Acute pericarditis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute pericarditis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile it:
Acute Pericarditis
Definition and Epidemiology
Acute pericarditis is an inflammatory syndrome of the pericardium, with or without pericardial effusion, lasting up to 4-6 weeks. It accounts for approximately 5% of emergency department visits for nonischemic chest pain. Incidence in developed countries is roughly 27.7 cases/100,000 population/year. Men aged 16-65 are at higher risk (RR 2.02 vs women). In-hospital mortality is low (~1.1%) but rises with age and severe concurrent infections.
- Braunwald's Heart Disease, p. 940
- Fuster and Hurst's The Heart, 15th Ed., p. 1638
Etiology
In developed countries, ~85% of cases are idiopathic or viral (presumed viral even when unconfirmed, as specific viral testing is costly with low yield). In developing/endemic regions, tuberculosis is the most common cause.
| Category | Key Examples |
|---|---|
| Viral (most common) | Coxsackievirus B, echovirus, adenovirus, CMV, EBV, parvovirus B19, SARS-CoV-2 |
| Bacterial | M. tuberculosis (most important globally), Pneumococcus, Staphylococcus |
| Fungal | Histoplasma (immunocompetent), Aspergillus, Candida (immunocompromised) |
| Autoimmune | SLE, rheumatoid arthritis, scleroderma, sarcoidosis, Sjögren, FMF, Still disease |
| Neoplastic | ~6% of cases; metastatic lung/breast cancer, lymphoma; primary mesothelioma |
| Post-cardiac injury | Dressler syndrome, post-pericardiotomy, post-ablation/PCI |
| Metabolic | Uremia, hypothyroidism (myxedema), anorexia nervosa |
| Drug-induced | Procainamide, hydralazine, isoniazid (lupus-like); checkpoint inhibitors |
| Radiation-induced | After thoracic radiotherapy |
- Goldman-Cecil Medicine, p. 2204
- Fuster and Hurst's The Heart, Table 53-2
Clinical Features
Symptoms
- Sharp, pleuritic chest pain - typically retrosternal, severe, and debilitating
- Worse with inspiration and supine position
- Relieved by sitting up and leaning forward (reduces pericardial contact)
- Radiation to the scapular ridge (phrenic nerve irritation)
- Low-grade fever (<38°C) and sinus tachycardia
Signs
-
Pericardial friction rub - pathognomonic; heard in ~1/3 of cases
- High-pitched, scratchy sound
- Up to 3 components: ventricular ejection, rapid early diastolic filling, atrial systole
- Best heard at the lower left sternal border with patient leaning forward
- Evanescent - requires repeated auscultation
- Key distinction: pericardial rub persists during breath-holding; pleural rub disappears
-
Goldman-Cecil Medicine, p. 2212-2213
-
Braunwald's Heart Disease, p. 1884
Diagnosis
Diagnostic Criteria (2 of 4 required)
- Typical pleuritic chest pain
- Pericardial friction rub
- Characteristic ECG changes
- New or worsening pericardial effusion on imaging
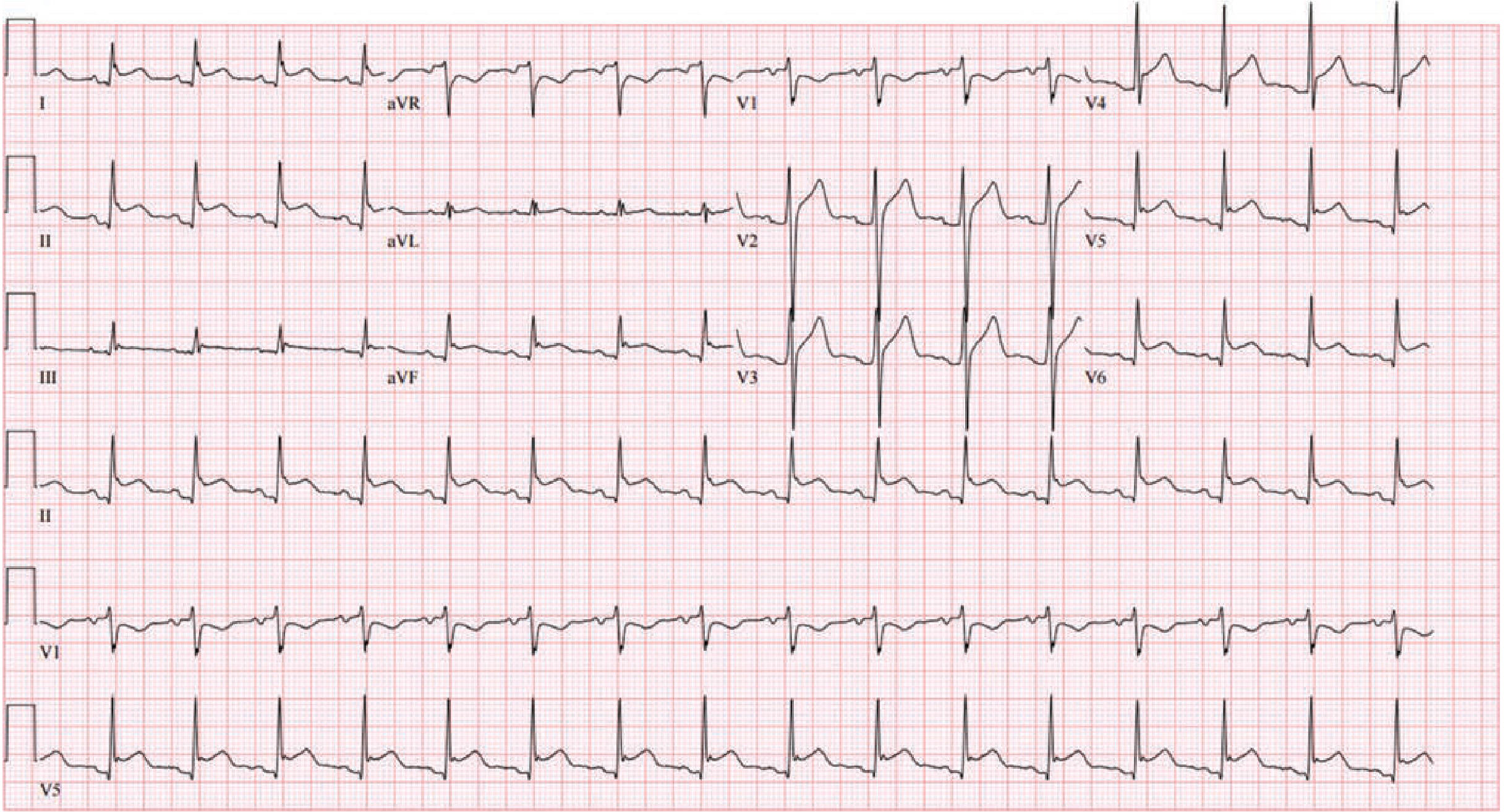
ECG Changes - 4 Stages (Spodick's Sign)
| Stage | Finding |
|---|---|
| Stage I (acute, days 1-2) | Diffuse concave-up ST elevation in all leads except aVR (ST depression) and often V1; PR-segment depression (virtually pathognomonic) |
| Stage II (days to weeks) | ST segments normalize; T waves flatten |
| Stage III | Diffuse T-wave inversions |
| Stage IV | ECG normalizes |
ECG distinguishing from STEMI:
| Feature | Acute Pericarditis | STEMI |
|---|---|---|
| ST morphology | Concave up (saddle-shaped) | Usually convex |
| Distribution | Widespread (nearly all leads) | Localized (territory-specific) |
| Reciprocal ST depression | Absent | Common |
| PR depression | Present | Absent |
| Q waves | Absent | May develop |
| T-wave inversion | After ST normalization | Before/with ST changes |
The ECG below shows classic Stage I changes - diffuse ST elevation with PR depression, with reciprocal changes in aVR:
Laboratory Tests
- CRP/ESR: elevated (CRP is the best marker for guiding treatment duration and taper)
- CBC: leukocytosis
- Troponin: mildly elevated in ~30-50% due to epicardial involvement (myopericarditis); usually returns to normal within 1-2 weeks - a persistently elevated troponin raises concern for myocarditis
- Serum creatinine: assess for uremia as etiology
- Routine viral titers are NOT recommended (costly, low yield, do not change management)
Imaging
-
Echocardiography: normal in ~40% of cases; performed to detect effusion and assess hemodynamics
-
Chest X-ray: may show enlarged cardiac silhouette if effusion >300 mL; otherwise normal
-
Cardiac MRI: most sensitive for pericardial inflammation (gadolinium enhancement); useful when diagnosis is uncertain or to assess for myocarditis
-
Goldman-Cecil Medicine, pp. 2218-2224
-
Braunwald's Heart Disease, p. 1888-1920
Risk Stratification - High-Risk Features (Predictors of a Specific Cause)
The following features predict a higher likelihood of a non-idiopathic (potentially serious) etiology and may warrant hospitalization or further workup:
-
Fever >38°C
-
Subacute onset
-
Large pericardial effusion or cardiac tamponade
-
Immunocompromised state
-
Recent anticoagulant use
-
Trauma
-
Failure to respond to NSAIDs/aspirin within 1 week
-
Goldman-Cecil Medicine, p. 2205
Treatment
Non-pharmacologic
- Physical activity restriction: athletes should avoid competitive sports until symptom resolution and normalization of CRP, ECG, and echo (generally minimum 3 months)
- Non-athletes: restrict strenuous activity until symptom-free
Pharmacologic - First-Line
Aspirin OR NSAIDs + Colchicine (combination)
| Drug | Dose | Duration | Taper |
|---|---|---|---|
| Aspirin | 750-1000 mg every 8 h | 1-2 weeks | Decrease by 250-500 mg every 1-2 weeks |
| Ibuprofen | 600-800 mg every 8 h | 1-2 weeks | Decrease dose every 1-2 weeks |
| Colchicine | 0.5 mg once daily (<70 kg) OR 0.5 mg twice daily (≥70 kg) | 3 months | Optional taper over 2-3 weeks |
- Aspirin is preferred if concurrent anticoagulation is needed (e.g., post-MI)
- Colchicine added to NSAIDs significantly reduces recurrence (from ~32% to ~11%, per the COPE and ICAP trials)
- Therapy duration guided by symptoms AND normalization of hsCRP (do not taper early if CRP still elevated)
Corticosteroids - Second-Line (Use Cautiously)
Corticosteroids should be avoided as first-line because they:
- Impair clearance of infectious agents
- Increase risk of recurrence when used at high doses
Indications for corticosteroids:
- Contraindication to or failure of NSAID + colchicine
- Autoimmune disease as the primary indication (e.g., SLE)
- Renal failure (NSAIDs contraindicated)
- Pregnancy
- Concurrent oral anticoagulation therapy (relative contraindication to NSAIDs)
Dose: Low-dose prednisone 0.2-0.5 mg/kg/day; taper slowly over 6-12 weeks guided by symptoms and CRP. Always add colchicine concurrently.
- Braunwald's Heart Disease, p. 1991-1995
Recurrent Pericarditis
- Occurs in 15-30% of idiopathic cases
- Defined as recurrence after a symptom-free interval of ≥4-6 weeks with new objective evidence (rub, ECG changes, new effusion, elevated CRP)
- Treatment: NSAID + colchicine (same doses as initial episode)
- For corticosteroid-dependent recurrence: anakinra (IL-1 receptor antagonist) or rilonacept have shown benefit in refractory cases
Complications
| Complication | Frequency | Notes |
|---|---|---|
| Pericardial effusion | Common (small effusions very frequent) | Usually resolve with treatment |
| Cardiac tamponade | ~3% over 31-month follow-up | More likely with bacterial, neoplastic, or traumatic etiology |
| Constrictive pericarditis | ~1.5-1.8% overall | Extremely rare with idiopathic (~0.48%); higher risk with bacterial TB |
| Myopericarditis | ~15% | Concurrent myocardial involvement; elevated troponin marker |
| Recurrence | 15-30% | Associated with poor quality of life; not linked to constriction |
Patients with idiopathic pericarditis can be reassured that constrictive pericarditis is exceedingly unlikely.
- Braunwald's Heart Disease, pp. 1997-2000
Differential Diagnosis
Conditions most easily confused with acute pericarditis:
- STEMI (most important distinction - see ECG table above)
- Pulmonary embolism
- Pneumonia with pleurisy
- Costochondritis
- Aortic dissection
- Gastroesophageal reflux
- Herpes zoster (pre-eruption)
- Takotsubo cardiomyopathy (elevated troponin + ECG changes)
Sources: Braunwald's Heart Disease (10th/12th Ed.); Goldman-Cecil Medicine International Edition; Fuster and Hurst's The Heart, 15th Ed.; Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.