Give notes on development of female reproductive system from mullerian ducts and it's anamolies
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the key information needed. Let me compile comprehensive notes.
Development of the Female Reproductive System from Mullerian Ducts and Anomalies
1. Background - The Indifferent (Bisexual) Stage
Both male and female embryos start with two sets of paired ducts running alongside the mesonephros (second primitive kidney):
- Mullerian ducts (paramesonephric ducts) - precursors of the female tract
- Wolffian ducts (mesonephric ducts) - precursors of the male tract
The default developmental pathway in the absence of testicular hormones (testosterone and AMH) is female. No ovarian hormone is required for the female tract to develop - the ovary is not needed for Mullerian duct development to proceed.
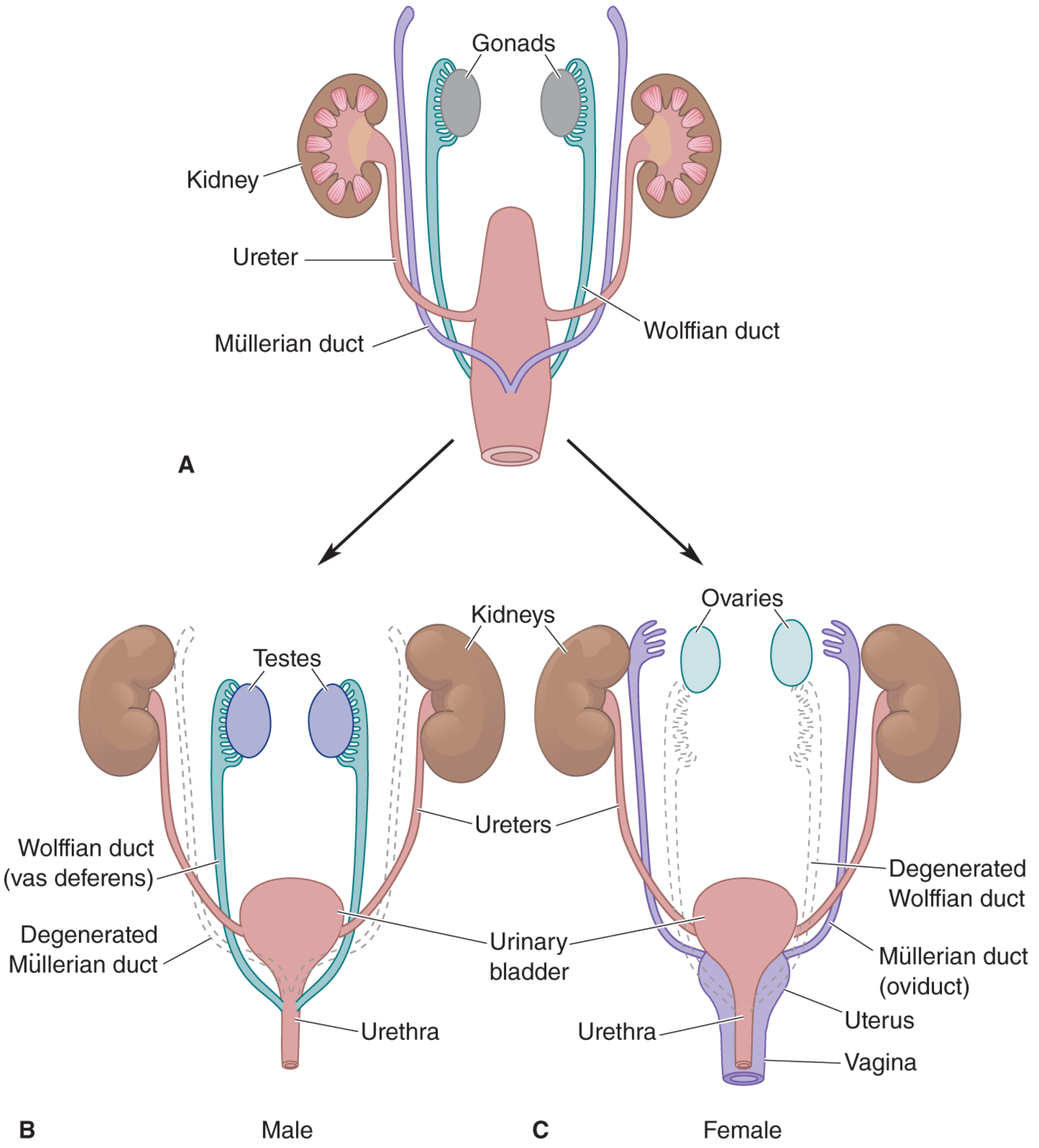
Diagram showing: (A) Indifferent stage with both Mullerian and Wolffian ducts. (B) Male - Wolffian duct becomes vas deferens, Mullerian duct degenerates. (C) Female - Mullerian duct forms oviduct/uterus/vagina, Wolffian duct degenerates.
2. Initiation of Mullerian Duct Development (Week 5)
- At week 5, the coelomic epithelium invaginates on the lateral surface of the paired urogenital ridges
- These infoldings later become the tubal ostia of the Mullerian (paramesonephric) ducts
- The Wolffian duct acts as a "guidewire" - the Mullerian duct grows caudally alongside it; the Wolffian duct is requisite for caudal MD migration to the urogenital sinus (UGS)
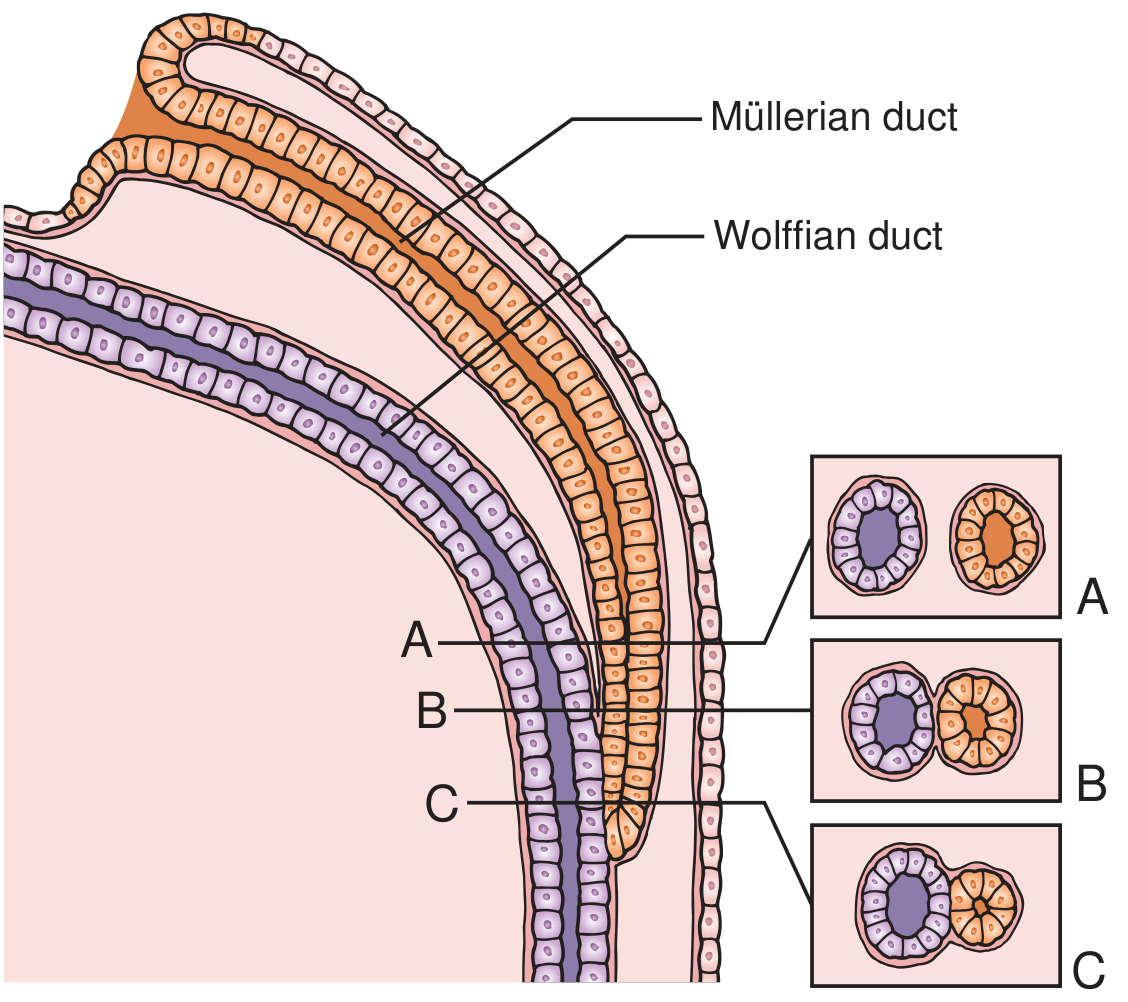
Three stages of Mullerian-Wolffian duct relationship during caudal migration: (A) mesenchyme intervening between them, (B) contact of basement membranes only, (C) direct epithelial contact at the tip.
3. Fate of the Wolffian Duct in Females
In the female fetus, the Wolffian ducts degenerate after serving as guidewires, leaving only vestigial remnants:
| Remnant | Location |
|---|---|
| Epöophoron | Broad ligament (cranial) |
| Paroöphoron | Broad ligament (caudal) |
| Gartner's duct | Fibromuscular wall of the vagina |
4. Key Developmental Events - Week-by-Week Timeline
| Week | Event |
|---|---|
| Week 5 | Coelomic epithelium invaginates; Mullerian duct initiation |
| Weeks 7-8 | Right and left MDs approach midline, lie between the two Wolffian ducts heading to the UGS |
| Week 8 | Paired MDs fuse in the midline to form the uterovaginal canal |
| Week 8 onwards | Midline epithelial septum (zone of MD fusion) must regress - failure causes uterine malformations |
| Week 9.5 | Unfused cranial portions form the fallopian tubes; fused caudal portions form the uterovaginal canal |
| Week 12 | Solid vaginal plate is forming; PAX2-positive Mullerian epithelium present throughout |
| Week 15 | Canalization of the solid vaginal plate begins |
| Weeks 18-19 | Canalization mostly complete; vaginal fornices well defined |
| Week 21 | Vaginal epithelium is many cell layers thick and glycogenated (due to endogenous estrogen) |
5. Derivatives of the Mullerian Duct
| Structure | Derived From |
|---|---|
| Fallopian tubes | Cranial, unfused portions of paired MDs |
| Uterine corpus | Cranial part of the fused uterovaginal canal |
| Uterine cervix | Caudal part of the fused uterovaginal canal |
| Upper vagina (partial) | Caudal uterovaginal canal + sinovaginal bulbs from urogenital sinus |
Note on vaginal epithelium: Both Mullerian epithelium (PAX2-positive) and urogenital sinus epithelium (FOXA1-positive, endodermal) contribute to the vagina. The UGS-derived epithelium progressively replaces Mullerian epithelium from the caudal end upward. By adulthood, the vagina is FOXA1-positive (UGS-derived), while the cervix remains PAX2-positive (Mullerian-derived).
6. Fallopian Tube Development
- Develops from the paired cranial portions of the MDs that are NOT fused
- Fimbria develop from the irregular ostia of the MDs
- At 8 weeks, the tubes are narrow with circular epithelial profile
- Over subsequent months:
- Mucosa becomes highly folded, most prominent in infundibulum and ampulla
- Loose mesenchyme differentiates into inner stroma + outer smooth muscle layer
7. Uterine Corpus and Cervix Development
- The uterovaginal canal is initially lined by a midline epithelial septum (zone of fusion)
- This septum must regress - failure of regression = various uterine malformations
- Uterine corpus: Endometrial stroma + uterine glands derive from Mullerian epithelium and surrounding mesenchyme; myometrium differentiates from surrounding mesenchyme
- Cervical epithelium: Near the external os, Mullerian epithelium differentiates into stratified squamous epithelium covering the exocervix
8. Vaginal Development
- The caudal uterovaginal canal joins the urogenital sinus
- Sinovaginal bulbs form from UGS epithelium
- A solid vaginal plate forms from both UGE and Mullerian epithelium
- Canalization begins ~week 15, complete by weeks 18-19
- The hymen represents the junction of the vaginal plate and the UGS
9. Mullerian Duct Anomalies (MDAs) - Classification
MDAs are classified according to the Buttram & Gibbons / American Fertility Society (AFS) classification:
Class I - Uterine Agenesis or Hypoplasia
- Failure of both Mullerian ducts to develop normally
- Ovaries are normal (distinguishes it from androgen insensitivity syndrome and gonadal dysgenesis)
- Most common subtype: Mayer-Rokitansky-Kuster-Hauser (MRKH) Syndrome
- Uterine and vaginal agenesis/hypoplasia
- Intact ovaries and fallopian tubes
- 46,XX karyotype
- MRI is more reliable than ultrasound for detecting uterine remnants
Class II - Unicornuate Uterus
- Failure of one Mullerian duct to develop normally
- Associated with increased spontaneous abortion and obstetric complications
- Imaging: "banana-like" configuration on axial oblique MRI - curved, elongated uterus tapering off midline
- May have a rudimentary horn (communicating or non-communicating):
- Functional non-communicating horn: accumulates blood → haematometra
- Associated with increased risk of endometriosis
Class III - Uterus Didelphys
- Non-fusion of the entire Mullerian duct pair → two separate, normal-sized uterine horns and two cervices
- Longitudinal vaginal septum present in ~75% of cases
- MRI: two uterine horns widely separated, each with preserved normal zonal anatomy (endometrial and myometrial widths preserved)
- Obstetric complications relate to degree of non-fusion
Class IV - Bicornuate Uterus
- Incomplete fusion of the cephalad uterovaginal horns with resorption of the uterovaginal septum
- Results in two horns joined caudally with a concave external fundal contour
- Intervening cleft ≥1 cm in the external fundal myometrium
- Each horn shows normal myometrial signal intensity
Class V - Septate Uterus
- Most common Mullerian duct abnormality
- Mechanism: incomplete resorption of the fibrous septum between the two uterine horns
- Septum may be partial or complete (extending to external cervical os)
- Worst obstetric outcome of all MDAs
- Key MRI feature: convex, flat, or concave (≤1 cm) external uterine contour (distinguishes it from bicornuate uterus which has a deeper cleft)
- Treatment: Hysteroscopic metroplasty (surgical resection of the septum)
Class VI - Arcuate Uterus
- Considered a normal variant
- Smooth, broad indentation of the fundus of the uterine cavity
- Normal external uterine contour
- No significant effect on fertility or pregnancy
10. Other Important Anomalies
Vaginal Agenesis / Transverse Vaginal Septum
- Failure of canalization of the vaginal canal
- Incidence: ~1 in 80,000 women
- Septum typically at the junction of the middle and superior third of the vagina
- Can cause haematocolpos (blood in vagina) and haematometrocolpos
Imperforate Hymen
- Most common cause of vaginal obstruction
- Failure of the inferior end of the vaginal canal to open
- Presents with cyclic abdominal pain in adolescent females; bulging at the introitus
OHVIRA Syndrome (Obstructed Hemivagina and Ipsilateral Renal Anomaly)
- Rare congenital anomaly involving combined Mullerian and urinary tract malformations
- Caused by abnormal development of both MDs and Wolffian ducts (they develop together)
- Presents after menarche: cyclical abdominal pain, vaginal discharge; can present as acute abdomen / tubo-ovarian abscess
- Renal anomaly: typically ipsilateral renal dysplasia or agenesis
Persistent Mullerian Duct Syndrome (in Males)
- A male anomaly: 46,XY males with normal male external genitalia but persistent uterus and fallopian tubes
- Due to AMH (anti-Mullerian hormone) deficiency or resistance
- Can present with cryptorchidism or inguinal hernia
11. Summary - Key Points for Exams
| Mechanism | Resulting Anomaly |
|---|---|
| Failure of both MDs to develop | MRKH syndrome (Class I agenesis) |
| Failure of one MD to develop | Unicornuate uterus (Class II) |
| Complete failure of midline fusion | Uterus didelphys (Class III) |
| Incomplete cranial fusion | Bicornuate uterus (Class IV) |
| Failure of septum resorption | Septate uterus (Class V) - most common |
| Normal variant | Arcuate uterus (Class VI) |
| Failure of canalization | Transverse vaginal septum |
| Failure of inferior canal opening | Imperforate hymen |
| Combined MD + WD abnormality | OHVIRA syndrome |
Key principle: The ovary is NOT required for female duct development. The absence of testosterone and AMH is sufficient for the Mullerian ducts to develop and the Wolffian ducts to regress. Unilateral testicular removal in experiments leads to female duct development on the ipsilateral (castrated) side only.
Sources: Campbell-Walsh-Wein Urology (5th Volume), p. 435-436; Grainger & Allison's Diagnostic Radiology, p. 889-891; Neuroscience: Exploring the Brain, 5th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.