pancreatitis pathology detail notes
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I have all the content I need for comprehensive detailed notes. Let me now compile the full answer.
Pancreatitis - Detailed Pathology Notes
(Robbins & Kumar Basic Pathology + Sleisenger & Fordtran's GI and Liver Disease)
Overview
Inflammatory disorders of the pancreas are divided into acute and chronic forms. In acute pancreatitis, function can return to normal if the underlying cause is removed. Chronic pancreatitis causes irreversible destruction of the exocrine pancreas.
ACUTE PANCREATITIS
Definition
A reversible inflammatory disorder ranging in severity from focal edema and fat necrosis to widespread hemorrhagic necrosis.
- Annual incidence: 33-74 per 100,000 globally; 5-35 per 100,000 in the Western world
- Overall mortality ~5%
- Incidence is increasing due to the obesity epidemic and related gallstone disease
Etiology
Gallstones and chronic alcohol use account for ~80% of cases.
| Category | Causes |
|---|---|
| Metabolic | Alcohol use disorder*, hypertriglyceridemia (>1000 mg/dL - causes 5-10%), hypercalcemia, drugs (azathioprine, thiazides, estrogens, anticonvulsants, chemotherapy, valproate) |
| Mechanical | Gallstones*, trauma, iatrogenic/perioperative injury, post-ERCP |
| Nongallstone obstruction | Pancreatic cancer, periampullary neoplasms, pancreas divisum, biliary sludge, parasites (Ascaris, Clonorchis) |
| Infectious | Mumps virus, coxsackievirus (directly infect acinar cells) |
| Vascular | Shock, atheroembolism, polyarteritis nodosa |
| Genetic | PRSS1 (cationic trypsinogen), SPINK1 (trypsin inhibitor), CFTR mutations |
| Idiopathic | 10-20% of cases; many have underlying genetic basis |
Most common causes in the United States.
Pathogenesis
The core mechanism is autodigestion of the pancreas by intraacinar activation of pancreatic enzymes, particularly premature trypsin activation.
Key role of trypsin:
- PRSS1 mutations alter the trypsin self-cleavage (auto-inactivation) site → hyperactivation of trypsin
- Active trypsin activates multiple downstream digestive enzymes
- Trypsin converts prekallikrein → activated kallikrein (kinin system)
- Activates factor XII (Hageman factor) → clotting and complement systems
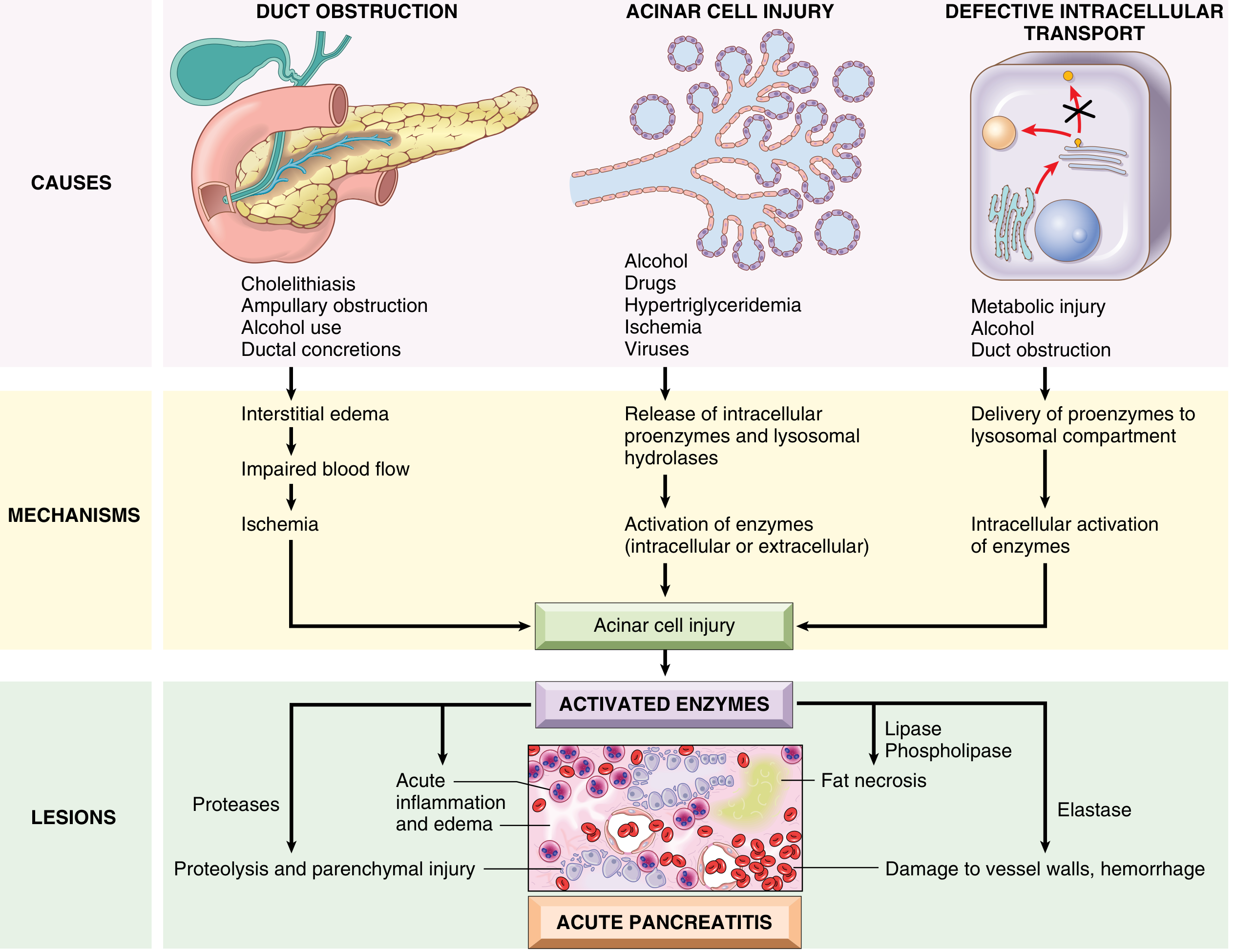
Three initiating pathways:
1. Pancreatic Duct Obstruction (gallstones, biliary sludge, mass)
- Blocks ductal flow → increased intraductal pressure → enzyme-rich interstitial fluid
- Lipase (secreted in active form) → local fat necrosis
- Injured tissues and leukocytes release proinflammatory cytokines → local inflammation and interstitial edema
- Edema compromises blood flow → vascular insufficiency and ischemic acinar cell injury
2. Primary Acinar Cell Injury (alcohol, hypertriglyceridemia, ischemia, viruses, drugs)
- Direct toxic effects → release of intracellular proenzymes and lysosomal hydrolases
- Intracellular or extracellular enzyme activation
3. Defective Intracellular Transport of Proenzymes (metabolic injury, alcohol, duct obstruction)
- In normal acinar cells, digestive enzymes (for zymogen granules) and hydrolytic enzymes (for lysosomes) travel in discrete pathways
- In metabolic injury, proenzymes and lysosomal hydrolases become co-packaged
- Leads to proenzyme activation and lysosomal rupture (phospholipases)
Alcohol-specific mechanisms:
- Transiently increases pancreatic exocrine secretion
- Causes contraction of the sphincter of Oddi
- Direct toxic effects / oxidative stress on acinar cells → membrane damage
- Delivers proenzymes to lysosomal compartment
- Chronic use → protein-rich pancreatic fluid → protein plugs → small duct obstruction
Morphology
The basic alterations are:
- Microvascular leakage causing edema
- Fat necrosis by lipases
- Acute inflammatory reaction
- Proteolytic destruction of pancreatic parenchyma and blood vessels → interstitial hemorrhage
Mild form (interstitial/edematous pancreatitis):
- Interstitial edema
- Focal areas of fat necrosis in the pancreas and peripancreatic fat
- Fat necrosis = enzymatic destruction of fat cells → released fatty acids combine with calcium → insoluble calcium soaps precipitate in situ
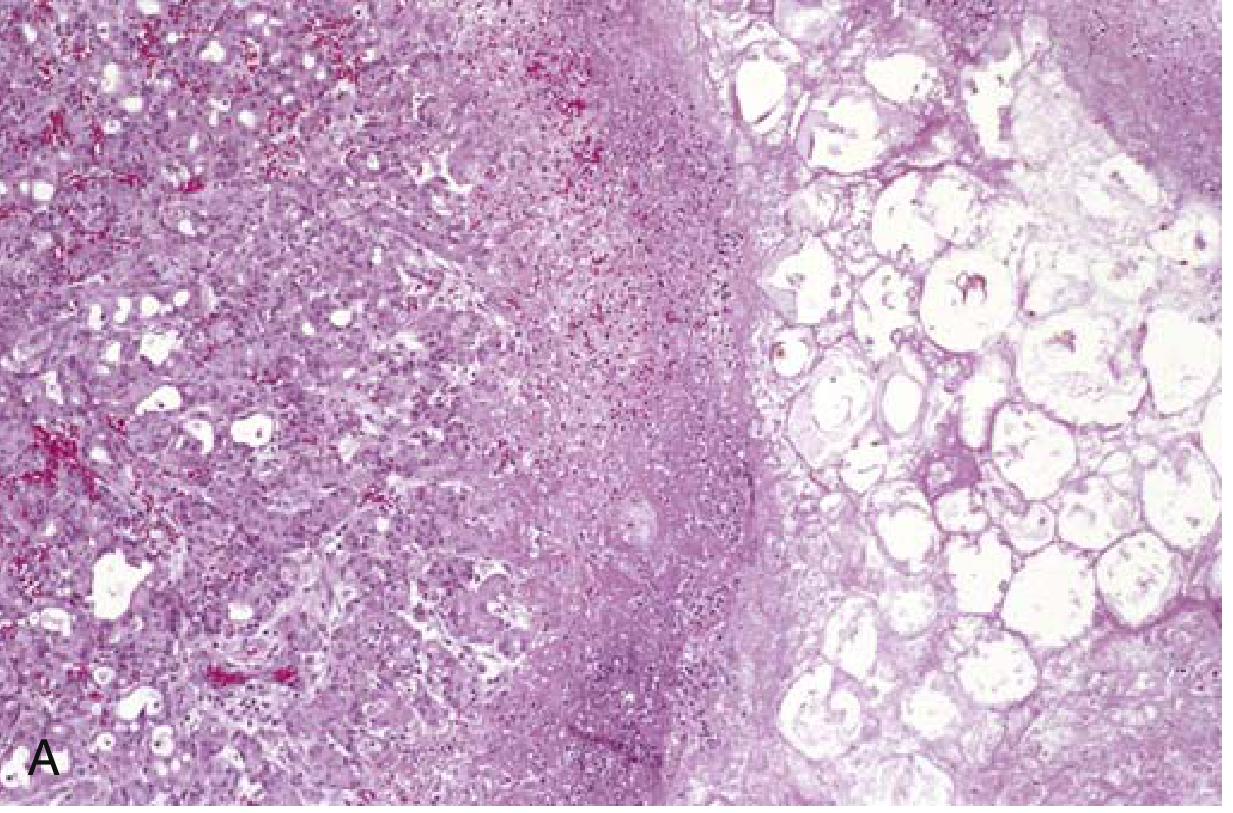
Severe form (acute necrotizing pancreatitis):
- Damage also involves acinar and ductal cells, islets of Langerhans, and blood vessels
- Macroscopically: red-black hemorrhagic areas interspersed with yellow-white chalky fat necrosis
- Fat necrosis can extend to extrapancreatic fat: omentum, bowel mesentery, even subcutaneous fat
- Peritoneum: serous, slightly turbid, brown-tinged fluid with fat globules
Most severe form (hemorrhagic pancreatitis):
- Extensive parenchymal necrosis with diffuse hemorrhage within the gland
Clinical Features
- Cardinal symptom: Abdominal pain - constant, intense, referred to the upper back
- Diagnosis: Elevated serum lipase and amylase (rise 4-12 hours after onset)
- 80% - mild and self-limiting; 20% - severe disease
Laboratory findings:
- Serum lipase - most specific and sensitive; remains elevated for 8-14 days
- Serum amylase - short half-life, returns to normal in 3-5 days
- Hypocalcemia - calcium precipitates in fat necrosis areas; if persistent, poor prognostic sign
- Leukocytosis
Severe acute pancreatitis (systemic manifestations):
- Disseminated intravascular coagulation (DIC)
- Acute respiratory distress syndrome (ARDS) - diffuse alveolar damage
- Diffuse fat necrosis
- Peripheral vascular collapse (shock): increased microvascular permeability → hypovolemia + endotoxemia (gut flora breach) + renal failure (acute tubular injury)
Severity scoring:
- Ranson's criteria - severe if ≥3 criteria; negative predictive value 90%, positive predictive value 50%
- APACHE II and BISAP scores also used
- CT severity index (Balthazar score)
Complications:
- In 40-60% of acute necrotizing pancreatitis, necrotic debris becomes infected (most commonly by gram-negative organisms from gut)
- Pancreatic pseudocyst - collection of necrotic material walled off by fibrous tissue; lacks epithelial lining, lined by fibrin and granulation tissue
CHRONIC PANCREATITIS
Definition
Long-standing inflammation leading to irreversible destruction of the exocrine pancreas, followed eventually by loss of the islets of Langerhans. Recurrent bouts of acute pancreatitis (regardless of etiology) can evolve into chronic pancreatitis.
- Prevalence: 0.04-5% of U.S. population; 9-62 per 100,000 globally
Etiology
- Most common: Chronic excessive alcohol consumption (especially middle-aged men)
- Functional or anatomic duct obstruction
- Genetic mutations: CFTR, PRSS1, SPINK1 (same genes as hereditary acute pancreatitis)
- Autoimmune pancreatitis - IgG4-secreting plasma cells (IgG4-related disease); responds to anti-B cell/steroid therapy
- Idiopathic: ~40% of cases (many are "idiopathic" but have genetic basis)
How alcohol causes chronic injury (proposed mechanisms):
- Alters activation of digestive enzymes
- Increases production of oxygen-derived free radicals
- Direct toxic effects on acinar cells
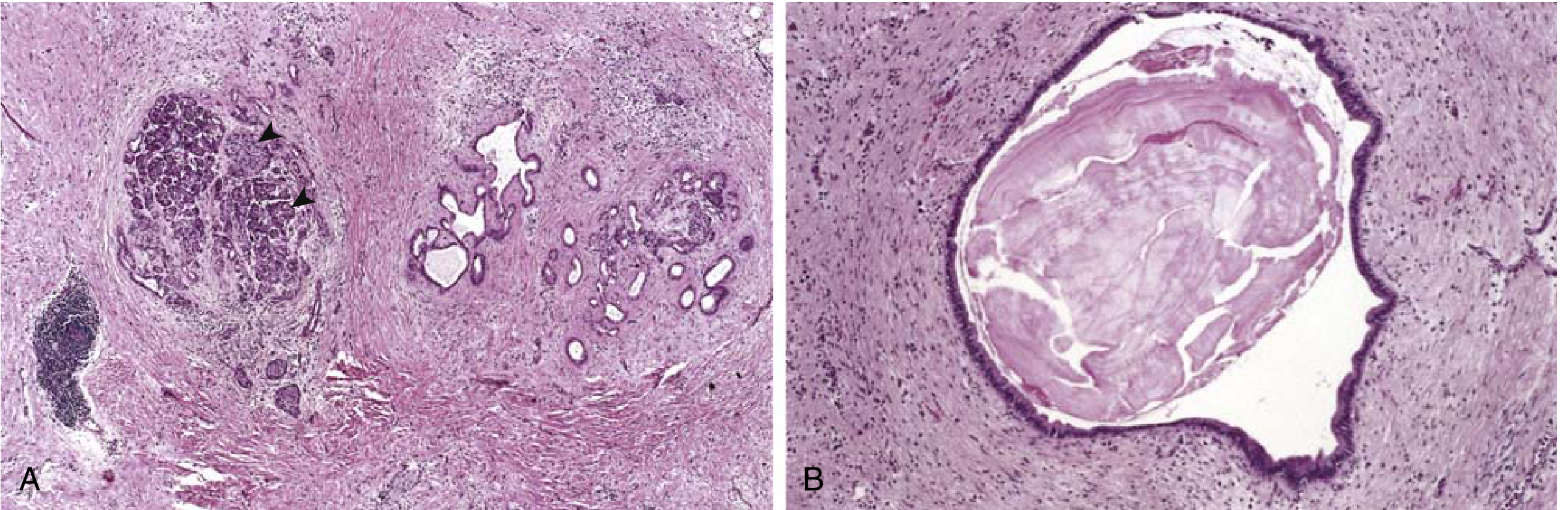
Pathology / Morphology
Gross:
- Gland is hard (fibrosis)
- Sometimes extremely dilated ducts
- Visible calcific concretions
Microscopy:
- Parenchymal fibrosis (collagenous stroma)
- Reduced number and size of acini (acinar loss - constant feature)
- Variable dilation of pancreatic ducts
- Relative sparing of islets of Langerhans (initially)
- Chronic inflammatory infiltrate around remaining lobules and ducts
- Ductal epithelium may be atrophied, hyperplastic, or exhibit squamous metaplasia
- Ductal concretions (inspissated eosinophilic material in dilated ducts)
- Eventually islets also disappear and become embedded in sclerotic tissue
Autoimmune pancreatitis (special type):
- Striking lymphocyte and plasma cell infiltration (IgG4+ plasma cells)
- "Swirling" fibrosis
- Venulitis (lymphocytic sclerosing pancreatitis)
Clinical Features
- Abdominal pain - most common symptom
- Repeated bouts of jaundice
- Vague indigestion, persistent/recurrent abdominal and back pain
- May be silent until exocrine insufficiency and diabetes develop (islet destruction)
Precipitating attacks:
- Excessive alcohol use
- Overeating (increases demand on pancreatic secretions)
- Opiates or drugs that increase tone of sphincter of Oddi
Diagnosis:
- With extensive fibrosis, enzyme elevations may be absent
- Weight loss and hypoalbuminemic edema from malabsorption (exocrine insufficiency)
- Deficiency of fat-soluble vitamins (particularly vitamin D) → osteopenia
- CT/US showing calcifications within the pancreas (helpful finding)
Complications of Chronic Pancreatitis
- Pancreatic pseudocysts - develop in ~10% of patients
- Pancreatic cancer - most serious long-term complication
- Patients with hereditary pancreatitis (PRSS1 mutations): 40% lifetime risk of pancreatic cancer
- Other forms of chronic pancreatitis: only modestly elevated risk
- Diabetes mellitus (destruction of islets)
- Exocrine pancreatic insufficiency with steatorrhea, malabsorption
- Mortality: 50% over 20-25 years
Quick Comparison: Acute vs. Chronic Pancreatitis
| Feature | Acute Pancreatitis | Chronic Pancreatitis |
|---|---|---|
| Reversibility | Reversible (if cause removed) | Irreversible |
| Most common cause | Gallstones, alcohol | Alcohol |
| Morphology | Edema, fat necrosis, hemorrhage | Fibrosis, acinar loss, calcifications |
| Islet involvement | In severe cases | Late finding |
| Key enzyme marker | Lipase (more specific, longer lasting) | Enzymes may be absent (burnt out) |
| Key complication | Infected necrosis, ARDS, DIC | Pancreatic cancer, diabetes, malabsorption |
| Genetics | PRSS1, SPINK1, CFTR | PRSS1, SPINK1, CFTR |
Pancreatic Pseudocyst (Complication of Both)
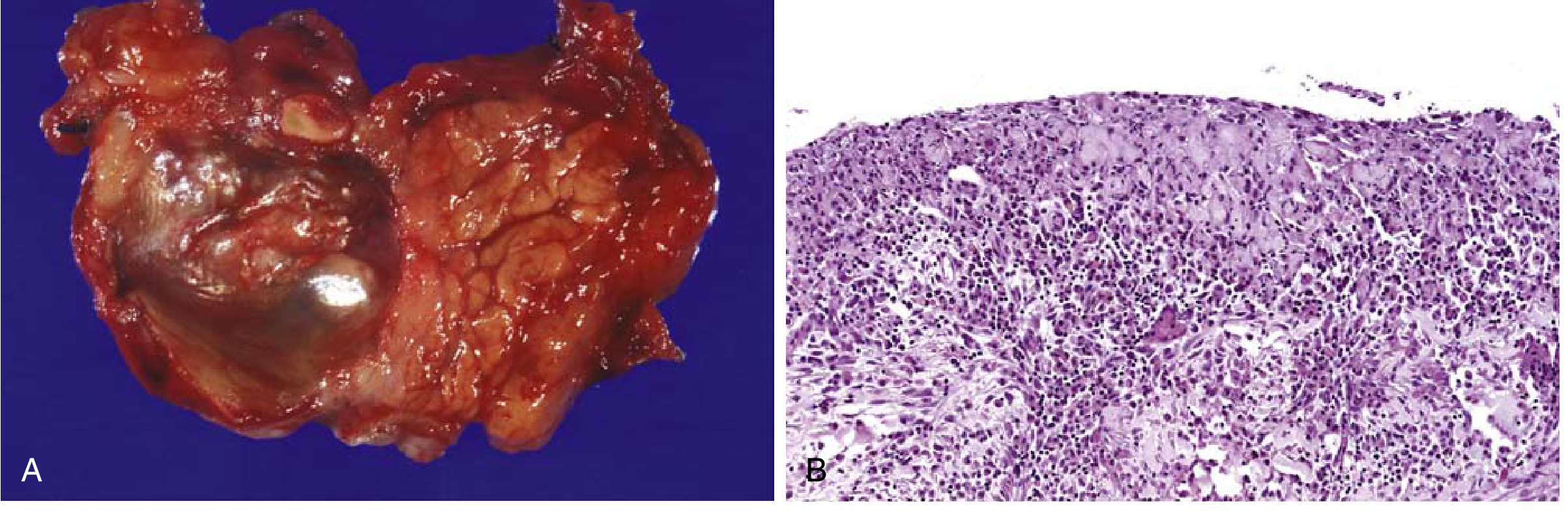
- Poorly defined cyst with necrotic brownish wall
- Lacks epithelial lining (distinguishes it from true cysts)
- Lined by fibrin and granulation tissue
- Contains necrotic debris
Sources: Robbins & Kumar Basic Pathology (pp. 640-646); Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.