Cerebral autoreglation
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cerebral autoregulation"[MeSH Terms] AND review
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have excellent material from multiple authoritative textbooks with diagrams. Let me compile the comprehensive answer.
Cerebral Autoregulation
Definition
Cerebral autoregulation (CA) is the intrinsic ability of the cerebral vasculature to maintain a relatively constant cerebral blood flow (CBF) despite changes in cerebral perfusion pressure (CPP). It is a homeostatic mechanism that protects the brain from both ischemia (at low pressures) and hyperemia/edema (at high pressures).
Normal CBF is approximately 50 mL/100 g/min.
The Autoregulation Curve
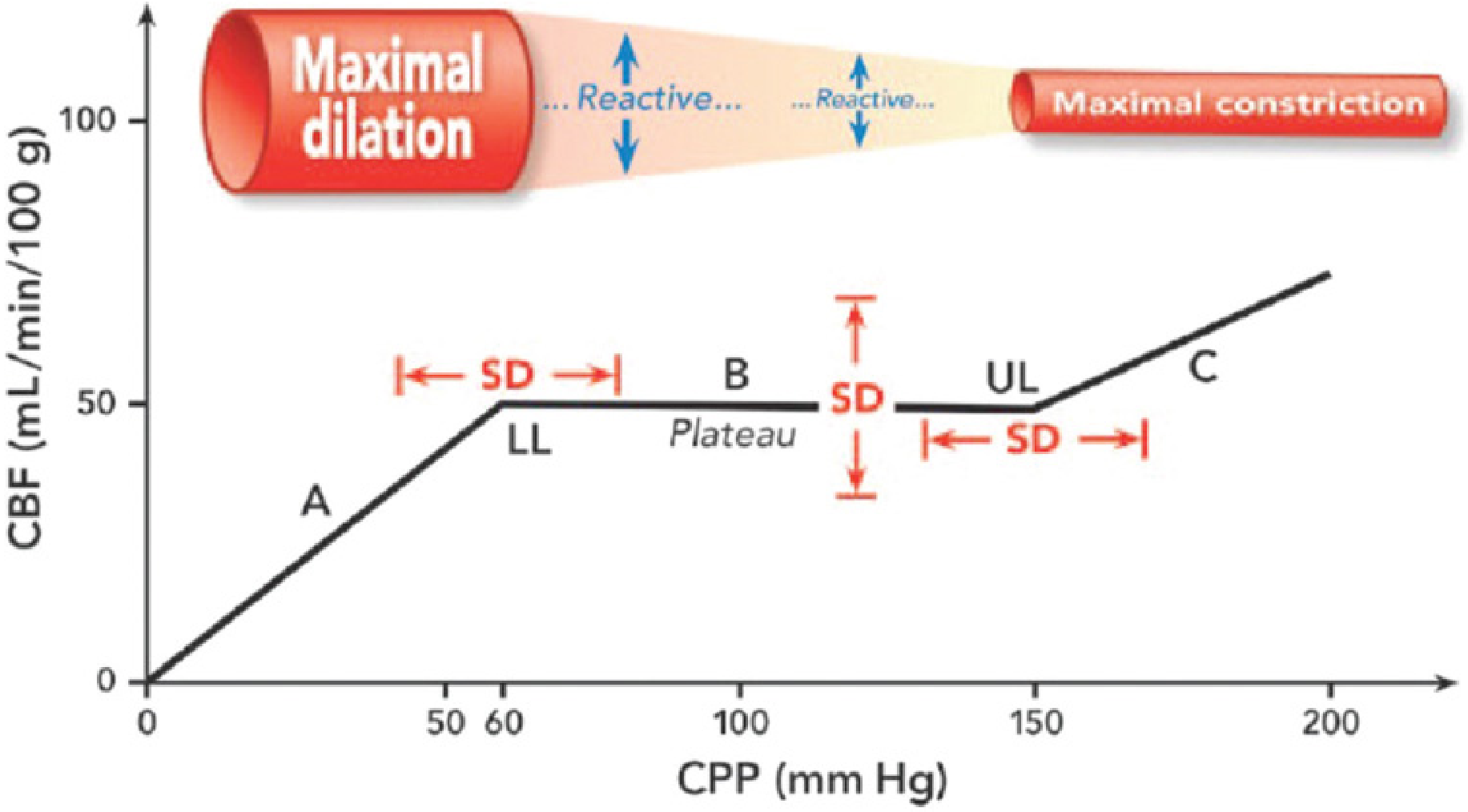
Cerebral autoregulation curve: CBF (mL/min/100 g) on y-axis vs CPP (mm Hg) on x-axis. LL = lower limit (~60 mm Hg), UL = upper limit (~150 mm Hg). SD arrows indicate significant inter-individual variability in both the plateau level and the limits. - Mulholland & Greenfield's Surgery, 7e
The curve has three regions:
| Region | CPP | Vascular response | CBF |
|---|---|---|---|
| A (below LL) | < 50-60 mm Hg | Maximal dilation, capacity exhausted | Pressure-passive (falls with CPP) |
| B (Plateau) | ~60-150 mm Hg | Active vasoconstriction/dilation | Constant (~50 mL/100g/min) |
| C (above UL) | > 150-160 mm Hg | Maximal constriction overcome | Pressure-passive (rises with CPP) |
The response time is rapid: 10-60 seconds after a change in CPP. - Morgan & Mikhail's Clinical Anesthesiology, 7e
Cerebral Perfusion Pressure (CPP)
$$\text{CPP} = \text{MAP} - \text{ICP}$$
Normal CPP = MAP (~95 mm Hg) minus intracranial venous/CSF pressure (<10 mm Hg) = ~85-90 mm Hg. Autoregulation operates between CPP of ~70-150 mm Hg (some sources use MAP 60-160 mm Hg). - Medical Physiology (Boron & Boulpaep)
Mechanisms of Autoregulation
Three mechanisms work in concert:
1. Myogenic Mechanism
- The fundamental basis of pressure autoregulation
- Vascular smooth muscle responds directly to changes in wall tension/intraluminal pressure
- Increased stretch (higher pressure) → vasoconstriction
- Decreased stretch (lower pressure) → vasodilation
- This is the "intrinsic myogenic regulation of vascular tone" - Barash et al., Clinical Anesthesia, 9e
2. Metabolic Mechanism (Flow-Metabolism Coupling)
- Local metabolic byproducts modulate vascular tone
- Low CBF → accumulation of CO2, H+, K+, adenosine, lactate → vasodilation → CBF rises
- High CBF → washout of these metabolites → vasoconstriction
- Involves neurovascular coupling: neurons, astrocytes, and pericytes act as a neurovascular unit
- Glutamate/GABA release from neurons triggers Ca2+ waves in astrocytes
- Astrocytic endfeet contact penetrating arterioles directly
- Release of NO and arachidonic acid metabolites causes vasodilation
- Signal propagates retrograde via gap junctions to pial arteries - Medical Physiology
3. Neurogenic Mechanism
- Sympathetic innervation of cerebral vessels (primarily from the superior cervical ganglion)
- Plays a role in the upper limit of autoregulation - protects against breakthrough hypertension
- Sympathetic activity reduces vasodilatory capacity during hypotension
- Parasympathetic and nitrergic fibers contribute vasodilation
Extrinsic Modifiers of CBF
Carbon Dioxide - The Most Important Extrinsic Factor
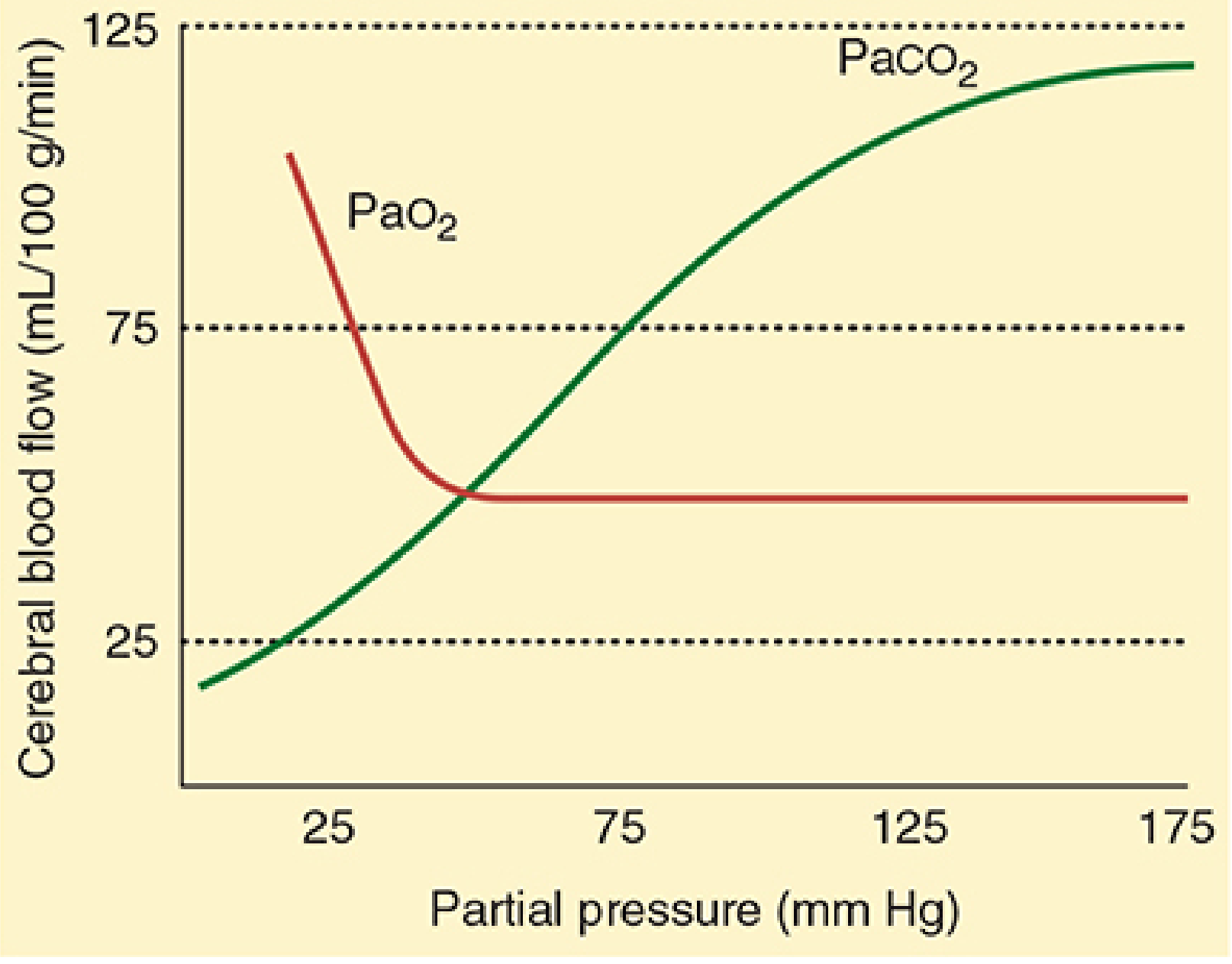
CBF response to PaCO2 (green, linear between 20-80 mm Hg) and PaO2 (red, threshold effect below ~50 mm Hg). - Morgan & Mikhail's Clinical Anesthesiology, 7e
- CBF is directly proportional to PaCO2 between 20-80 mm Hg
- Change in CBF: ~1-2 mL/100g/min per 1 mm Hg change in PaCO2
- Mechanism: CO2 crosses the blood-brain barrier freely; lowers CSF/tissue pH → vasodilation
- Acute metabolic acidosis has little effect (H+ does NOT freely cross the BBB)
- After 24-48 hours, CSF bicarbonate adjusts and the CO2 effect is attenuated
- Both hypercarbia and hypoxia attenuate autoregulation - Morgan & Mikhail; Miller's Anesthesia, 10e
Oxygen
- CBF does not change significantly until PaO2 falls below ~50 mm Hg
- Below this threshold, CBF rises sharply (hypoxic vasodilation)
- Severe hyperoxia can mildly decrease CBF
The Normal Autoregulation Curve (Classic vs. Contemporary View)
The classic view depicted CA as a flat plateau with sharp break-points. The contemporary view (Miller's Anesthesia, 10e) recognizes it as a dynamic process:
- CBF and cerebrovascular tone are under the simultaneous influence of MAP, cardiac output, PaCO2, PaO2, autonomic tone, medications, and anesthetics
- The autoregulatory curve is not static - it reflects the integration of all variables acting on cerebrovascular tone
- There is considerable inter-individual variability in lower limit of autoregulation (LLA), plateau level, and upper limit
- Clinically prudent lower MAP threshold: 70 mm Hg (CPP ~60-65 mm Hg) - Miller's Anesthesia, 10e
Symptoms of cerebral ischemia are not apparent until CBF falls 35-40% below baseline in awake individuals.
Shifts in the Autoregulation Curve
| Condition | Shift | Effect |
|---|---|---|
| Chronic hypertension | Rightward | Both LL and UL shift right; ischemia at "normal" MAP; protected at high MAP |
| Long-term antihypertensive therapy | Back toward normal | Restores autoregulation |
| Volatile anesthetics | Dose-dependent impairment | At high doses, CBF is essentially pressure-passive |
| Acute brain injury / TBI | Loss of autoregulation | ~1/3 of severe TBI patients |
- Morgan & Mikhail's Clinical Anesthesiology, 7e; Mulholland & Greenfield Surgery, 7e
Clinical Conditions Affecting Autoregulation
Traumatic Brain Injury (TBI)
- Autoregulation is disrupted in approximately one-third of patients with severe TBI
- In patients with intact autoregulation: rising MAP causes vasoconstriction → CBF preserved
- In patients with lost autoregulation: rising MAP → cerebral vasodilation → increased cerebral blood volume → elevated ICP
- Target CPP: 60-70 mm Hg for severe TBI patients
- Recovery of autoregulation can be delayed for weeks after TBI - Mulholland & Greenfield Surgery, 7e; Miller's Anesthesia, 10e
Raised ICP and the Cushing Reflex
- Elevated ICP compresses cerebral vasculature → reduces CBF despite autoregulatory vasodilation
- The brain responds via the Cushing reflex: rising ICP → medullary ischemia → increased sympathetic outflow → systemic hypertension (to maintain CPP)
- CPP = MAP - ICP; ICP goal ≤ 22 mm Hg to avoid mortality - Medical Physiology; Mulholland & Greenfield, 7e
Pressure Reactivity Index (PRx)
A continuous bedside monitoring method for assessing the state of autoregulation:
- PRx = correlation coefficient between mean ICP and MAP (calculated continuously)
- PRx near +1: ICP passively follows MAP → autoregulation is absent
- PRx near 0 (e.g., 0.05): ICP independent of MAP → autoregulation is intact
- Used in severe TBI to predict survival and favorable neurological outcome - Mulholland & Greenfield Surgery, 7e
Effects of Anesthetic Agents
| Agent | Effect on Autoregulation |
|---|---|
| Volatile anesthetics (all) | Dose-dependent impairment; CBF becomes pressure-passive at high MAC |
| Sevoflurane | Autoregulation preserved up to ~1 MAC; better preserved at 1.5 MAC than isoflurane |
| Isoflurane/desflurane | Dose-dependent reduction in autoregulation |
| Halothane | Greater impairment of autoregulation than newer volatiles |
| IV agents (propofol, barbiturates) | Generally preserve autoregulation and CO2 reactivity |
| α-stat CPB strategy | Preserves autoregulation until deep hypothermia |
| pH-stat CPB strategy | Impairs autoregulation |
- Barash Clinical Anesthesia, 9e; Morgan & Mikhail, 7e; Miller's Anesthesia, 10e
Summary of Key Values
| Parameter | Normal Value |
|---|---|
| Normal CBF | ~50 mL/100 g/min |
| Autoregulation range (MAP) | 60-160 mm Hg |
| Autoregulation range (CPP) | ~50-150 mm Hg |
| Normal CPP | ~85-90 mm Hg |
| TBI target CPP | 60-70 mm Hg |
| ICP threshold for treatment | >22 mm Hg |
| PaCO2 range for CBF proportionality | 20-80 mm Hg |
| PaO2 threshold for hypoxic vasodilation | <50 mm Hg |
| Time for autoregulatory response | 10-60 seconds |
| CBF drop required for ischemia symptoms | 35-40% below baseline |
Sources: Medical Physiology (Boron & Boulpaep) | Miller's Anesthesia, 10e | Morgan & Mikhail's Clinical Anesthesiology, 7e | Barash Clinical Anesthesia, 9e | Mulholland & Greenfield's Surgery, 7e
This is a shared conversation. Sign in to Orris to start your own chat.