Detailed analysis and question answer for coolis fracture
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Colles fracture" management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive, authoritative content from multiple textbooks. Let me compose the full detailed analysis and Q&A.
Colles' Fracture - Detailed Analysis & Question Bank
Definition
A Colles' fracture is a transverse fracture of the distal radial metaphysis, occurring within 2 to 2.5 cm of the articular surface, with:
- Dorsal (backward) displacement and angulation of the distal fragment
- Radial displacement of the carpus
- Proximal displacement (radial shortening)
- Frequently associated fracture of the ulnar styloid
Named after Irish surgeon Abraham Colles, who described it in 1814 - before X-rays existed.
- Rosen's Emergency Medicine, p. 612
- Pye's Surgical Handicraft, p. 189
Epidemiology & Mechanism
- Most common wrist fracture in adults
- Classically affects postmenopausal women (underlying osteoporosis makes it a pathological fracture in this group)
- Mechanism: Fall on an outstretched, extended (dorsiflexed) hand (FOOSH)
- Compression forces on the dorsal side produce dorsal comminution; fracture may extend into the radiocarpal or radioulnar joints ("die-punch" fracture)
Anatomy of Displacement (The "DRAB" Pattern)
| Feature | Direction |
|---|---|
| Distal fragment angulation | Dorsal (backward) |
| Distal fragment displacement | Dorsal + Proximal |
| Radial tilt | Lost (normal volar tilt ~10-15° lost) |
| Radial deviation | Distal fragment displaced radially |
The normal distal radius has:
- ~10-15° volar tilt on lateral view
- ~22-23° radial inclination on AP view
- Radius normally longer than ulna (negative ulnar variance)
Clinical Features
Symptoms
- Pain, swelling, and tenderness at the distal wrist
- Palmar paresthesias (median nerve compression)
- Restricted wrist motion
Signs
- "Dinner fork" deformity - the classic appearance on lateral view: wrist looks like a dinner fork because the hand is displaced dorsally relative to the forearm
- "Garden spade" deformity - appearance on AP view with radial displacement
- Radial deviation of the hand
- Prominent ulnar head (due to radial shortening)
- Tenderness over the distal radius
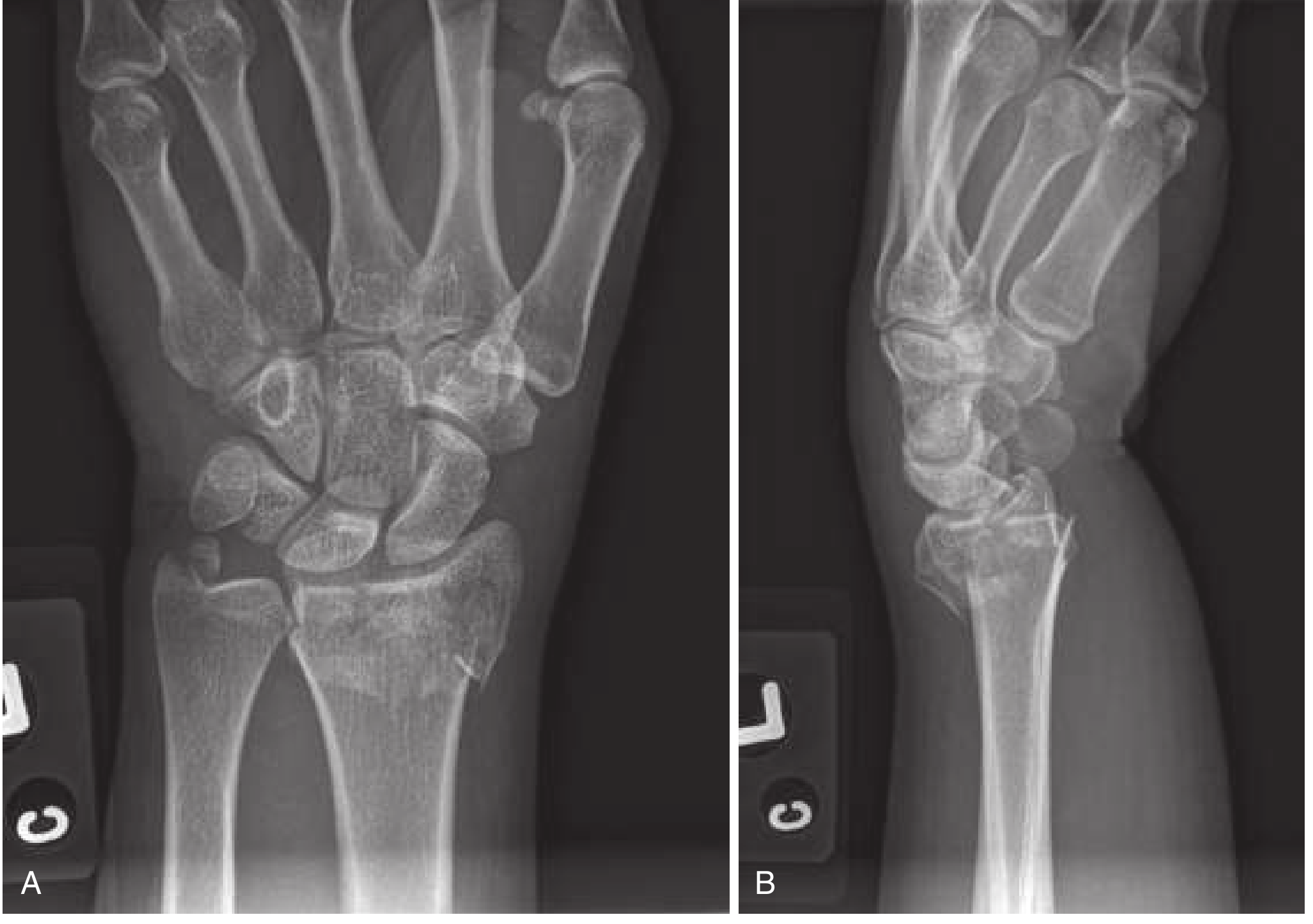
Radiographic Appearance
X-ray findings (Rosen's/Tintinalli):
| View | Finding |
|---|---|
| PA/AP | Fracture line within 2-2.5 cm of articular surface; radial shortening; radial displacement of carpus; possible ulnar styloid fracture; intraarticular extension |
| Lateral | Dorsal angulation of the distal radial articular surface (loss of normal volar tilt); dorsal displacement of distal fragment |
Criteria for UNSTABLE fracture (requiring surgery):
- Dorsal angulation >20 degrees
- Intraarticular involvement
- Marked comminution
- Radial shortening >1 cm (or >5 mm)
- Distal radioulnar joint instability
Classification Systems
(Campbell's Operative Orthopaedics, 15th Ed.)
1. Gartland and Werley (1951)
| Group | Description |
|---|---|
| 1 | Simple Colles fracture |
| 2 | Comminuted Colles fracture, undisplaced intraarticular fragment |
| 3 | Comminuted Colles fracture, displaced intraarticular fragment |
2. Frykman Classification (1967) - 8 types
Based on intraarticular involvement and ulnar styloid fracture:
| Group | Joint involved | Ulnar styloid |
|---|---|---|
| 1 | Extra-articular | Absent |
| 2 | Extra-articular | Present |
| 3 | Radiocarpal joint only | Absent |
| 4 | Radiocarpal joint only | Present |
| 5 | Radioulnar joint only | Absent |
| 6 | Radioulnar joint only | Present |
| 7 | Both joints | Absent |
| 8 | Both joints | Present |
Higher even numbers = worse prognosis. Ulnar styloid fracture in any group increases number by 1.
3. Melone Classification (1986)
| Type | Description |
|---|---|
| 1 | Undisplaced, minimal comminution, stable |
| 2 | Unstable, displacement of medial complex, moderate-severe comminution |
| 3 | Displacement of medial complex + anterior spike |
| 4 | Wide separation or rotation of dorsal and palmar fragments |
4. Fernandez Classification (1987)
| Type | Mechanism |
|---|---|
| 1 | Bending: one cortex fails from tensile stress |
| 2 | Shearing: fracture of joint surface |
| 3 | Compression: joint surface impaction + metaphyseal comminution |
| 4 | Avulsion: ligament attachment fractures, radiocarpal dislocation |
| 5 | Combination: high-velocity injuries |
Management
Step 1: Assessment for Reduction
Reduction is indicated when:
- Lateral X-ray shows dorsal tilt beyond neutral
- Radial shortening (radius not longer than ulna on AP view)
- Dorsal angulation >20 degrees
- Significant displacement
Reduction is NOT indicated for:
- Undisplaced, nondisplaced fractures
- Acceptable alignment (volar tilt neutral or slightly positive)
Step 2: Anesthesia for Reduction
Three options (Rosen's, Pfenninger's):
- Hematoma block (most common, easy method):
- 22-gauge needle inserted dorsally into fracture site
- Aspirate to confirm hematoma
- Inject 5-10 mL of 1-2% lidocaine (with or without bupivacaine)
- Skin surface can be iced or sprayed with ethyl chloride first
- IV regional anesthesia (Bier block)
- Regional nerve blocks (median, radial, ulnar, or brachial plexus)
- Procedural sedation (for very comminuted or difficult fractures)
Step 3: Closed Reduction Technique
(Tintinalli's, Pye's, Rosen's):
- Traction applied to distal fragment to disimpact from proximal fragment
- Use finger traps + countertraction on arm, OR
- Manual traction with assistant holding upper arm
- Re-creation of deformity (increases angulation briefly) to unlock dorsal cortex
- Correction: push distal fragment distally, volarly (anteriorly), and ulnarly using thenar eminence
- Goal: Restore volar tilt (minimum neutral/0°, ideally 10-15° volar), radial inclination, and radius length
Finger traps relax deforming muscle forces, may perform reduction alone, and hold reduction during splinting.
Step 4: Immobilization
- Double sugar-tong splint (one from elbow to wrist, second over it from elbow to axilla) - Pfenninger's / Rosen's
- Immobilization for 4-6 weeks
- Allows finger movement
- Circumferential casting avoided for at least 24 hours (risk of neurovascular compromise from edema)
- If short-arm cast applied, bivalve to allow for swelling
Step 5: Follow-up
- Radiographs at 1, 2, and 6 weeks
- Urgent orthopaedic referral within 2-3 days in most cases
- After cast removal at 6 weeks: if tenderness persists or incomplete union, apply ulnar gutter splint
Indications for Surgery (Operative Management)
- Open fracture
- Neurovascular compromise
- Unstable, severely comminuted, or intra-articular fractures
- Dominant wrist in high-demand (very active) patient
- Failed closed reduction
- Irreducible fractures
Associated Injuries
- Ulnar styloid fracture - occurs in ~60% of Colles' fractures; avulsed by the interarticular disc; disrupts the lower radioulnar joint
- Triangular fibrocartilage complex (TFCC) injury - caused by ulnar styloid avulsion
- Scaphoid fracture (less common, but check)
- Distal radioulnar joint (DRUJ) disruption
- Carpal instability
Complications
(Tintinalli's, Rosen's - complications range from 6-80% of cases)
Early Complications
| Complication | Notes |
|---|---|
| Median nerve injury | Most common nerve injury (17%); carpal tunnel syndrome - immediate or delayed; from contusion, traction, compression after reduction, or cast pressure |
| Radial/ulnar nerve injury | Less common |
| DRUJ instability | Disruption of lower radioulnar joint |
| Compartment syndrome (ACTS) | Rare but serious |
| Malreduction | Inadequate fracture reduction |
Late Complications
| Complication | Notes |
|---|---|
| Malunion | Most common late complication; causes weak, stiff, painful wrist |
| Carpal tunnel syndrome | Median nerve compression |
| Post-traumatic arthritis | Especially with intraarticular fractures |
| TFCC injuries | Lead to radioulnar instability |
| Radiocarpal instability | |
| Stiffness and weakness | Common |
| Reflex sympathetic dystrophy (CRPS) | Rare but debilitating |
| Extensor pollicis longus (EPL) rupture | Due to attritional wear over dorsal tubercle |
Factors predicting poor outcome/instability:
- Dorsal angulation ≥20 degrees
- Radial shortening ≥5 mm
- Intraarticular extension
- Significant comminution
- Older age
Colles' vs. Smith's vs. Barton's Fractures
| Feature | Colles' | Smith's | Barton's |
|---|---|---|---|
| Also known as | - | Reverse Colles' | - |
| Angulation | Dorsal | Volar | Intraarticular shear |
| Displacement | Dorsal + proximal | Volar + proximal | Marginal rim |
| Mechanism | FOOSH (wrist extended) | Fall on dorsum of hand / wrist flexed | Shearing force |
| Deformity | Dinner fork | Garden spade (reverse) | - |
| Stability | Often reducible | More unstable, often needs surgery | Often needs surgery |
Question Bank (Exam-Style Q&A)
Q1. What is the most common wrist fracture in adults?
A: Colles' fracture - a dorsally displaced/angulated fracture of the distal radial metaphysis within 2-2.5 cm of the articular surface.
Q2. Describe the mechanism of a Colles' fracture.
A: Fall on an outstretched, extended (dorsiflexed) hand (FOOSH). Axial compressive force with wrist in extension causes failure of the distal radial metaphysis.
Q3. What classic deformity is seen in Colles' fracture?
A: "Dinner fork" deformity - on lateral view, the dorsal displacement of the distal fragment makes the wrist profile resemble an upturned dinner fork. On AP view, radial deviation of the hand gives a "garden spade" appearance.
Q4. Which nerve is most commonly injured in Colles' fracture?
A: The median nerve (injured in ~17% of cases), causing carpal tunnel syndrome - either acutely from displacement or late from swelling/fibrosis. Always check motor and sensory function before and after reduction.
Q5. What are the radiographic criteria for an UNSTABLE Colles' fracture?
A:
- Dorsal angulation >20 degrees
- Intraarticular extension (radiocarpal or radioulnar joint)
- Marked comminution
- Radial shortening >1 cm (or >5 mm)
- DRUJ instability
Q6. Describe the Frykman classification of distal radial fractures.
A: 8 types based on:
- Intraarticular involvement (radiocarpal, radioulnar, or both)
- Associated ulnar styloid fracture (adds 1 to the type number) Types 1-2 = extra-articular, Types 3-8 = intra-articular. Higher even numbers = worse prognosis.
Q7. What is the technique of a hematoma block for Colles' fracture reduction?
A: Insert a 22-gauge needle dorsally into the fracture site, aspirate to confirm entry into hematoma, then inject 5-10 mL of 1-2% lidocaine (± bupivacaine for longer duration). Avoids the need for procedural sedation and reduces ED length of stay.
Q8. What is the treatment goal for closed reduction of Colles' fracture?
A: Restore:
- Volar tilt (minimum 0°/neutral, ideally 10-15° volar)
- Radial inclination (~22°)
- Radius length (negative ulnar variance or radius equal to ulna)
Q9. What splint is used after Colles' fracture reduction?
A: Double sugar-tong splint - immobilizes the wrist while allowing finger movement. Circumferential casting is avoided for at least 24 hours due to swelling-related neurovascular risk.
Q10. What are the indications for surgical management?
A:
- Open fracture
- Neurovascular compromise
- Unstable/comminuted/intra-articular fractures not reducible by closed methods
- High-demand patient (dominant wrist)
- Failed closed reduction
Q11. What is Smith's fracture? How does it differ from Colles'?
A: Smith's fracture (reverse Colles') is a fracture of the distal radius with volar angulation and displacement - the opposite of Colles'. Caused by fall on a flexed wrist or direct blow on the dorsum of the hand. More likely to be unstable and require surgery than Colles'.
Q12. What associated injury occurs in ~60% of Colles' fractures?
A: Ulnar styloid fracture, caused by avulsion via the interarticular disc. This disrupts the lower radioulnar joint and the TFCC, and is a common source of long-term morbidity.
Q13. What is the most common LATE complication of Colles' fracture?
A: Malunion - results in a weak, stiff, and painful wrist. Factors predicting malunion and poor outcome include dorsal angulation ≥20° and radial shortening ≥5 mm.
Q14. In which population is Colles' fracture considered a pathological fracture?
A: Postmenopausal women with osteoporosis - the underlying bone fragility means the fracture occurs at a force that would not break normal bone.
Q15. What is periosteal entrapment in Colles' fracture and how is it corrected?
A: The periosteum folds into the fracture site, blocking anatomic reduction and disrupting blood supply. Correction requires re-creating the mechanism of injury (brief re-angulation) then reversing the mechanism under traction to unfold and release the periosteum.
Sources used:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, pp. 612-613
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, pp. 1847-1848
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed., pp. 1321-1322
- Pye's Surgical Handicraft, 22nd Ed., pp. 189-190
- Campbell's Operative Orthopaedics, 15th Ed. (2026), Classification section
Detailed analysis and question answer for cooles fracture
I already provided a comprehensive analysis of Colles' fracture in my previous response. Here's the complete reference — no need to re-research since this is the same topic (your spelling "cooles" = Colles').
Colles' Fracture — Complete Analysis & Question Bank
Definition
A Colles' fracture is a transverse fracture of the distal radial metaphysis, occurring within 2 to 2.5 cm of the articular surface, with:
- Dorsal (backward) displacement and angulation of the distal fragment
- Radial displacement of the carpus
- Proximal displacement (radial shortening)
- Frequently associated ulnar styloid fracture
Named after Irish surgeon Abraham Colles (1814) - described before X-rays existed.
Epidemiology & Mechanism
- Most common wrist fracture in adults
- Classically affects postmenopausal women (osteoporotic bone = pathological fracture in this group)
- Mechanism: Fall on an outstretched, extended (dorsiflexed) hand - FOOSH
- Compression forces on the dorsal side produce dorsal comminution
- Fracture may extend into radiocarpal or radioulnar joints ("die-punch" fracture)
The Four Classic Displacement Features (DRAB)
| Feature | Direction |
|---|---|
| Displacement | Dorsal + proximal |
| Radial shortening | Yes (radius shorter than ulna) |
| Angulation | Dorsal (backward tilt) |
| Backward radial deviation | Hand displaced radially |
Normal distal radius values (which are lost):
- Volar tilt: ~10-15° on lateral view
- Radial inclination: ~22-23° on AP view
- Radius normally longer than ulna (negative ulnar variance)
Clinical Features
Deformities
- "Dinner fork" deformity - lateral view: hand displaced dorsally relative to forearm, resembling an upturned dinner fork
- "Garden spade" deformity - AP view: radial deviation of hand
- Prominent ulnar head (from radial shortening)
- Swelling, ecchymosis, point tenderness over distal radius
Neurological
- Palmar paresthesias from median nerve compression (most common nerve affected, ~17%)
- Always assess neurovascular status before and after reduction
Radiographic Findings
| View | Findings |
|---|---|
| PA/AP | Fracture within 2-2.5 cm of joint; radial shortening; radial carpal displacement; possible ulnar styloid fracture; intraarticular extension |
| Lateral | Dorsal angulation of distal radial articular surface; loss of normal volar tilt; dorsal fragment displacement |
Criteria for UNSTABLE Fracture
- Dorsal angulation >20 degrees
- Intraarticular extension (radiocarpal or radioulnar)
- Marked comminution
- Radial shortening >5 mm to 1 cm
- DRUJ instability
Classification Systems
(Campbell's Operative Orthopaedics, 15th Ed. 2026)
1. Gartland and Werley (1951)
| Group | Description |
|---|---|
| 1 | Simple Colles fracture |
| 2 | Comminuted, undisplaced intraarticular fragment |
| 3 | Comminuted, displaced intraarticular fragment |
2. Frykman Classification (1967) - Most used
8 types based on two variables:
- Intraarticular involvement (radiocarpal / radioulnar / both)
- Presence or absence of ulnar styloid fracture (adds 1 to type number)
| Group | Joint Involvement | Ulnar Styloid |
|---|---|---|
| 1 | Extra-articular | Absent |
| 2 | Extra-articular | Present |
| 3 | Radiocarpal only | Absent |
| 4 | Radiocarpal only | Present |
| 5 | Radioulnar only | Absent |
| 6 | Radioulnar only | Present |
| 7 | Both joints | Absent |
| 8 | Both joints | Present |
Higher even numbers = worst prognosis. Type 8 = most severe.
3. Melone Classification (1986)
| Type | Description |
|---|---|
| 1 | Undisplaced, minimal comminution, stable |
| 2 | Unstable, medial complex displaced, moderate-severe comminution |
| 3 | Medial complex displaced as unit + anterior spike |
| 4 | Wide separation/rotation of dorsal and palmar fragments |
4. Fernandez Classification (1987)
| Type | Mechanism | Description |
|---|---|---|
| 1 | Bending | One cortex fails from tensile stress; opposite cortex comminuted |
| 2 | Shearing | Fracture of joint surface |
| 3 | Compression | Joint surface impaction with metaphyseal comminution |
| 4 | Avulsion | Ligament attachment fractures; radiocarpal dislocation |
| 5 | Combination | High-velocity injuries |
Management
Step 1 - Assess Need for Reduction
Reduction REQUIRED when:
- Dorsal tilt beyond neutral on lateral X-ray
- Radius shorter than ulna on AP (positive ulnar variance)
- Dorsal angulation >20°
- Significant displacement
Reduction NOT required when:
- Undisplaced or nondisplaced
- Volar tilt neutral or slightly positive
- No significant shortening
Step 2 - Anesthesia
| Method | Details |
|---|---|
| Hematoma block (easiest) | 22-gauge needle dorsal to fracture site; aspirate hematoma; inject 5-10 mL 1-2% lidocaine ± bupivacaine |
| Bier block (IV regional) | Good for prolonged procedures |
| Regional nerve blocks | Median, radial, ulnar, or brachial plexus |
| Procedural sedation | For very comminuted/difficult fractures |
The hematoma block avoids procedural sedation and reduces ED length of stay.
Step 3 - Reduction Technique
- Apply traction to distal fragment (via finger traps + countertraction, or manual)
- Disimpact the fragment from proximal radius
- Re-create deformity briefly to unlock dorsal cortex (if periosteal entrapment present)
- Push distal fragment: distally + volarly (anteriorly) + ulnarly
- Use thenar eminence of operator to mold fragment into position
Finger traps relax deforming muscle spasm, may complete reduction alone, and hold alignment during splinting.
Goal of reduction:
- Restore volar tilt (minimum 0°/neutral, ideally 10-15° volar)
- Restore radial inclination (~22°)
- Restore radial length (negative ulnar variance)
Step 4 - Immobilization
- Double sugar-tong splint: first from elbow to wrist; second over it from elbow to axilla
- Allows finger movement
- Immobilization for 4-6 weeks
- No circumferential casting for at least 24 hours (edema risk)
- If short-arm cast applied, bivalve it
Step 5 - Follow-up
- X-rays at 1, 2, and 6 weeks
- Urgent orthopaedic referral within 2-3 days
- At 6 weeks: assess union; if incomplete, continue splinting
Indications for Surgery
- Open fracture
- Neurovascular compromise
- Unstable / severely comminuted / intraarticular fractures
- Failed or irreducible closed reduction
- Dominant wrist of high-demand/active patient
- Fractures with >5 mm articular step-off
Associated Injuries
| Injury | Notes |
|---|---|
| Ulnar styloid fracture | ~60% of cases; TFCC avulsion; disrupts DRUJ |
| TFCC injury | Triangular fibrocartilage complex tear |
| DRUJ disruption | Lower radioulnar joint instability |
| Carpal instability | Scapholunate ligament injury |
| Median nerve injury | Most common nerve, 17% |
Complications
Immediate
| Complication | Notes |
|---|---|
| Median nerve injury | Most common; acute carpal tunnel syndrome |
| Malreduction | Most common reason for re-intervention |
| Neurovascular compromise | From tight cast/splint |
| Compartment syndrome | Rare |
Late
| Complication | Notes |
|---|---|
| Malunion | Most common late complication; weak, stiff, painful wrist |
| Carpal tunnel syndrome | Delayed median nerve compression |
| Post-traumatic arthritis | Especially with intraarticular fractures |
| DRUJ instability | Chronic wrist pain and weakness |
| EPL rupture | Extensor pollicis longus rupture over Lister's tubercle |
| CRPS (Reflex Sympathetic Dystrophy) | Rare but severe |
| Radiocarpal instability | |
| Stiffness / weakness | Very common |
Predictors of poor outcome:
- Dorsal angulation ≥20°
- Radial shortening ≥5 mm
- Intraarticular involvement
- Severe comminution
- Older age with osteoporosis
Colles' vs Smith's vs Barton's - Comparison Table
| Feature | Colles' | Smith's | Barton's |
|---|---|---|---|
| Nickname | - | Reverse Colles' | - |
| Angulation | Dorsal | Volar | Marginal shear |
| Displacement | Dorsal + proximal | Volar + proximal | Intraarticular rim |
| Mechanism | FOOSH (wrist extended) | Fall on flexed wrist | Shearing force |
| Deformity | Dinner fork | Garden spade (reverse) | None specific |
| Stability | Usually reducible | More unstable | Usually needs surgery |
| Treatment | Closed reduction ± surgery | Often needs surgery | Usually surgery |
Exam-Style Question & Answer Bank
Q1. What is the definition and site of Colles' fracture?
A: Transverse fracture of the distal radial metaphysis within 2-2.5 cm of the articular surface with dorsal displacement, dorsal angulation, radial displacement, and radial shortening.
Q2. What is the mechanism of injury?
A: Fall on an outstretched, extended (dorsiflexed) hand (FOOSH). Axial load with wrist in extension drives the distal radius to fracture dorsally.
Q3. Who classically gets Colles' fracture and why?
A: Postmenopausal women - osteoporosis makes the distal radius fragile, so it fractures from a low-energy fall. It is effectively a pathological fracture in this population.
Q4. Name the two classic deformities.
A:
- Dinner fork deformity (lateral view) - dorsal displacement of hand relative to forearm
- Garden spade deformity (AP view) - radial deviation of the hand
Q5. Which nerve is most commonly injured? What are the mechanisms?
A: Median nerve (~17%). Mechanisms include: acute contusion/traction from displacement, compression after closed reduction, overlying cast pressure, or secondary carpal tunnel syndrome from swelling/fibrosis.
Q6. What are the radiographic features on the lateral X-ray?
A: Dorsal angulation of the distal radial articular surface (loss of normal 10-15° volar tilt); dorsal and proximal displacement of the distal fragment. The deformity creates the dinner fork appearance.
Q7. What fracture is associated with 60% of Colles' fractures?
A: Ulnar styloid fracture - avulsed by the interarticular disc (which remains attached to the displaced distal radius fragment). This disrupts the DRUJ and TFCC and is a common source of chronic morbidity.
Q8. Describe the Frykman classification.
A: 8 groups based on:
- Intraarticular involvement: none (1-2), radiocarpal (3-4), radioulnar (5-6), both (7-8)
- Even numbers = associated ulnar styloid fracture
- Higher number = worse prognosis; Group 8 is the most severe
Q9. What are the criteria for an unstable Colles' fracture?
A: Dorsal angulation >20°, intraarticular involvement, marked comminution, radial shortening >5 mm-1 cm, DRUJ instability. These predict loss of reduction and need for surgery.
Q10. How is a hematoma block performed?
A: Insert 22-gauge needle dorsally into fracture site, withdraw until fracture hematoma is aspirated, then inject 5-10 mL of 1-2% lidocaine (± bupivacaine). Avoids procedural sedation; easy and effective in ED.
Q11. Describe the steps of closed reduction.
A:
- Apply traction (finger traps or manual) to disimpact fragment
- Re-create deformity if periosteal entrapment suspected
- Push distal fragment distally + volarly + ulnarly
- Mold and hold while applying splint
- Goal: restore volar tilt (≥0°), radial inclination, and radial length
Q12. What splint is applied after reduction and why not a full cast?
A: Double sugar-tong splint - immobilizes wrist but allows fingers to move. Circumferential casting avoided for ≥24 hours because post-injury edema can cause neurovascular compromise inside a rigid cast.
Q13. What is periosteal entrapment and how does it affect reduction?
A: The periosteum folds into the fracture gap, blocking anatomic reduction and disrupting periosteal blood supply. Corrected by re-creating the mechanism of injury under traction (briefly increasing angulation) to unfold the periosteum, then reversing.
Q14. What are the indications for operative management?
A: Open fracture, neurovascular compromise, irreducible/unstable/intraarticular fractures, failed closed reduction, dominant wrist of high-demand patient, articular step-off >2 mm.
Q15. What is the most common late complication?
A: Malunion - results in a stiff, weak, painful wrist. Factors predicting malunion: dorsal angulation ≥20° and radial shortening ≥5 mm.
Q16. What is EPL rupture and when does it occur in Colles' fracture?
A: Rupture of the extensor pollicis longus tendon over Lister's tubercle on the dorsum of the distal radius. Occurs as a late attritional complication (weeks to months after fracture), even after undisplaced fractures. Presents as inability to extend the interphalangeal joint of the thumb.
Q17. How does Colles' fracture differ from Smith's fracture?
A: Smith's fracture = reverse Colles'. Caused by fall on a flexed wrist or blow on dorsum. Distal fragment is displaced volarly (not dorsally). More unstable - often requires surgery. Treated in a sugar-tong splint after reduction, but surgical fixation is more frequently needed.
Q18. What is the Fernandez Type 1 Colles' fracture?
A: A bending fracture where one cortex (dorsal) fails under tensile stress while the opposite (volar) cortex may show some comminution. This is the classic simple Colles' mechanism from a FOOSH.
Q19. What follow-up schedule is used for Colles' fracture after splinting?
A: X-rays at 1 week (splint removed), 2 weeks, and 6 weeks (after cast removal). Orthopaedic referral within 2-3 days for reduced fractures. At 6 weeks, if union incomplete, apply ulnar gutter splint with range-of-motion exercises.
Q20. What percentage of Colles' fractures develop complications?
A: Complications occur in 6-80% of cases (Tintinalli's). Higher rates with open fractures, displaced fractures, and older patients with osteoporosis.
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed.
- Pye's Surgical Handicraft, 22nd Ed.
- Campbell's Operative Orthopaedics, 15th Ed. (2026)
This is a shared conversation. Sign in to Orris to start your own chat.