Give a case scenario for Gall stones and cholecystitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks to construct a detailed, realistic clinical case. Here it is:
Clinical Case: Gallstones and Acute Cholecystitis
Case Presentation
Patient: Mrs. Anita Sharma, 42-year-old woman
BMI: 31 kg/m² | Parity: G3P3 | Past medical history: Type 2 diabetes mellitus (diet-controlled), no prior surgeries
Chief Complaint
"Severe pain in my upper right abdomen for the past 8 hours - it won't go away."
History of Present Illness
Mrs. Sharma presents to the Emergency Department at 11 PM with an 8-hour history of constant, severe right upper quadrant (RUQ) pain radiating to the right shoulder and back. She describes having experienced 3-4 similar but shorter episodes over the past 6 months - each lasting 1-2 hours and resolving on its own, typically after eating fatty food (fried rice, mutton curry). Tonight's episode started after dinner and has progressively worsened rather than resolving.
She also reports:
- Nausea and two episodes of vomiting (non-bilious)
- Low-grade fever (she feels warm)
- No jaundice, dark urine, or pale stools
- No diarrhoea or dysuria
She denies any previous diagnosis of gallstones, though she recalls being told her liver "looked a little fatty" on a scan 2 years ago.
Risk factors present (the "5 F's"):
- Fat - BMI 31 (overweight)
- Female - 42-year-old woman
- Fertile - 3 pregnancies (elevated estrogen promotes cholesterol supersaturation in bile)
- Forty - age in the fourth decade
- Family - her mother had a cholecystectomy at age 50
Physical Examination
| Parameter | Finding |
|---|---|
| Temperature | 38.2°C |
| HR | 98 bpm |
| BP | 124/78 mmHg |
| RR | 18/min |
| SpO₂ | 98% on room air |
Abdomen:
- Soft, with voluntary guarding in the RUQ
- No rigidity or rebound tenderness
- Murphy's sign: POSITIVE - deep palpation of the RUQ causes sharp pain and sudden cessation of inspiration. Murphy's sign is 65% sensitive and 87% specific for acute cholecystitis.
- No palpable gallbladder mass (Courvoisier's sign negative)
- Bowel sounds present and normal
- No jaundice, no scleral icterus
Differential Diagnosis
| Diagnosis | For | Against |
|---|---|---|
| Acute cholecystitis | Positive Murphy's, fever, persistent RUQ pain, prior biliary colic episodes | - |
| Biliary colic | Prior similar episodes | This episode >6 hours, fever, Murphy's sign |
| Choledocholithiasis | RUQ pain, history of stones | No jaundice, no dark urine |
| Acute pancreatitis | RUQ/epigastric pain, vomiting | No radiation to back in a band-like pattern |
| Peptic ulcer disease | Epigastric pain | Pain is RUQ, not epigastric; no NSAID/alcohol history |
Investigations
Bloods:
| Test | Result | Interpretation |
|---|---|---|
| WBC | 14,200/µL | Leukocytosis - suggests active inflammation |
| CRP | 68 mg/L | Elevated - inflammatory marker |
| Total Bilirubin | 1.1 mg/dL | Normal - no duct obstruction |
| ALT / AST | 42 / 38 U/L | Mildly elevated |
| ALP | 95 U/L | Normal |
| Serum Lipase | 38 U/L | Normal - pancreatitis excluded |
| Serum Amylase | 55 U/L | Normal |
| Blood glucose | 7.2 mmol/L | Mildly elevated (background T2DM) |
| Urea / Creatinine | Normal | No organ dysfunction |
| Urine dipstick | Negative | UTI excluded |
Note: Bilirubin >2 mg/dL with a significant direct component would raise concern for choledocholithiasis, Mirizzi syndrome, or cholangitis.
Imaging:
Abdominal Ultrasound (US) - the first-line imaging of choice:
- Multiple echogenic foci with posterior acoustic shadowing in the gallbladder lumen - gallstones confirmed, largest measuring 1.4 cm
- Gallbladder wall thickening: 6 mm (normal <4 mm)
- Pericholecystic fluid present
- Sonographic Murphy's sign positive (pain reproduced when probe pressed over gallbladder)
- Common bile duct: 4 mm (normal) - no choledocholithiasis
US sensitivity for acute cholecystitis is 88-90%, specificity 80%. It identifies gallstones as small as 2 mm and can demonstrate the "double wall sign" (sonolucent halo around the gallbladder wall) in acute inflammation.
Diagnosis
Acute Calculous Cholecystitis (Grade I - Mild, Tokyo Guidelines)
- Grade I (Mild): No organ dysfunction, no severe local inflammation (no gangrenous or emphysematous change, no pericholecystic abscess, no perforation)
Understanding the Pathophysiology
The prior short-lived RUQ pain episodes were biliary colic - a gallstone intermittently obstructing the cystic duct, causing gallbladder distension and pain, then passing back into the lumen. Tonight, a stone became persistently impacted in the cystic duct. The sustained obstruction caused:
- Increased intraluminal pressure and gallbladder distension
- Ischemia of the gallbladder wall
- Release of prostaglandins and inflammatory mediators
- Secondary bacterial colonisation (E. coli, Klebsiella are the predominant organisms in ~50% of cases)
- Transmural inflammation = acute cholecystitis
Management
Immediate (ED):
- IV access + IV fluids - volume replacement, keep NBM (nil by mouth)
- Analgesia - IV ketorolac (NSAID first-line; analgesic efficacy comparable to opioids for biliary pain and may reduce short-term complications). Opioids (e.g., morphine) can be added if insufficient.
- Antiemetics - IV ondansetron or metoclopramide
- Antibiotics - IV cefuroxime + metronidazole (or piperacillin-tazobactam). Appropriate regimens include 2nd/3rd generation cephalosporins, carbapenems, beta-lactam/beta-lactamase inhibitor combinations, or fluoroquinolone + metronidazole.
- Surgical consultation - urgent
Definitive Treatment:
Early Laparoscopic Cholecystectomy - within 72 hours of admission (within the first week of symptom onset) is the treatment of choice. This approach results in a shorter hospital stay without increased serious complications compared to delayed surgery. This is a Grade 1A recommendation (Yamada's Gastroenterology).
If early surgery is not possible due to late presentation or high surgical risk, elective cholecystectomy after 6 weeks is preferred, as morbidity is higher between days 7-45.
Severity Grading and Management Algorithm (Tokyo Guidelines 2013)
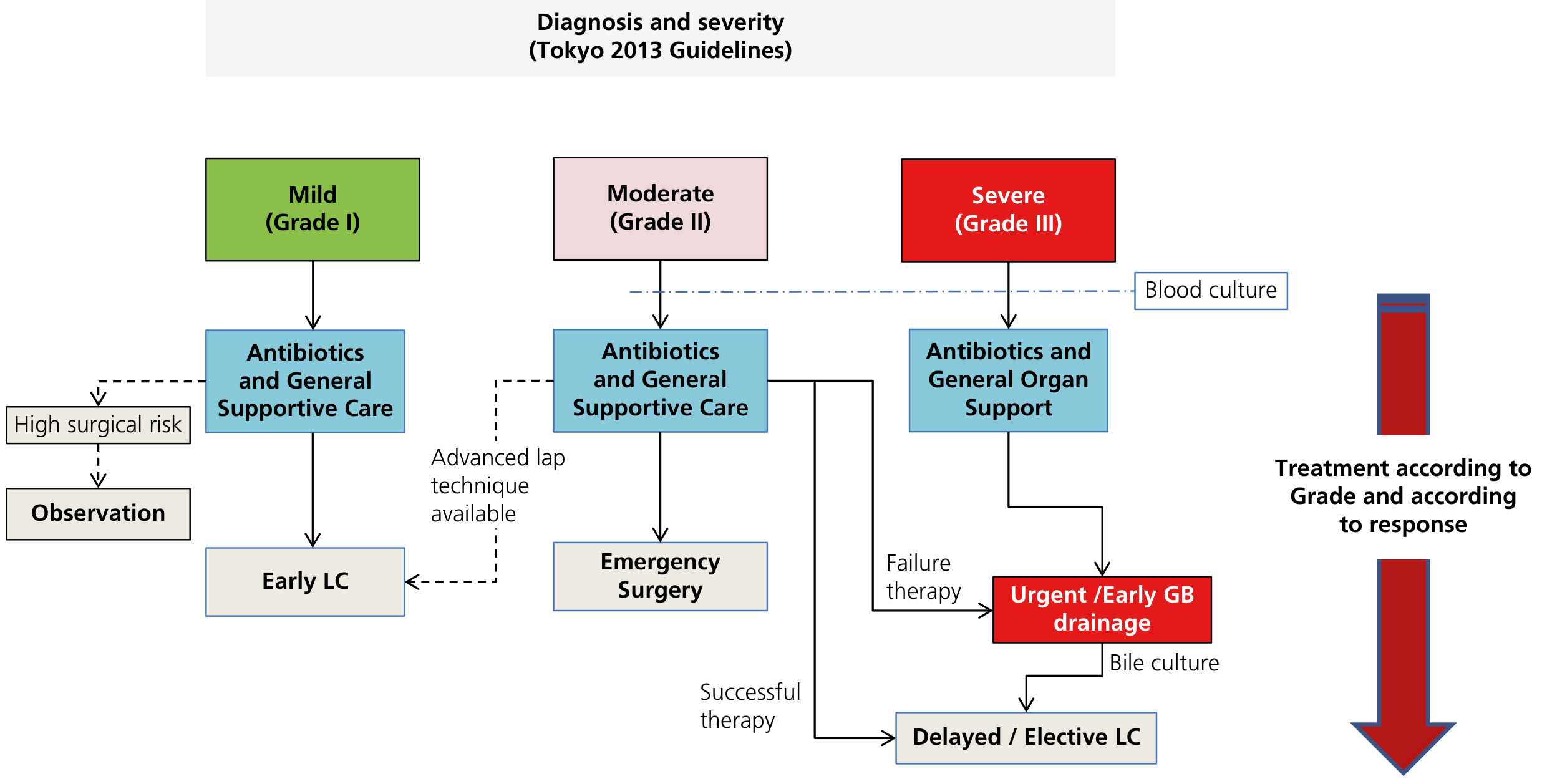
Management of acute cholecystitis based on Tokyo 2013 severity grading. LC = laparoscopic cholecystectomy; GB = gallbladder.
| Grade | Criteria | Management |
|---|---|---|
| Grade I (Mild) | No organ dysfunction; mild local inflammation | Antibiotics + supportive care → Early Laparoscopic Cholecystectomy |
| Grade II (Moderate) | Marked local inflammation (e.g., elevated WBC >18k, onset >72h, GB mass) | Antibiotics → Emergency surgery if advanced laparoscopic technique available; otherwise delayed/elective LC after successful therapy |
| Grade III (Severe) | Organ dysfunction (cardiovascular, neurological, respiratory, renal, hepatic, haematologic) | Antibiotics + organ support → Urgent gallbladder drainage → Delayed elective LC + bile culture |
Complications to Watch For
If left untreated or undertreated, Mrs. Sharma could develop:
| Complication | Description |
|---|---|
| Gangrenous cholecystitis | Necrosis of the GB wall; occurs in up to 20% of cases |
| Empyema of gallbladder | Pus-filled gallbladder from bacterial superinfection (E. coli, Klebsiella, Pseudomonas, Streptococci) |
| Gallbladder perforation | Usually at the fundus; can lead to pericholecystic abscess or peritonitis; rare but carries high mortality |
| Emphysematous cholecystitis | Gas-forming organisms (Clostridium, E. coli) infect the wall; more common in diabetic men; high mortality - requires urgent cholecystectomy |
| Choledocholithiasis | Stone migrating to the CBD causing jaundice and obstruction |
| Cholangitis | Infection of the biliary tree; life-threatening, demands urgent biliary decompression (ERCP preferred) |
| Gallstone pancreatitis | Stone impacting at the ampulla of Vater |
| Gallstone ileus (rare) | Cholecystoenteric fistula + stone impacting at ileocecal valve; causes bowel obstruction |
| Mirizzi syndrome | Impacted stone in cystic duct causing extrinsic compression of the CBD |
Patient Course
Mrs. Sharma is admitted, started on IV fluids, IV cefuroxime + metronidazole, and IV ketorolac. Her pain improves significantly within 4 hours. She undergoes laparoscopic cholecystectomy on day 2 of admission. Intraoperatively, the gallbladder is found to be oedematous with a 1.4 cm stone impacted in Hartmann's pouch. The surgery proceeds without conversion to open. She is discharged home on day 3 with analgesia and dietary advice to avoid high-fat meals in the short term.
Key Teaching Points
- Gallstones are common - 8% prevalence in men, 17% in women in the USA; prevalence rises with age and BMI.
- Most gallstones are asymptomatic - risk of developing symptoms/complications is 1-4% per year.
- Biliary colic vs. acute cholecystitis: Biliary colic is self-limiting (hours); cholecystitis is persistent (>6 hours) with fever and positive Murphy's sign.
- Murphy's sign is 65% sensitive, 87% specific for acute cholecystitis.
- Ultrasound is first-line imaging - cheap, no radiation, sensitivity 88-90%.
- Early laparoscopic cholecystectomy (within 1 week) is the standard of care - Grade 1A evidence.
- NSAIDs are first-line analgesia and may also reduce the risk of progression to cholecystitis in biliary colic.
- Diabetic patients are at special risk for emphysematous and gangrenous cholecystitis and should be monitored closely.
Sources: Tintinalli's Emergency Medicine, 9th ed. | Yamada's Textbook of Gastroenterology, 7th ed. | Fischer's Mastery of Surgery, 8th ed. | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Mulholland and Greenfield's Surgery, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.