Air trapping (expiratory) | Areas stay dark on expiration | Small airways disease |
| Thin-walled cysts | Discrete cysts, no surrounding fibrosis | LAM, LCH, LIP |
Part 3: Idiopathic Interstitial Pneumonias (IIPs)
The ATS/ERS classification divides IIPs into several entities. Each has a characteristic CT signature.
1. Idiopathic Pulmonary Fibrosis (IPF) / Usual Interstitial Pneumonia (UIP)
IPF is the most common and most lethal IIP. The underlying pattern is UIP. HRCT is so characteristic it can often confirm the diagnosis without biopsy.
The 4 HRCT Categories (ATS/ERS/JRS/ALAT 2018 + Fleischner Society 2018):
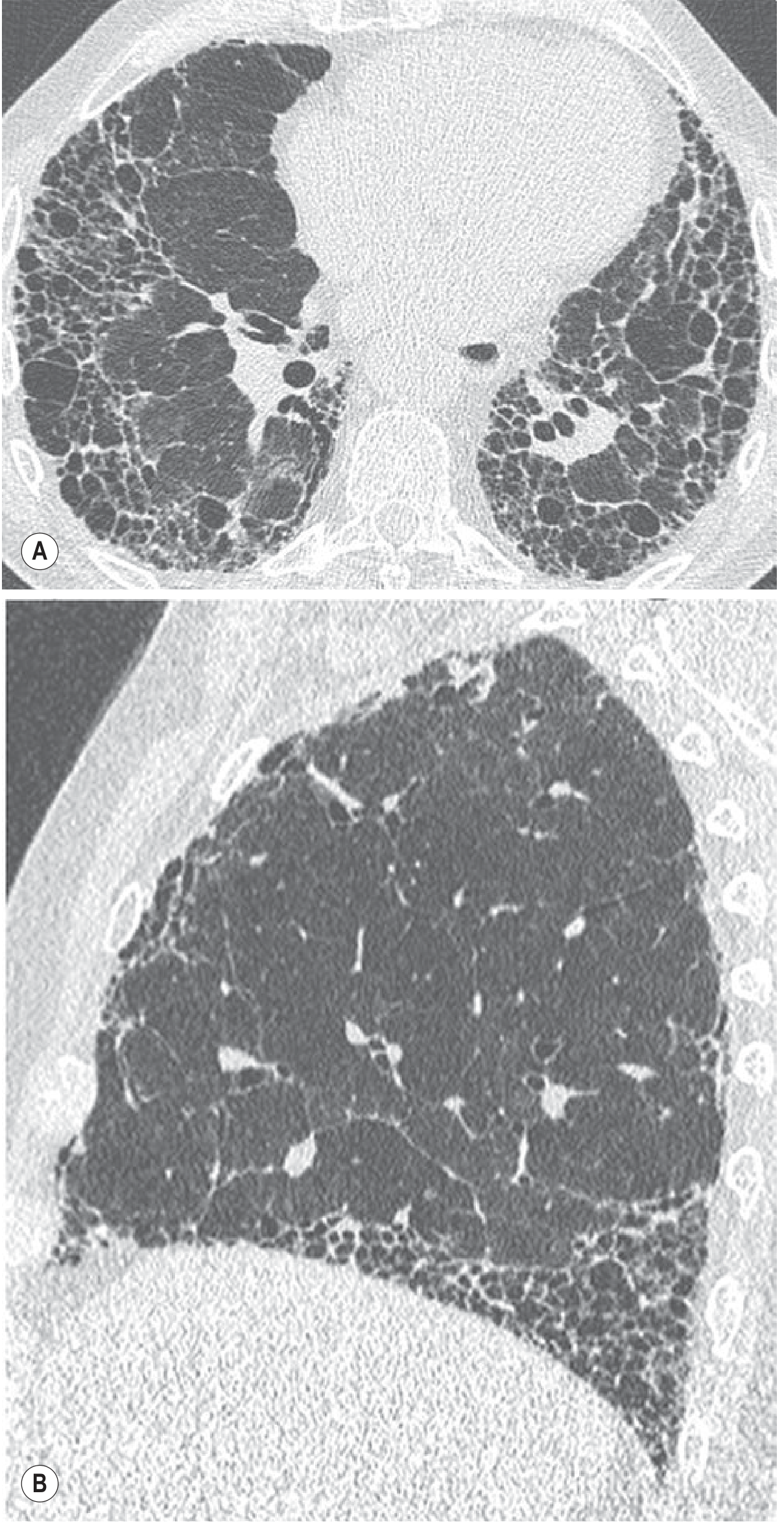
Typical UIP pattern - virtually pathognomonic for IPF:
- Predominantly subpleural, bibasal reticular pattern
- Honeycombing (thick-walled cysts in stacked layers)
- Traction bronchiectasis and bronchiolectasis
- The disease "creeps" up the periphery in a "propeller blade" distribution on sagittal images
- GGO is NOT dominant; when present, it is surrounded by traction bronchiectasis (indicating fibrosis, not activity)
- No features suggesting alternative diagnosis
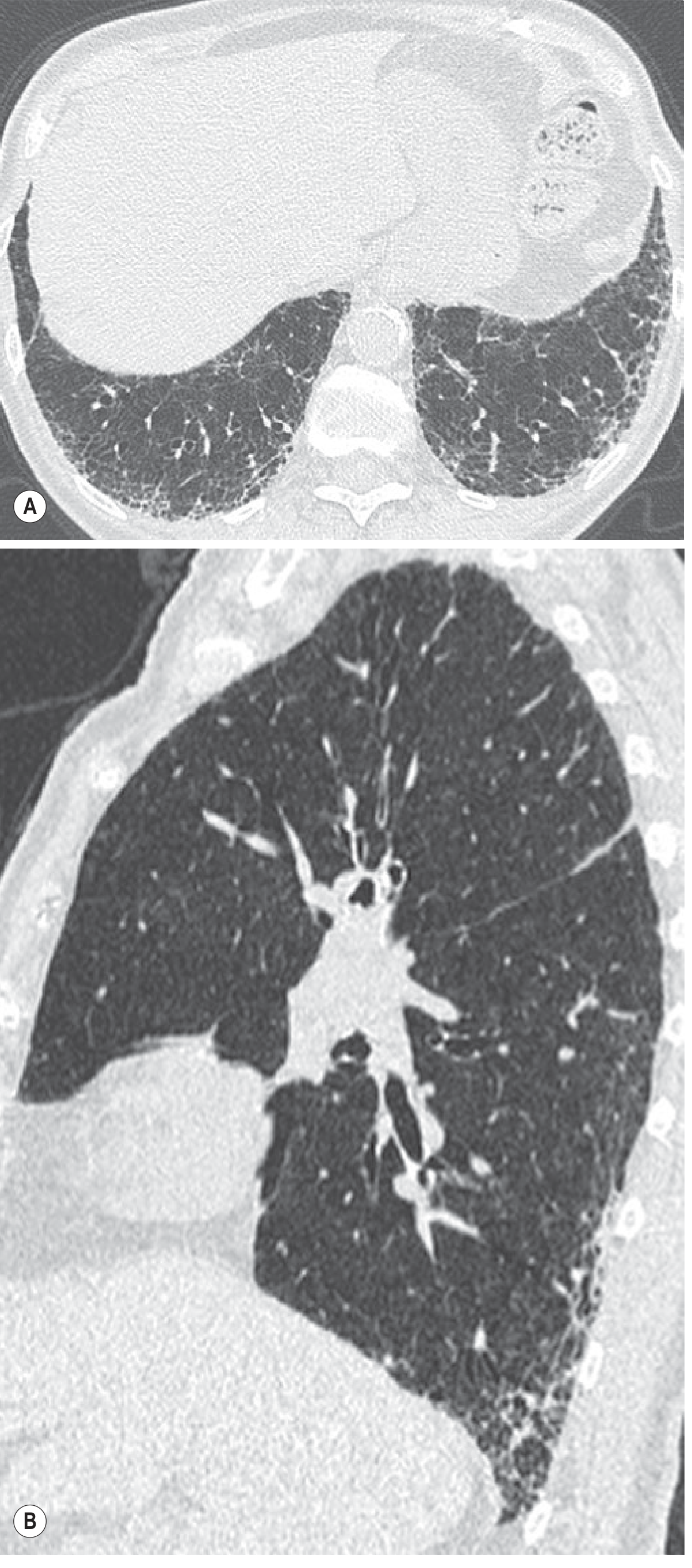
Probable UIP pattern (biopsy may still be avoided with right clinical context):
- Subpleural bibasal reticular pattern
- Peripheral traction bronchiectasis/bronchiolectasis
- No honeycombing
- Reflects definite/probable UIP pathology in 82-94% of cases
Indeterminate for UIP (requires biopsy):
- Subtle reticulation; may have mild GGO
- No distribution that fits typical/probable
- No features inconsistent with UIP
CT pattern inconsistent with UIP (alternative diagnosis):
- Upper or mid-lung predominant fibrosis
- Peribronchovascular predominance
- Extensive GGO (>extent of reticulation)
- Profuse micronodules, discrete cysts away from honeycombing zones
- Diffuse air trapping (mosaic pattern)
- Consolidation in bronchopulmonary segment/lobe
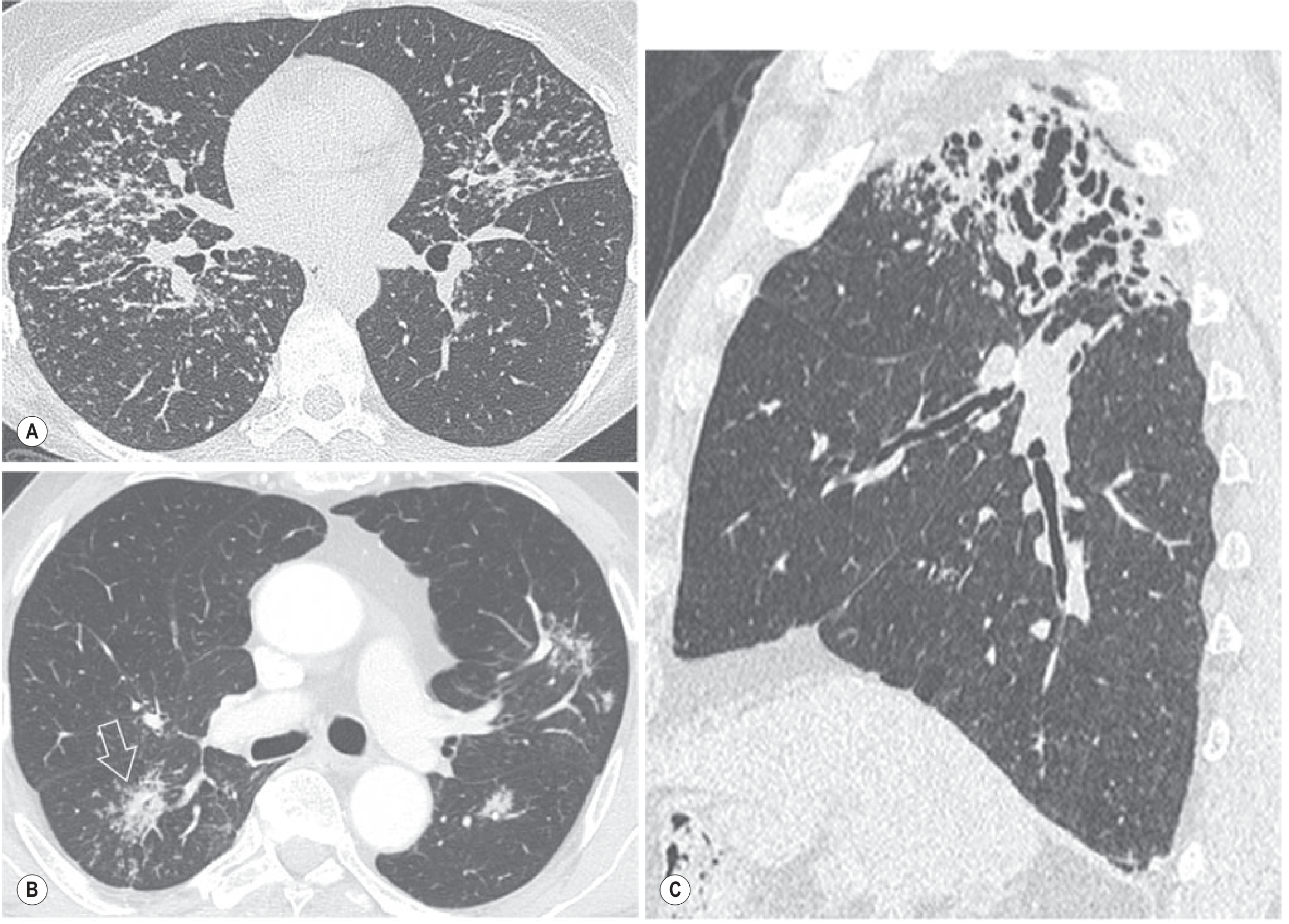
Fig. 9.1 - Typical UIP/IPF: axial HRCT showing subpleural honeycombing and reticular pattern at the lung bases with traction bronchiectasis; sagittal showing the "propeller blade" peripheral distribution creeping toward upper lobes.
Fig. 9.2 - Probable UIP: subpleural basal reticulation with peripheral traction bronchiolectasis, no honeycombing. Bronchiolectasis characteristically originates at the posterior costophrenic sulcus.
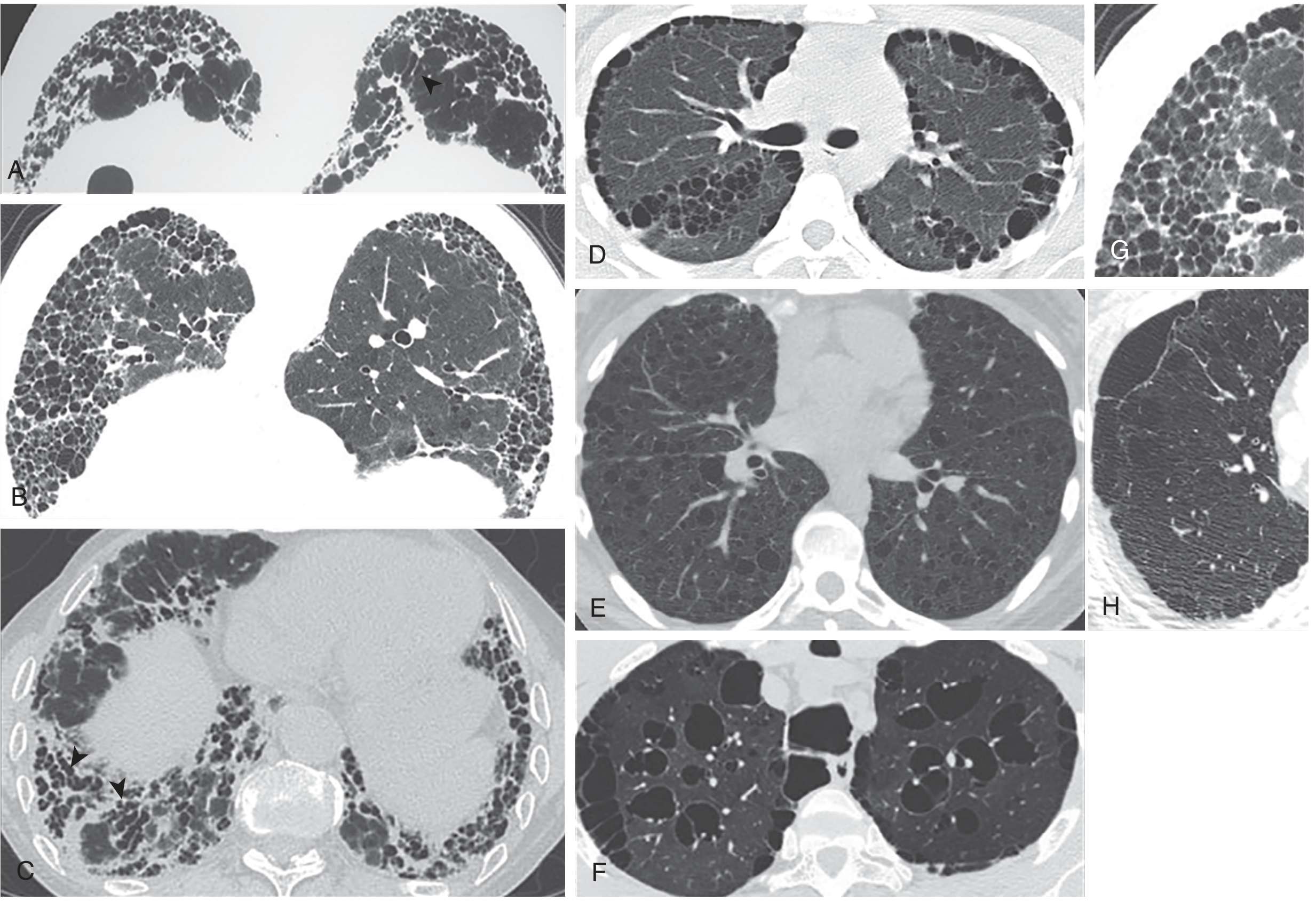
Honeycombing vs mimics - this is clinically critical:
Key distinguishing points:
- True honeycombing: thick-walled cysts, subpleural, stacked in layers, always with other fibrotic features (traction bronchiectasis, architectural distortion)
- Paraseptal emphysema: thin-walled, single layer subpleural, no fibrotic features
- LAM cysts: randomly scattered, normal lung between cysts, no subpleural predominance, no fibrosis
- Cystic bronchiectasis: centrally located, along vessels, tubular shape
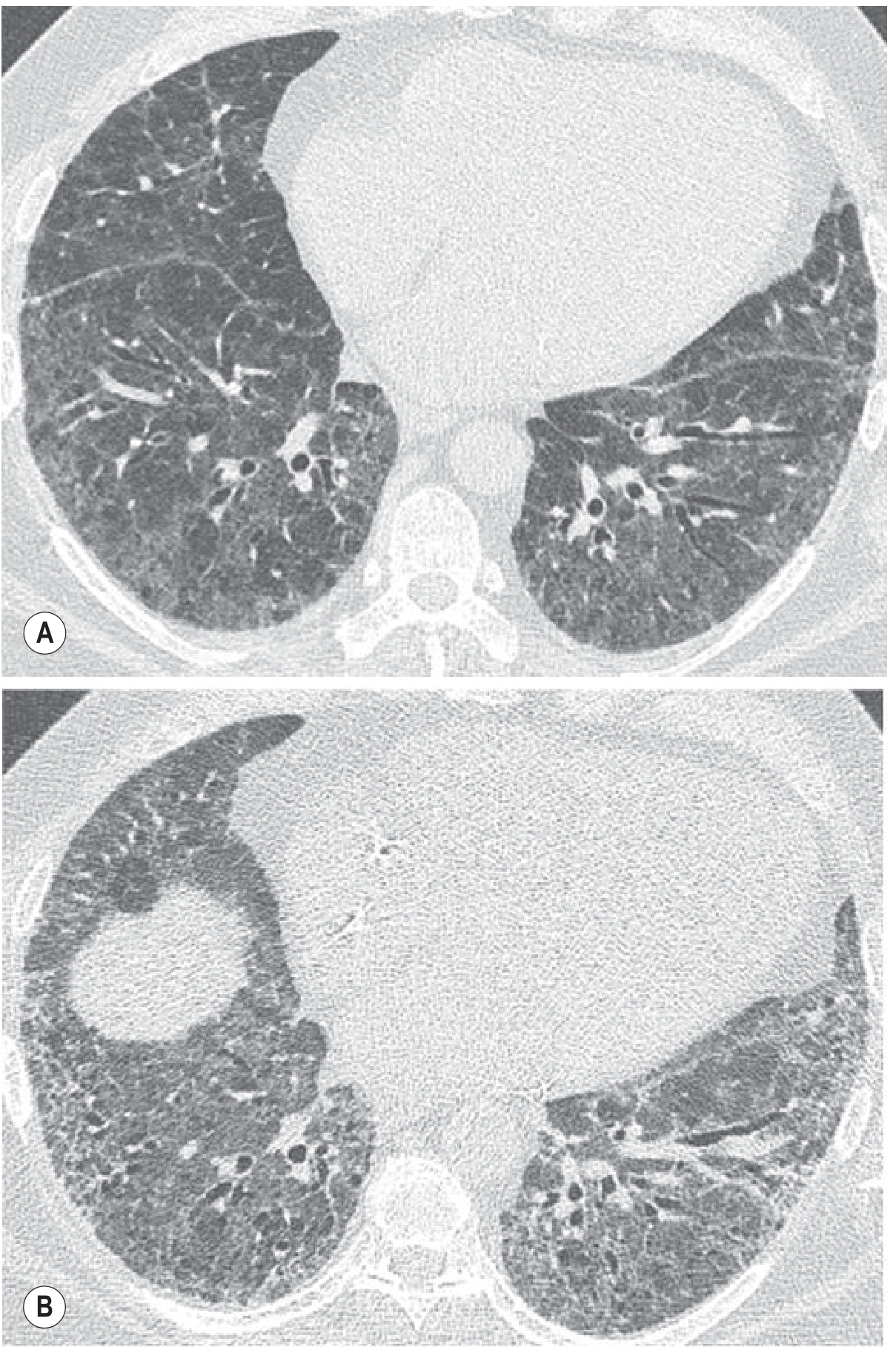
2. Nonspecific Interstitial Pneumonia (NSIP)
NSIP is the most common IIP pattern in connective tissue diseases (CTD). It has a better prognosis than IPF.
HRCT features:
- Bilateral symmetric ground-glass attenuation - the dominant finding
- Peripheral, subpleural, lower-lobe predominance
- Subpleural sparing - a characteristic and distinctive feature (unlike UIP)
- Irregular lines and mild reticulation
- Occasional consolidation
- Traction bronchiectasis when fibrotic NSIP
- Honeycombing rare (if present, indicates fibrotic NSIP, worse prognosis)
CXR: Bilateral ground-glass and reticular opacification, basal predominance.
Key distinction from UIP: NSIP shows more GGO and less honeycombing; subpleural sparing helps.
3. Cryptogenic Organizing Pneumonia (COP)
COP (formerly BOOP) has a distinctive CT pattern. It often responds well to corticosteroids, but lesions can recur.
HRCT features:
- Patchy bilateral consolidation - most characteristic
- Distribution: subpleural or peribronchial (peribronchovascular)
- Air bronchograms within consolidation
- Lower lobe predominance
- "Reversed halo sign" (atoll sign): crescent or ring of consolidation around central GGO - highly specific for COP
- Perilobular pattern: band-like consolidation along lobular borders
- Migration of lesions over time ("migratory infiltrates")
- GGO with traction bronchiectasis may be present in fibrotic COP
CXR: Bilateral patchy consolidation, may be fleeting/migratory on serial films.
4. Acute Interstitial Pneumonia (AIP) / Diffuse Alveolar Damage (DAD)
AIP is the idiopathic form of ARDS. It is histologically DAD and clinically presents as rapidly progressive respiratory failure.
HRCT features (evolve through phases):
- Exudative phase (days 1-7): Bilateral diffuse GGO and consolidation, often with lobular sparing (geographic distribution)
- Organizing phase (weeks 2-4): Traction bronchiectasis develops within GGO (hallmark of transition to fibrosis)
- Dependent consolidation common
- Anterior-posterior density gradient (dependent vs. non-dependent)
- Architectural distortion in fibrotic phase
CXR: Bilateral diffuse ground-glass density or consolidation (similar to cardiogenic pulmonary edema).
5. Respiratory Bronchiolitis-ILD (RB-ILD)
Strongly associated with heavy cigarette smoking. Often an incidental finding.
HRCT features:
- Diffuse, patchy ground-glass opacification due to macrophage accumulation
- Poorly defined centrilobular nodules (fluffy, low-attenuation)
- Upper lobe predominance (bilateral, symmetric)
- Centrilobular emphysema (related to smoking)
- Areas of air trapping
- Interlobular septal thickening and interstitial fibrosis may occur but are not dominant
- Normal CXR in up to 20% of RB-ILD patients
6. Desquamative Interstitial Pneumonia (DIP)
Also smoking-related. More extensive macrophage accumulation than RB-ILD.
HRCT features:
- Extensive ground-glass opacification - dominant feature
- Distribution: lower zone, peripheral, may be patchy or geographic
- Associated reticulation (mild)
- Small cysts may be present within GGO
- Features of established fibrosis (architectural distortion, mild bronchiectasis) in some patients
- Normal CXR in up to 25% of cases
DIP vs RB-ILD: DIP has more extensive GGO (often bilateral and diffuse), while RB-ILD has centrilobular nodules with more upper lobe distribution.
7. Lymphoid Interstitial Pneumonia (LIP)
Associated with Sjögren syndrome, HIV, and immunodeficiency states.
HRCT features:
- Diffuse GGO (dominant)
- Thin-walled cysts (scattered, often bilateral) - highly characteristic
- Centrilobular nodules
- Thickened interlobular septa and bronchovascular wall thickening
- Lower lobe predominance
Key feature: The combination of GGO + scattered thin-walled cysts in the right clinical context (Sjögren, HIV) is strongly suggestive.
Part 4: Non-Idiopathic ILD
8. Sarcoidosis
Sarcoidosis is the archetypal perilymphatic nodular disease.
CXR Staging (Scadding):
- Stage 0: Normal
- Stage I: Bilateral hilar lymphadenopathy (BHL) only
- Stage II: BHL + parenchymal infiltrates
- Stage III: Parenchymal infiltrates only (no BHL)
- Stage IV: Pulmonary fibrosis
Note: Parenchymal changes often appear as BHL is subsiding (unlike lymphoma where they progress together).
HRCT features:
- Perilymphatic nodules (1-5mm) - along bronchovascular bundles, pleura (including fissures), and interlobular septa - this distribution is the key
- "Galaxy sign": smaller nodules cluster around a large central nodule - highly specific for sarcoidosis
- Irregular and beaded interfaces
- Larger ill-defined nodules ± air bronchograms
- Patchy GGO
- Interlobular septal thickening
- Air trapping - correlates with small airways disease on PFTs
- Advanced disease: upper/mid-zone fibrosis, traction bronchiectasis, bullae, ring shadowing
- Progressive massive fibrosis (PMF) - resembling silicosis - in end-stage
Distribution: Mid and upper lobe predominance (bilateral); perihilar in advanced fibrotic disease.
9. Hypersensitivity Pneumonitis (HP)
Three phases: acute, subacute, chronic. Radiology differs by phase.
Acute HP:
- Bilateral GGO and consolidation
- Often resolves spontaneously on antigen removal
Subacute HP (classic HRCT pattern):
- Diffuse poorly defined centrilobular nodules (3-5mm)
- Patchy bilateral GGO
- Air trapping on expiratory CT (lobular or panlobular) - very characteristic
- Mosaic perfusion - areas of normal and reduced attenuation
- Mid and upper lobe predominance
- Head-cheese sign: combination of GGO, normal lung, and air trapping creating three different densities
Chronic HP (fibrotic):
- Reticulation and fibrosis
- Upper/mid lobe predominance (differs from IPF which is lower lobe)
- Traction bronchiectasis
- May develop honeycombing - can mimic UIP
- Peribronchovascular distribution (not purely subpleural like UIP)
- GGO and centrilobular nodules often persist alongside fibrosis (important clue)
CXR: Bilateral GGO and consolidation (acute/subacute); reticulonodular, upper lobe fibrosis (chronic).
10. Connective Tissue Disease-ILD (CTD-ILD)
Most CTDs can cause ILD; they most commonly produce NSIP or UIP patterns.
Rheumatoid Arthritis (RA-ILD):
- Most common pattern: UIP (more than NSIP, unlike other CTDs)
- HRCT indistinguishable from idiopathic UIP/IPF
- Also: bronchiectasis (up to 30%), obliterative bronchiolitis, follicular bronchiolitis, COP pattern, pleural effusions
- Necrobiotic (rheumatoid) nodules: well-defined, peripheral, may cavitate
Systemic Sclerosis (SSc/Scleroderma):
- Most common ILD pattern: fibrotic NSIP
- Subpleural basal GGO with reticulation, subpleural sparing
- Dilated esophagus on HRCT - a helpful diagnostic clue
- Pulmonary hypertension disproportionate to fibrosis extent
Polymyositis/Dermatomyositis (PM/DM):
- Mixed pattern: GGO, reticular, consolidation
- Both NSIP and COP patterns occur
- "Mechanic's hands," elevated CK, anti-Jo-1 in some
Sjögren Syndrome:
- LIP pattern (GGO + thin-walled cysts)
- Also: follicular bronchiolitis, NSIP
SLE:
- Acute lupus pneumonitis (bilateral GGO/consolidation)
- Pleuritis/effusions common
- Shrinking lung syndrome: small lung volumes, elevated diaphragm
11. Langerhans Cell Histiocytosis (LCH / PLCH)
Almost exclusively in smokers. Distinctive cystic pattern.
HRCT features:
- Upper and mid-lung predominance (spares costophrenic angles)
- Bilateral irregular/bizarre-shaped cysts - key feature; cysts vary in size and shape (not all round)
- Centrilobular nodules (early disease) that cavitate and form cysts (later)
- Normal lung volumes or hyperinflation
- Pneumothorax is a recognized complication
Evolution: nodules (early) → cavitating nodules → cysts (late)
12. Lymphangioleiomyomatosis (LAM)
Occurs almost exclusively in women of childbearing age. Associated with tuberous sclerosis.
HRCT features:
- Bilateral, diffuse, thin-walled, round cysts - uniformly distributed throughout the lung
- Normal lung intervening between cysts (unlike UIP honeycombing)
- No subpleural predominance
- No fibrosis
- Cysts increase in number/size over time
- Pleural effusion (chylothorax) may occur
- Pneumothorax common
Key distinction from UIP honeycombing: LAM cysts are round, thin-walled, uniformly distributed, with no surrounding fibrosis.
13. Asbestosis
Occupational ILD from asbestos exposure (>10 year latency). Pattern mirrors UIP.
HRCT features:
- Bilateral lower-lobe fibrosis - subpleural, basal (similar to UIP)
- Reticular pattern, traction bronchiectasis, honeycombing in advanced disease
- Subpleural dots and lines - early characteristic finding
- Pleural plaques - calcified or non-calcified, diaphragmatic/posterolateral
- Pleural thickening (diffuse)
- Rounded atelectasis ("crow's feet" - curvilinear bands converging on pleura)
The combination of lower lobe fibrosis + pleural plaques strongly suggests asbestosis.
14. Silicosis / Coal Worker's Pneumoconiosis (CWP)
Simple silicosis:
- Upper lobe nodules (1-10mm) - bilateral, well-defined
- Perilymphatic distribution (like sarcoidosis)
- Eggshell calcification of hilar/mediastinal nodes (pathognomonic)
Progressive Massive Fibrosis (PMF):
- Conglomerate masses (>1cm, usually >2cm) in upper lobes
- "Egg-in-a-cup" or PMF masses migrating toward hilum
- Associated emphysema
15. Eosinophilic Pneumonia (Chronic)
HRCT features:
- Peripheral consolidation and GGO - "photographic negative of pulmonary edema"
- Upper/mid-lung zone predominance with peripheral distribution
- Recurrent or migratory lesions (unlike most ILDs)
- Air bronchograms within consolidation
- Pleural effusion in ~10%
16. Drug-Induced ILD
Highly variable patterns - virtually any ILD pattern can be drug-induced. Common patterns:
- Amiodarone: high-density consolidation (due to iodine in drug), peripheral GGO, NSIP pattern
- Methotrexate: hypersensitivity pattern, GGO, consolidation
- Chemotherapy (bleomycin, cyclophosphamide): COP pattern, NSIP pattern
- Nitrofurantoin: pleural effusion + parenchymal infiltrates
Part 5: Chest X-Ray Pattern → Differential Diagnosis
(From Goldman-Cecil Medicine, Table 80-3)
| CXR Finding | Key Diagnoses |
|---|
| Decreased lung volumes | IPF, NSIP, DIP, CTD-ILD, asbestosis, drug-ILD |
| Preserved/increased volumes | IPF+emphysema, LCH, LAM, sarcoidosis, HP, RB-ILD |
| Micronodules | HP, sarcoidosis, RB-ILD, infection |
| Honeycombing | IPF, fibrotic NSIP, CTD-ILD, asbestosis, chronic HP |
| Migratory/fleeting infiltrates | COP, HP, eosinophilic, ABPA |
| Upper lobe predominance | Sarcoidosis, HP, LCH, silicosis, ankylosing spondylitis |
| Lower lobe predominance | IPF, NSIP, CTD-ILD, asbestosis |
| Peripheral distribution | IPF, NSIP, COP, chronic eosinophilic pneumonia |
| Pleural disease | CTD, asbestosis, malignancy, LAM, sarcoidosis |
| Pneumothorax | LCH, LAM, tuberous sclerosis |
| Hilar adenopathy | Sarcoidosis, silicosis, LIP, malignancy |
| Normal CXR | Cellular NSIP, RB-ILD, HP, sarcoidosis (up to 10%) |
Part 6: Diagnostic Approach Summary
Step 1: Clinical context
- Age, sex, smoking history, occupation, drug history, CTD symptoms
- Pace of onset (acute, subacute, chronic)
Step 2: CXR
- Lung volumes (decreased vs preserved)
- Distribution (upper/lower, central/peripheral)
- Pattern (nodular, reticular, consolidation, mixed)
- Pleural changes, adenopathy
Step 3: HRCT (1mm, prone and expiratory views)
- Classify dominant pattern (GGO, reticular, honeycomb, nodular, consolidation, cystic)
- Assess distribution (upper/lower, central/peripheral/subpleural, axial)
- Look for specific signs (perilymphatic nodules, galaxy sign, reversed halo, subpleural sparing)
Step 4: Multidisciplinary Discussion
- Radiologist + Pulmonologist + Pathologist
- Correlate with serology, BAL, PFTs
- Decide if biopsy is needed or if HRCT pattern is diagnostic
Step 5: Biopsy (if needed)
- Site guided by HRCT (most active disease, avoid honeycombing/end-stage areas)
Quick Reference: ILD Pattern on HRCT
| ILD Type | Dominant CT Pattern | Distribution | Key Feature |
|---|
| IPF/UIP | Reticular + honeycombing | Subpleural, bibasal | Propeller blade; no GGO dominance |
| NSIP | GGO + reticulation | Subpleural, lower | Subpleural sparing |
| COP | Consolidation | Subpleural/peribronchial | Reversed halo sign; migrating |
| AIP | GGO + consolidation | Diffuse, bilateral | Lobular sparing; rapid progression |
| RB-ILD | Centrilobular GGO nodules | Upper lobe, bilateral | Heavy smoker; subtle |
| DIP | Extensive GGO | Lower lobe, peripheral | Diffuse; smoker |
| LIP | GGO + cysts | Lower lobe | Thin-walled cysts; Sjögren/HIV |
| Sarcoidosis | Perilymphatic nodules | Upper/mid lobe, perihilar | Galaxy sign; BHL |
| HP (subacute) | GGO + centrilobular nodules + air trapping | Upper/mid lobe | Head-cheese sign; mosaic |
| LAM | Thin-walled cysts | Diffuse, uniform | Young women; no fibrosis |
| LCH | Nodules → bizarre cysts | Upper/mid, spares bases | Smokers; irregular cysts |
| Asbestosis | Reticular + pleural plaques | Lower lobe, subpleural | Pleural plaques = clue |
| Silicosis | Upper lobe nodules | Upper lobe | Eggshell calcification |
| Chronic eosinophilic | Peripheral consolidation | Upper/mid, peripheral | "Photographic negative of edema" |
Sources: Grainger & Allison's Diagnostic Radiology (9780323760751); Murray & Nadel's Textbook of Respiratory Medicine (9780323655873); Goldman-Cecil Medicine (9780323930345); Fishman's Pulmonary Diseases and Disorders (9781260473940)