Pseudomembrane collitis
Reading File
Finding Sources
Searching PubMed
"pseudomembranous colitis" OR "Clostridioides difficile colitis"
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Now I have comprehensive information. Let me compile the full answer.
Pseudomembranous Colitis
Definition
Pseudomembranous colitis (PMC) is a severe form of Clostridioides difficile infection (CDI) — the most common health care-associated diarrheal illness. It is characterized by the formation of pseudomembranes on the colonic mucosa resulting from toxin-mediated mucosal injury. While other organisms (Salmonella, C. perfringens type A, S. aureus) can cause antibiotic-associated diarrhea, only C. difficile causes pseudomembrane formation.
Etiology
| Feature | Detail |
|---|---|
| Organism | Clostridioides difficile — obligate anaerobe, gram-positive, spore-forming bacillus |
| Reservoir | Environmental surfaces, hospital settings; spores persist for months |
| Transmission | Fecal–oral via spore ingestion; hands of healthcare workers |
| Colonization rate | 1–3% community; up to 20–30% of hospitalized adults |
Risk Factors
- Antibiotic use — nearly any antibiotic; highest risk with clindamycin, 2nd/3rd-gen cephalosporins, fluoroquinolones
- Age >65 years
- Hospitalization / nursing home residence
- Gastrointestinal surgery
- Immunosuppression
- Proton pump inhibitor use (modest risk, especially if already on antibiotics)
- Enteral tube feeding
Pathogenesis
Three events are required for CDI to develop:
- Antibiotic exposure → disrupts normal colonic microbiota, creating colonization susceptibility
- Exposure to toxigenic C. difficile → spores survive gastric acid, germinate in small bowel, colonize the colon
- Host factors → inadequate immune response (low IgG anti-toxin A/B), virulent strain (e.g., NAP1/BI/027)
Toxins
| Toxin | Type | Mechanism |
|---|---|---|
| Toxin A | Enterotoxin | Potent neutrophil chemoattractant; glucosylates Rho GTPases |
| Toxin B | Cytotoxin | Primary virulence factor; glucosylates Rho GTPases → disrupts actin cytoskeleton → tight junction loss, fluid leakage |
| Binary toxin (CDT) | — | Present in hypervirulent NAP1/BI/027 strain; role in pathogenesis still being defined |
Downstream effects: epithelial cytoskeletal disruption → tight junction barrier loss → cytokine release → apoptosis → neutrophil infiltration → pseudomembrane formation.
Morphology
Gross / Endoscopic
- Pseudomembranes begin as 1–2 mm whitish-yellow plaques on colonic mucosa
- Intervening mucosa initially appears normal
- Progress to confluent plaques coating the entire colon wall
- Whole colon involved; ~10% show rectal sparing
- Terminal ileum typically spared
Histology — Pathognomonic "Volcano Lesion"
- Surface epithelium is denuded
- Superficial lamina propria: dense neutrophil infiltrate + fibrin thrombi in capillaries
- Damaged crypts distended by mucopurulent exudate that erupts through the surface — the classic "volcanic eruption" pattern
- Pseudomembranes = adherent layer of necrotic leukocytes, fibrin, mucus, and cellular debris
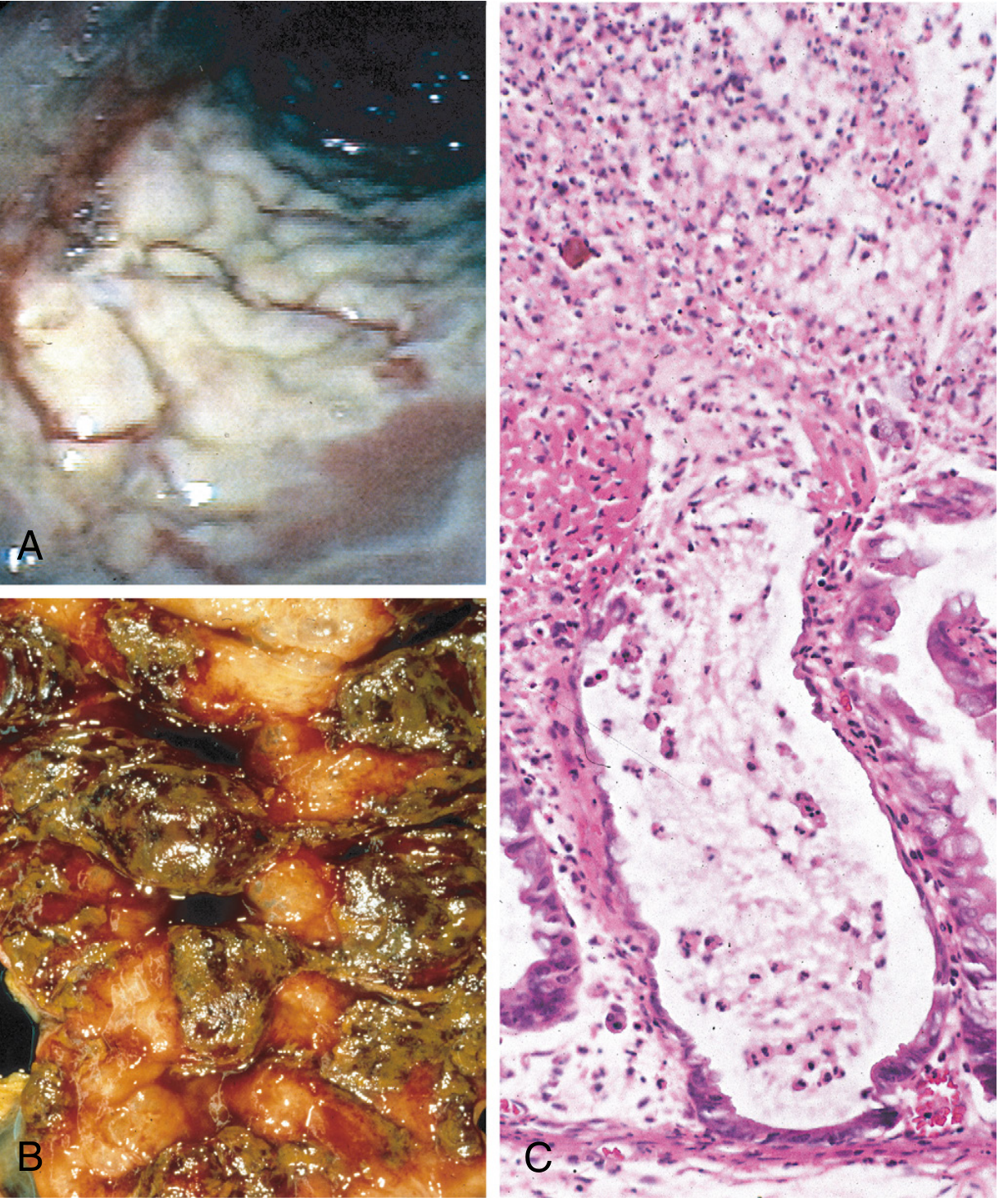
Fig. from Robbins, Cotran & Kumar Pathologic Basis of Disease — (A) Endoscopic view of gray pseudomembranes. (B) Gross specimen. (C) Volcano lesion: neutrophils erupting from a damaged, dilated crypt.
Clinical Features
| Symptom/Sign | Notes |
|---|---|
| Watery diarrhea | Most common presenting symptom |
| Abdominal cramping / pain | Common |
| Fever + leukocytosis | Especially in severe disease |
| Dehydration | Significant in moderate-severe disease |
| Hypoalbuminemia | From protein loss in severe cases |
| Fecal leukocytes / occult blood | May be present |
| Grossly bloody diarrhea | Uncommon |
Fulminant CDI
- May present WITHOUT diarrhea — mimics acute surgical abdomen
- Sepsis (hypotension, fever, tachycardia, leukocytosis ≥20,000 WBCs/μL)
- Toxic megacolon — potentially fatal
- CT abdomen: colon-wall thickening, ileus, ascites
Diagnosis
- Nucleic acid amplification test (NAAT) — highly sensitive; positive NAAT alone = colonization
- Stool toxin assay — both NAAT positive + toxin positive = CDI (symptomatic disease)
- Sigmoidoscopy/colonoscopy — to visualize pseudomembranes (especially in fulminant disease without diarrhea)
- Abdominal CT — for fulminant/surgical abdomen presentations
Treatment
Non-severe / Initial Episode
| Agent | Notes |
|---|---|
| Vancomycin (oral) | First-line for non-severe and severe CDI |
| Fidaxomicin | Preferred; lower recurrence rate than vancomycin |
| Metronidazole | No longer recommended as first-line; not for recurrent CDI |
Severe / Fulminant CDI
- Oral vancomycin + IV metronidazole (for ileus/inability to deliver oral therapy)
- Vancomycin per retention enema
- Surgical colectomy if no response to medical therapy — perform before serum lactate reaches 5 mmol/L
Recurrent CDI (~15–40% of patients)
- Fidaxomicin (superior to vancomycin for recurrence prevention)
- Vancomycin in tapering/pulsed regimen
- Fecal Microbiota Transplantation (FMT) — highly effective for recurrent disease; available as nasoduodenal tube, colonoscope, enema, or oral capsules
- FDA-approved microbiota products: Rebyota (live-jslm, suspension) and Vowst (live-brpk, oral spore suspension)
- Bezlotoxumab — monoclonal antibody against toxin B; adjunctive agent that reduces recurrence risk by ~10% absolute in high-risk patients
Complications
| Complication | Note |
|---|---|
| Toxic megacolon | Marked colonic wall injury; potentially fatal |
| Colonic perforation | Surgical emergency |
| Sepsis / septic shock | Especially in fulminant disease |
| Recurrent CDI | Up to 40%; each recurrence increases risk of further episodes |
Key Points Summary
- PMC is the severe end of C. difficile infection, defined by pseudomembrane formation on colonoscopy/pathology
- Pathognomonic histology: "volcano lesion" — mucopurulent exudate erupting from dilated crypts
- Toxin B is the primary virulence factor; toxin A is a potent neutrophil chemoattractant
- Antibiotic disruption of the microbiome is the essential first step
- Fidaxomicin is preferred over vancomycin for lower recurrence
- FMT is increasingly accepted for recurrent disease, with two FDA-approved commercial products now available
Sources: Harrison's Principles of Internal Medicine 22E (2025); Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.