Forest classification Rochelle score Black 4 score Glass glow score
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have all the information needed for a comprehensive answer. These four terms all relate to upper GI bleeding (UGIB) risk stratification and endoscopic classification. The user likely meant Forrest (not "Forest"), Rockall (not "Rochelle"), Blatchford (not "Black 4"), and Glasgow (Blatchford) score. Here is the complete response:
Upper GI Bleeding: Forrest, Rockall, Blatchford & Glasgow-Blatchford Scores
These four tools are used together in the assessment of upper gastrointestinal bleeding (UGIB) - two are endoscopic classification systems and two are clinical risk scores. Here is a breakdown of each:
1. Forrest Classification (Endoscopic)
The Forrest classification categorizes the endoscopic appearance of bleeding peptic ulcers and predicts rebleeding risk. It is widely used in Europe, Asia, and many other regions (descriptive terms are preferred in the USA).
| Class | Endoscopic Finding | Rebleeding Risk (without treatment) |
|---|---|---|
| Ia | Active spurting arterial bleed | ~90% |
| Ib | Active oozing bleed | ~10-27% |
| IIa | Non-bleeding visible vessel (NBVV) | ~50% |
| IIb | Adherent clot | ~33% |
| IIc | Flat pigmented (haematin) spot | ~7% |
| III | Clean-based ulcer | ~3-5% |
Clinical significance:
- Forrest Ia, Ib, IIa = HIGH-RISK stigmata - require endoscopic hemostasis + high-dose IV PPI
- Forrest IIb (adherent clot) = Intermediate risk; endoscopic therapy debated
- Forrest IIc, III = LOW-RISK; outpatient management may be appropriate; oral PPI sufficient
A non-bleeding visible vessel (IIa) that appears translucent or white (pearl-colored) carries a higher rebleeding risk than a dark/pigmented protuberance, as it likely represents the exposed arterial wall rather than a clot.
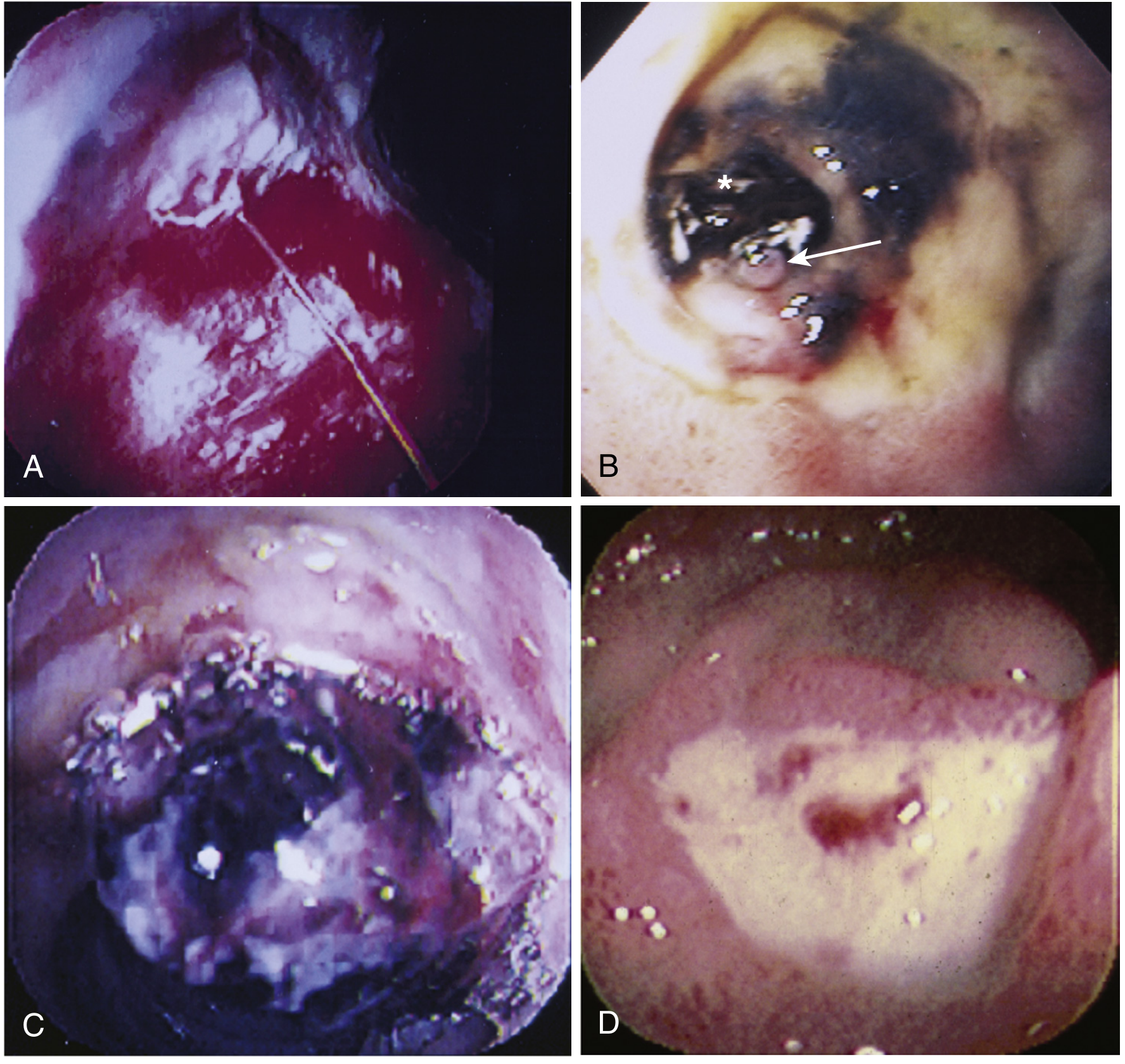
Endoscopic stigmata: A = active spurting (Forrest Ia), B = visible vessel/adherent clot (Forrest IIa/IIb), C = adherent clot (Forrest IIb), D = oozing after wash (Forrest Ib). - Sleisenger & Fordtran's GI and Liver Disease
2. Rockall Score (Pre- and Post-Endoscopy Clinical Risk Score)
The Rockall score predicts rebleeding and mortality after acute UGIB. It has two versions: a pre-endoscopy (clinical) Rockall and a complete (post-endoscopy) Rockall.
| Variable | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|
| Age | <60 yr | 60-79 yr | ≥80 yr | - |
| Shock | None | HR >100 bpm | SBP <100 mmHg | - |
| Comorbidity | None | - | CCF, IHD, other major illness | Renal failure, liver failure, metastatic cancer |
| Endoscopic diagnosis | Mallory-Weiss / no lesion | Peptic ulcer, esophagitis, erosions | UGI malignancy | - |
| Stigmata of recent hemorrhage | Clean base / flat pigmented spot | - | Blood in UGI tract, active bleeding, visible vessel, adherent clot | - |
Interpretation:
-
Clinical Rockall score 0 OR complete Rockall score ≤2 = low risk of rebleeding
-
Score ≥6 = ~50% require endoscopic hemostatic therapy; high mortality risk
-
Maximum score = 11
-
Yamada's Textbook of Gastroenterology, 7th Ed.
3. Glasgow-Blatchford Score / GBS (Pre-Endoscopy Triage Score)
The Glasgow-Blatchford score is a pre-endoscopy score designed to identify patients who need hospital-based intervention (transfusion, endoscopy, or surgery). It is the most widely validated tool and is endorsed by ESGE, International Consensus Group, and Asia-Pacific Working Group guidelines.
| Variable | Points |
|---|---|
| BUN (mmol/L): 6.5-7.9 | 2 |
| BUN 8.0-9.9 | 3 |
| BUN 10.0-24.9 | 4 |
| BUN ≥25 | 6 |
| Hemoglobin (g/dL) - male: 12.0-12.9 | 1 |
| Hgb (male) 10.0-11.9 | 3 |
| Hgb (male) <10 | 6 |
| Hemoglobin (g/dL) - female: 10.0-11.9 | 1 |
| Hgb (female) <10 | 6 |
| SBP (mmHg): 100-109 | 1 |
| SBP 90-99 | 2 |
| SBP <90 | 3 |
| Heart rate ≥100 bpm | 1 |
| Melena | 1 |
| Syncope | 2 |
| Liver disease | 2 |
| Heart failure | 2 |
Interpretation (key thresholds):
- GBS 0-1 = Very low risk; safe for outpatient discharge and close follow-up
- GBS ≥7 = Predicts need for endoscopic intervention (sensitivity 80.4%, NPV 92.4%)
- GBS ≥5 = 88.7% sensitive for 30-day mortality (NPV 97.9%)
The GBS is superior to Rockall and AIMS65 at predicting the combined endpoint of hospital-based intervention or death, making it the preferred pre-endoscopy triage tool.
- Mulholland & Greenfield's Surgery, 7th Ed.; Rosen's Emergency Medicine
4. Glasgow-Blatchford Score vs. Rockall Score - Key Differences
| Feature | Glasgow-Blatchford | Rockall |
|---|---|---|
| Timing | Pre-endoscopy only | Pre- and post-endoscopy versions |
| Purpose | Identify who needs intervention/admission | Predict rebleeding and mortality |
| Best use | Triage/discharge decisions | Prognosis after endoscopy |
| Low-risk threshold | Score ≤1 → safe discharge | Score ≤2 → low rebleeding risk |
| Requires endoscopy? | No | Complete version: Yes |
| Endorsed by guidelines? | ESGE, APAGE, International Consensus | Widely used, but GBS preferred for triage |
Summary: When to Use Each Tool
- Forrest classification - At the time of endoscopy, to grade ulcer stigmata and decide on hemostatic therapy
- Rockall score (clinical) - At presentation, before endoscopy, for early mortality/rebleeding risk stratification
- Glasgow-Blatchford score - At presentation, before endoscopy, to decide who can be safely discharged vs. admitted
- Rockall score (complete) - After endoscopy, to refine prognosis and guide further management
These tools are complementary rather than competing - GBS guides admission/discharge, Forrest guides endoscopic treatment, and Rockall provides overall prognosis.
This is a shared conversation. Sign in to Orris to start your own chat.