Latest guidelines for management of hypertension in pregnancy
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "pregnancy" AND "management"
Searching the Web
hypertension in pregnancy guidelines 2024 2025 ACOG ISSHP management
Reading File
Reading File
Searching PubMed
"hypertensive disorders of pregnancy" AND "guidelines" AND "treatment"
Searching the Web
ACOG practice bulletin hypertension pregnancy 2024 antihypertensive treatment targets
Reading File
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12998458
Finding Sources
Reading File
Searching PubMed
"CHAP trial" OR "chronic hypertension pregnancy" AND "antihypertensive" AND "outcomes"
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have sufficient information to compose a comprehensive, authoritative answer. Here it is:
Management of Hypertension in Pregnancy
Hypertension complicates more than 10% of pregnancies in the United States and is a leading cause of maternal and perinatal morbidity worldwide. The following covers classification, diagnosis, prevention, pharmacological management, and delivery timing, synthesized from current authoritative sources (ACOG, ESC 2024, ISSHP 2021, Harrison's 2025, Creasy & Resnik MFM, Brenner & Rector's Kidney).
1. Classification
| Category | Definition |
|---|---|
| Chronic hypertension | BP ≥140/90 mmHg before pregnancy or before 20 weeks gestation; persists >12 weeks postpartum |
| Gestational hypertension | New-onset SBP ≥140 or DBP ≥90 mmHg after 20 weeks without proteinuria or end-organ damage |
| Preeclampsia | New-onset hypertension after 20 weeks WITH proteinuria (≥300 mg/24h) OR end-organ dysfunction (see below) |
| Preeclampsia with severe features | SBP ≥160 or DBP ≥110 mmHg on two occasions; thrombocytopenia <100,000/µL; liver enzymes ≥2× ULN; creatinine ≥1.1 mg/dL or doubling of baseline; pulmonary edema; new-onset severe headache or visual disturbance |
| Eclampsia | Preeclampsia + new-onset generalized seizures |
| HELLP syndrome | Hemolysis + Elevated Liver enzymes + Low Platelets - a severe form of preeclampsia |
| Superimposed preeclampsia | Chronic hypertension with new or worsening proteinuria, or new end-organ features |
Note: Proteinuria is no longer required for preeclampsia diagnosis if other end-organ manifestations are present. This was a key update from the 2013 ACOG Task Force.
2. Blood Pressure Measurement
- Use the right arm with the patient seated and at rest for ≥5 minutes.
- Hypertension is confirmed on two readings ≥15 minutes apart.
- Severe hypertension = SBP ≥160 mmHg or DBP ≥110 mmHg (requires treatment within 30-60 minutes).
- Home BP monitoring and ambulatory monitoring are increasingly recommended to detect white-coat hypertension (office ≥140/90 but home <135/85) and masked hypertension.
3. Prevention
Low-Dose Aspirin
- Recommended for high-risk women starting at 12-16 weeks gestation (some guidelines recommend before 16 weeks).
- Dose: 75-150 mg/day (ACOG recommends 81 mg daily).
- High-risk indications: prior preeclampsia, chronic hypertension, diabetes (type 1 or 2), renal disease, autoimmune disease (SLE, antiphospholipid syndrome), multifetal gestation.
- Meta-analyses show aspirin reduces preeclampsia risk by ~10-20%; benefit is greater when initiated before 16 weeks and at higher doses (>100 mg).
Calcium supplementation
- 1.5-2 g/day elemental calcium recommended in populations with low dietary calcium intake - reduces preeclampsia risk.
Non-pharmacological
- Moderate exercise, weight management, salt restriction (though aggressive restriction is not recommended in pregnancy).
- Screening for obstructive sleep apnea in obese women or those with snoring (OSA present in ~40% of women with hypertension in pregnancy).
4. Treatment Thresholds and BP Targets
This is the area of most recent guideline evolution:
| Severity | Threshold for Treatment | Target BP |
|---|---|---|
| Mild-moderate (140-159/90-109 mmHg) | Debated (see below) | 130-150/80-100 mmHg |
| Severe (≥160/110 mmHg) | Mandatory - treat within 30-60 min | 140-150/90-100 mmHg (acute) |
Key Guideline Differences on Mild Hypertension:
- ACOG (2020, re-affirmed 2024): Does not require antihypertensive treatment for preeclampsia patients with mild gestational hypertension and no end-organ damage.
- ESC (2024): Recommends initiating antihypertensive therapy for all women with sustained BP ≥140/90 mmHg.
- ISSHP (2021): Recommends treatment for all women with BP ≥140/90 mmHg.
The CHAP Trial (2022) - Practice-Changing Evidence
The Chronic Hypertension and Pregnancy (CHAP) trial showed that treating mild chronic hypertension (BP 140-159/90-109 mmHg) to a target <140/90 mmHg significantly reduced the composite outcome of severe hypertension, preterm birth <35 weeks, placental abruption, and perinatal death (odds ratio ~0.82), without increasing risk of small-for-gestational-age infants. This prompted ACOG to issue a practice advisory (April 2022, re-affirmed 2024) recommending antihypertensive treatment for mild chronic hypertension in pregnancy to a target of <140/90 mmHg.
The earlier CHIPS trial also showed tight BP control (DBP target 85 mmHg) reduced severe hypertension and maternal complications vs. less-tight control (DBP 100 mmHg), without adverse fetal effects. - Brenner and Rector's Kidney, Table 48.5
5. Pharmacological Management
First-Line Oral Antihypertensives (Chronic/Gestational Hypertension)
| Drug | Dose | Notes |
|---|---|---|
| Labetalol | 100-200 mg PO BID-TID (max 2400 mg/day) | Alpha + beta blocker; most commonly used; avoid in asthma, CHF |
| Nifedipine (extended-release) | 30-60 mg PO once daily | Ca²+ channel blocker; safe; now preferred over methyldopa by many |
| Methyldopa | 250-500 mg PO BID-TID | Central α2-agonist; extensive safety data; less effective for severe HTN; interferes with iron absorption; less commonly preferred now |
- Second-line: Other beta-blockers (metoprolol, propranolol), amlodipine, hydralazine (oral).
- Atenolol: Avoid - associated with fetal growth restriction.
- Diuretics: Generally avoided (reduce plasma volume in preeclampsia); may be continued if patient was on them pre-pregnancy for chronic hypertension.
Contraindicated in Pregnancy
- ACE inhibitors (captopril, enalapril, lisinopril, etc.) - fetal renal toxicity, oligohydramnios, skull hypoplasia, death
- Angiotensin receptor blockers (ARBs) - same as ACEi
- Renin inhibitors (aliskiren)
- Mineralocorticoid antagonists (spironolactone) - theoretical risk of feminization of male fetus; eplerenone may be an alternative when needed
Acute/Severe Hypertension (≥160/110 mmHg) - Treat Within 30-60 Minutes
| Drug | Dose/Route | Notes |
|---|---|---|
| IV Labetalol | 20 mg IV; escalate to 40 mg, then 80 mg q10 min; max 300 mg | First-line IV option |
| Oral Nifedipine (IR) | 10-20 mg PO; repeat in 20-30 min if needed | Effective even without IV access; do NOT use sublingual route |
| IV Hydralazine | 5-10 mg IV q20 min | Traditional option; more reflex tachycardia |
| IV Nicardipine | 5-15 mg/h infusion | Used in ICU settings |
| IV Sodium nitroprusside | Last resort; cyanide toxicity risk; avoid prolonged use |
- Goal: Reduce BP to <160/110 mmHg within 1 hour, then stabilize at 140-150/90-100 mmHg.
- Avoid excessive reduction - risk of uteroplacental hypoperfusion.
- No significant difference in efficacy or safety between labetalol, hydralazine, and nifedipine for acute severe hypertension. - ACOG Practice Bulletin #203
6. Seizure Prophylaxis with Magnesium Sulfate
- Indicated for: Preeclampsia with severe features, eclampsia, and postpartum women with CNS symptoms.
- Not routinely recommended for preeclampsia without severe features (ACOG).
- Regimen: 4-6 g IV loading dose over 15-20 minutes, then 1-2 g/h IV maintenance.
- Continue for 24-48 hours postpartum.
- ~20% of eclampsia episodes occur >48h postpartum - maintain vigilance.
- Monitor: urine output, reflexes, respiratory rate, serum magnesium levels (therapeutic: 4-7 mEq/L).
- Antidote: Calcium gluconate 1 g IV for magnesium toxicity.
- Magnesium is superior to phenytoin and diazepam for seizure prophylaxis. - Creasy & Resnik MFM
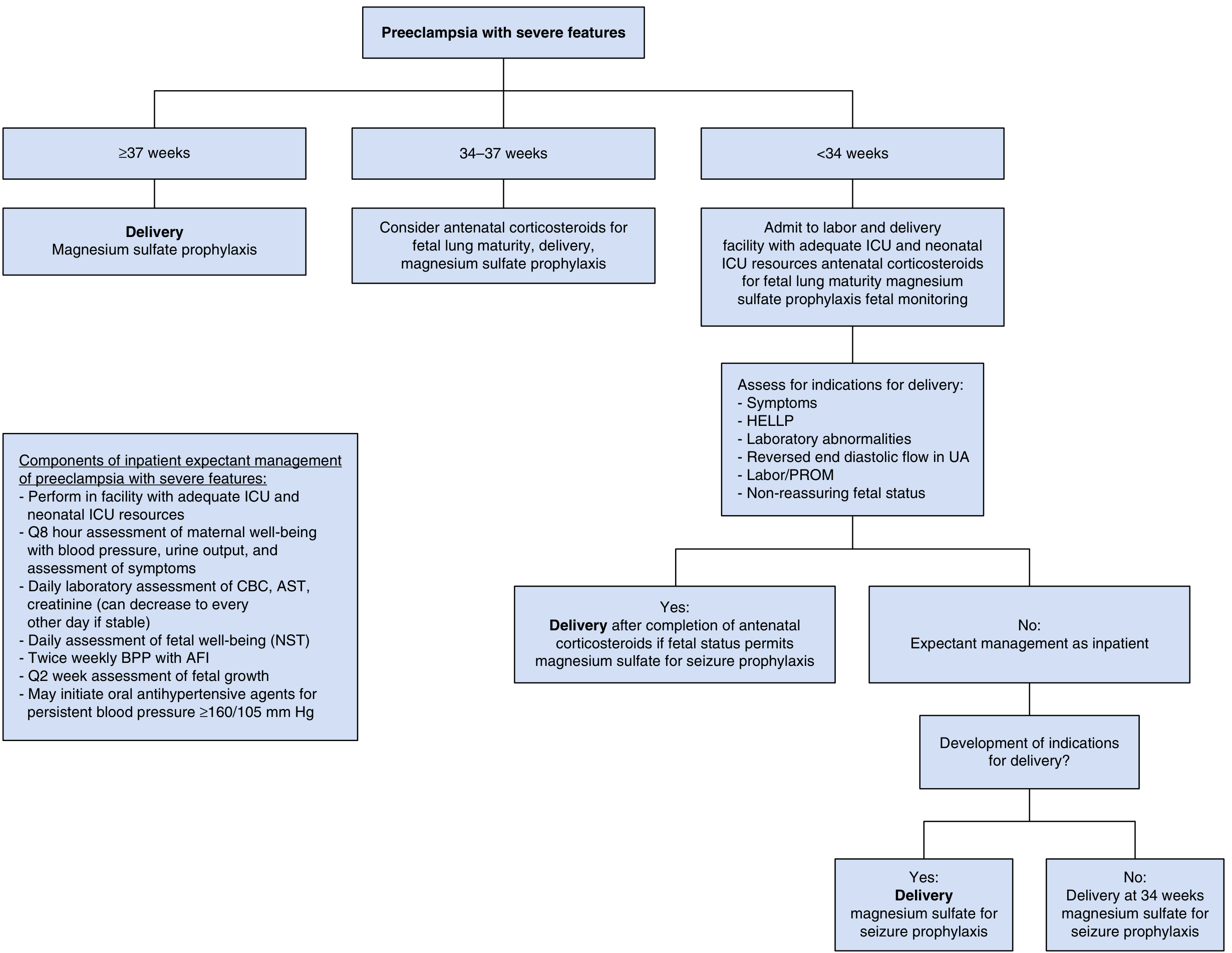
7. Delivery Timing
Delivery is the definitive treatment for preeclampsia.
| Condition | Gestational Age | Management |
|---|---|---|
| Preeclampsia without severe features | ≥37 weeks | Prompt delivery |
| Preeclampsia without severe features | <37 weeks | Expectant management with close monitoring (weekly labs, twice-weekly antenatal testing) |
| Preeclampsia with severe features | ≥37 weeks | Prompt delivery with MgSO₄ prophylaxis |
| Preeclampsia with severe features | 34-37 weeks | Antenatal corticosteroids for fetal lung maturity, then delivery |
| Preeclampsia with severe features | <34 weeks | Admit to facility with ICU/NICU; antenatal corticosteroids; expectant management if no indications for delivery; deliver at 34 weeks if stable |
| Gestational hypertension | 37-38 weeks | Deliver |
| Chronic hypertension (controlled on meds) | 36 weeks or 39-39⁶⁄₇ weeks | Antenatal surveillance from 36 weeks; deliver by 39⁶⁄₇ weeks |
8. Postpartum Management
- BP often initially falls after delivery but can surge again at 3-5 days postpartum (fluid remobilization).
- Continue/initiate antihypertensives for BP ≥150/100 mmHg postpartum.
- MgSO₄ prophylaxis should continue for 24-48 hours postpartum in severe preeclampsia/eclampsia.
- Safe for breastfeeding: Labetalol, nifedipine, methyldopa, enalapril (ACEi acceptable postpartum), captopril.
- Avoid NSAIDs in women with severe hypertension or renal impairment (can worsen BP).
- Screen for long-term cardiovascular risk - women with preeclampsia have 2-4x higher lifetime risk of cardiovascular disease.
- BP usually normalizes within 6-12 weeks postpartum; persistent hypertension requires workup for secondary causes.
9. Special Considerations
HELLP Syndrome
- Manage as preeclampsia with severe features.
- Platelet transfusion if <20,000/µL or active bleeding.
- Corticosteroids (dexamethasone) may improve platelet count, though evidence for improving overall outcomes is limited.
- Delivery is generally required.
Chronic Hypertension - Preconception Counseling
- Switch to pregnancy-safe medications before conception (discontinue ACEi/ARBs).
- Evaluate for secondary causes of hypertension.
- Counsel regarding risk of superimposed preeclampsia (15-25% in chronic HTN), preterm birth, IUGR.
Fetal Surveillance
- Chronic HTN on medication: Antenatal surveillance from ~36 weeks, growth scans every 3-4 weeks from 28-32 weeks.
- Gestational HTN/preeclampsia: Weekly NST or BPP, growth scan every 3 weeks.
Key Guideline Sources
- ACOG Practice Bulletin #203 (Chronic Hypertension in Pregnancy, 2019, re-affirmed 2024)
- ACOG Practice Bulletin #222 (Gestational Hypertension and Preeclampsia, 2020, re-affirmed 2023)
- ACOG Practice Advisory on CHAP trial (April 2022, re-affirmed 2024) - recommends treating mild chronic HTN to <140/90 mmHg
- ISSHP 2021 - recommends treatment for BP ≥140/90 mmHg in all hypertensive disorders of pregnancy
- ESC 2024 - recommends antihypertensive therapy at sustained BP ≥140/90 mmHg
- USPSTF - recommends low-dose aspirin for high-risk women from 12-16 weeks
Sources: Harrison's Principles of Internal Medicine 22E (2025); Creasy & Resnik's Maternal-Fetal Medicine (Principles and Practice); Brenner and Rector's The Kidney; Fuster and Hurst's The Heart, 15th Ed.; Goodman & Gilman's Pharmacological Basis of Therapeutics; ACOG Practice Bulletins #203 and #222; ESC 2024 Guidelines on Elevated Blood Pressure.
This is a shared conversation. Sign in to Orris to start your own chat.