Androgen
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile a thorough answer.
Androgens
Androgens are a group of steroid hormones that regulate the development and maintenance of male sex characteristics, though they are present and active in both sexes. Testosterone is the principal androgen; dihydrotestosterone (DHT) is its most potent metabolite.
1. Sources and Classification
| Source | Principal Androgens |
|---|---|
| Testes (Leydig cells) | Testosterone (main source in males) |
| Adrenal cortex | DHEA, androstenedione, small amounts of testosterone |
| Ovaries | Androstenedione, small amounts of testosterone |
| Peripheral tissues | DHT (from testosterone via 5α-reductase), estrogens (via aromatase) |
Adrenal androgens - DHEA and androstenedione - are weak. They serve as prohormones: in adipose and extra-adrenal tissues, androstenedione is converted to either testosterone or estrogens.
2. Biosynthesis
Adrenal Androgens
- Most 17-hydroxypregnenolone enters the glucocorticoid pathway.
- A fraction undergoes oxidative side-chain cleavage by 17,20-lyase (part of P450c17, a dual-function enzyme).
- This yields DHEA, which is converted to androstenedione by 3β-OHSD and Δ5,4-isomerase.
- Reduction of androstenedione at C-17 forms testosterone.
- In adrenogenital syndrome (CAH), impaired glucocorticoid synthesis shunts precursors into androgen synthesis, causing androgen excess.
Testicular Androgens (Leydig Cells)
-
LH from the anterior pituitary is the primary stimulus.
-
Rate-limiting step: cholesterol → pregnenolone via side-chain cleavage enzyme (P450scc), delivered by the transport protein StAR.
-
The predominant pathway in human testes is the Δ5 pathway: pregnenolone → 17α-hydroxypregnenolone → DHEA → androstenedione → testosterone.
-
Five enzyme activities in three proteins carry out the conversion:
- 3β-hydroxysteroid dehydrogenase + Δ5,4-isomerase
- 17α-hydroxylase + 17,20-lyase (both in P450c17)
- 17β-hydroxysteroid dehydrogenase
-
Harper's Illustrated Biochemistry, 32e, p. block4
Formation of DHT
- In target tissues (prostate, external genitalia, skin, epididymis), testosterone is converted to DHT by 5α-reductase.
- DHT is more potent than testosterone because of its higher affinity for the androgen receptor.
- The other metabolic pathway (oxidation at C-17) yields inactive or less-active 17-ketosteroids - primarily hepatic.
3. Mechanism of Action
Like other steroid hormones, androgens act intracellularly:
- Testosterone enters target cells and either acts directly or is converted to DHT by 5α-reductase (in skin, prostate, seminal vesicles, epididymis).
- Testosterone or DHT binds the intracellular androgen receptor (AR).
- The hormone-receptor complex undergoes conformational change, translocates to the nucleus, and binds androgen response elements (ARE) on DNA.
- This drives transcription of genes regulating growth, differentiation, and protein synthesis.
- Katzung's Basic and Clinical Pharmacology, 16e
4. Physiological Effects
Male
- In utero: differentiation of Wolffian ducts into epididymis, vas deferens, seminal vesicles (testosterone); external genitalia masculinization (DHT).
- Puberty: growth of testes, penis, and accessory glands; appearance of pubic, axillary, and facial hair; deepening of voice; acne; growth spurt followed by epiphyseal closure; enlargement of larynx; skeletal muscle growth.
- Adult: maintenance of secondary sex characteristics, spermatogenesis, libido.
- Erythropoiesis: natural androgens stimulate erythrocyte production.
- Protein anabolism: reduce urinary nitrogen excretion (increase protein synthesis or reduce catabolism) - more pronounced in women and children than in eugonadal men.
Female (when elevated)
- Facial and body hair growth (hirsutism)
- Deepening of voice
- Clitoral enlargement
- Frontal baldness
- Prominent musculature
- Menstrual irregularity
5. Feedback Regulation
- Androgens exert negative feedback on the hypothalamus (reducing GnRH) and anterior pituitary (reducing LH and FSH secretion).
- Inhibin, produced by Sertoli cells, also contributes to feedback suppression of FSH.
- Large doses are needed to suppress gonadotropins, suggesting inhibin + androgens together mediate physiological feedback.
6. Pharmacological Preparations
Androgenic:Anabolic Ratios (Animal Models)
| Drug | Androgenic:Anabolic |
|---|---|
| Testosterone | 1:1 |
| Testosterone cypionate | 1:1 |
| Testosterone enanthate | 1:1 |
| Methyltestosterone | 1:1 |
| Fluoxymesterone | 1:2 |
| Oxymetholone | 1:3 |
| Oxandrolone | 1:3 to 1:13 |
| Nandrolone decanoate | 1:2.5 to 1:4 |
Replacement Therapy Preparations
| Drug | Route | Dose |
|---|---|---|
| Methyltestosterone | Oral / sublingual | 25-50 mg/d / 5-10 mg/d |
| Fluoxymesterone | Oral | 2-10 mg/d |
| Testosterone enanthate | IM | 200 mg q2 weeks (adult) |
| Testosterone cypionate | IM | 200 mg q2 weeks (adult) |
| Testosterone | Transdermal patch/gel | 2.5-10 mg/d / 5-10 g/d (1% gel) |
- Katzung's Basic and Clinical Pharmacology, 16e, Table 40-6
7. Clinical Uses
- Hypogonadism - primary indication for replacement therapy in males with primary or secondary hypogonadal states. Long-acting IM esters (enanthate, cypionate) are preferred.
- Delayed puberty - gradually escalating doses in hypopituitary boys at expected pubertal age.
- Gynecologic uses - postpartum breast engorgement (with estrogens); endometriosis (danazol, a weak androgen); postmenopausal replacement (combined with estrogen); breast carcinoma in premenopausal women.
- Protein anabolic uses - catabolic states (burns, surgery, chronic illness); osteoporosis; aplastic anemia (though erythropoietin is now preferred).
- Male pattern baldness - finasteride 1 mg/d (via 5α-reductase inhibition).
8. Adverse Effects
- Virilization in women and children (irreversible deepening of voice)
- Premature epiphyseal closure in children (reduced final height)
- Hepatotoxicity - especially oral 17α-alkylated androgens (methyltestosterone); risk of cholestatic jaundice and hepatocellular carcinoma with prolonged use
- Polycythemia - from erythropoietic stimulation
- Sodium and water retention - edema, hypertension (caution in renal/cardiac disease)
- Suppression of spermatogenesis - testicular atrophy with large doses
- Gynecomastia - from peripheral aromatization to estrogens
- Dyslipidemia - decrease HDL, increase LDL
Contraindications: Prostate carcinoma, breast carcinoma in males, pregnancy.
9. Androgen Suppression and Antiandrogens
The HPG axis and sites of antiandrogen drug action:
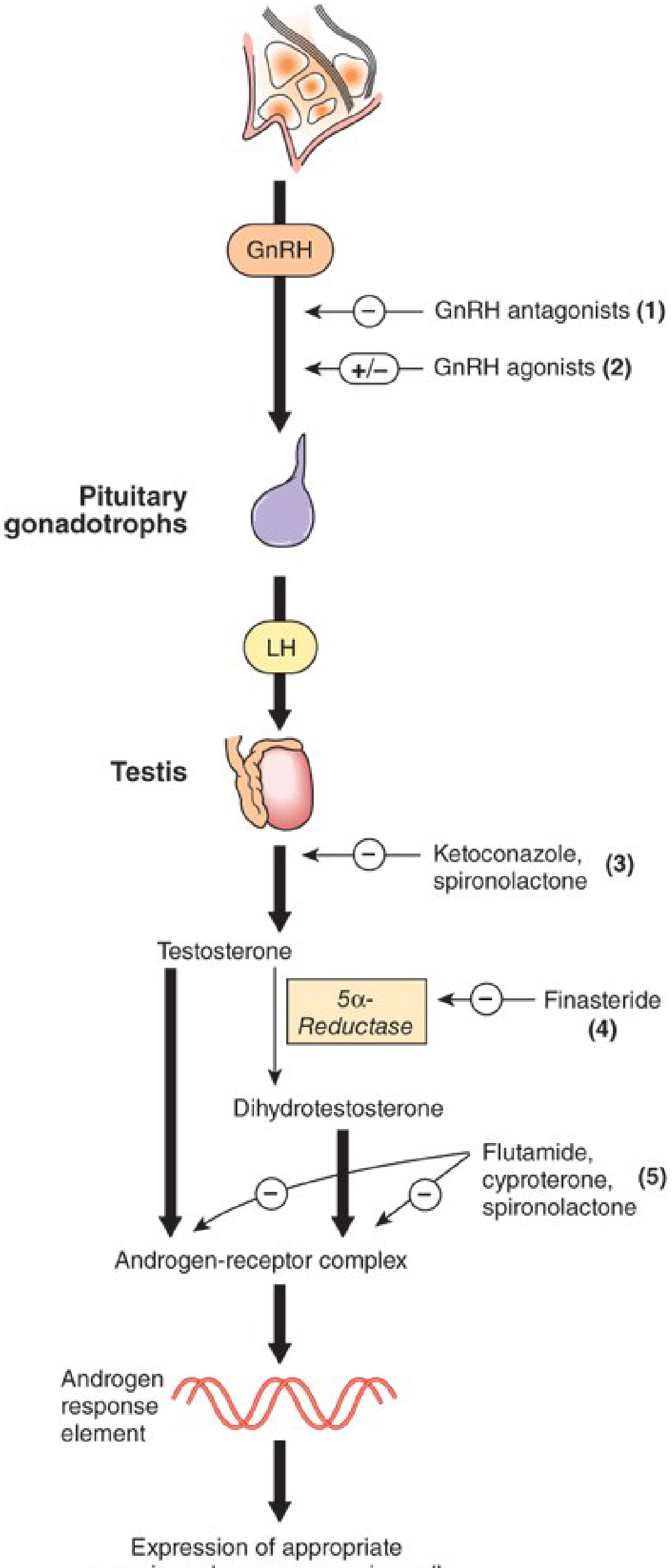
Sites of Intervention (numbered in diagram above)
- GnRH receptor antagonists - competitive block (e.g., degarelix)
- GnRH agonists - continuous (not pulsatile) administration desensitizes receptors, suppresses LH/FSH (e.g., leuprolide, goserelin, nafarelin, buserelin)
- Testicular synthesis inhibitors - ketoconazole, spironolactone
- 5α-Reductase inhibitors - block testosterone → DHT conversion
- Finasteride (5 mg/d for BPH; 1 mg/d for baldness) - onset within 8 hours, ~24h duration
- Dutasteride (0.5 mg/d) - slower onset, much longer half-life
- Androgen receptor antagonists (competitive)
- Flutamide - substituted anilide; used in prostate carcinoma; causes gynecomastia
- Bicalutamide, enzalutamide - newer, higher-affinity AR antagonists
- Cyproterone acetate - steroidal antiandrogen
- Spironolactone - weak AR antagonist in addition to aldosterone antagonism
Synthesis Pathway Inhibitors
- Ketoconazole - inhibits adrenal and gonadal steroidogenesis; increases estradiol:testosterone ratio (gynecomastia); toxicity limits use
- Abiraterone - 17α-hydroxylase/17,20-lyase inhibitor; approved for metastatic castration-resistant prostate cancer
10. Clinical Disorders
| Disorder | Mechanism | Key Features |
|---|---|---|
| Hypogonadism | Decreased testosterone production | Delayed puberty, sexual dysfunction, infertility |
| Androgen insensitivity syndrome | AR mutation | 46,XY females; blind vaginal pouch; absent uterus |
| CAH (21-hydroxylase deficiency) | Shunting to androgen pathway | Virilization in females; precocious puberty in males |
| BPH | DHT-driven prostatic growth | Urinary obstruction; treated with 5α-reductase inhibitors |
| Prostate carcinoma | Androgen-dependent growth | Androgen deprivation therapy (GnRH analogs, antiandrogens) |
| Polycystic ovary syndrome | Excess androgen production | Hirsutism, anovulation, insulin resistance |
| 5α-Reductase deficiency | Impaired DHT synthesis | 46,XY pseudohermaphroditism; virilization at puberty |
Sources:
- Katzung's Basic and Clinical Pharmacology, 16e, Chapter 40
- Basic Medical Biochemistry: A Clinical Approach, 6e, Chapter 32
- Harper's Illustrated Biochemistry, 32e, Chapter 41
- Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.