Hbsag positive pregnancy management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hepatitis B" AND pregnancy AND management
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading Article
I now have all the information needed to compile a thorough, well-structured answer. Here is the complete management guide:
HBsAg-Positive Pregnancy: Management
Overview of the Two Goals
Management of hepatitis B in pregnancy runs along two parallel tracks:
- Maternal health - assess disease activity and treat if indicated
- Prevention of mother-to-child transmission (MTCT) - the primary driver of chronic HBV globally
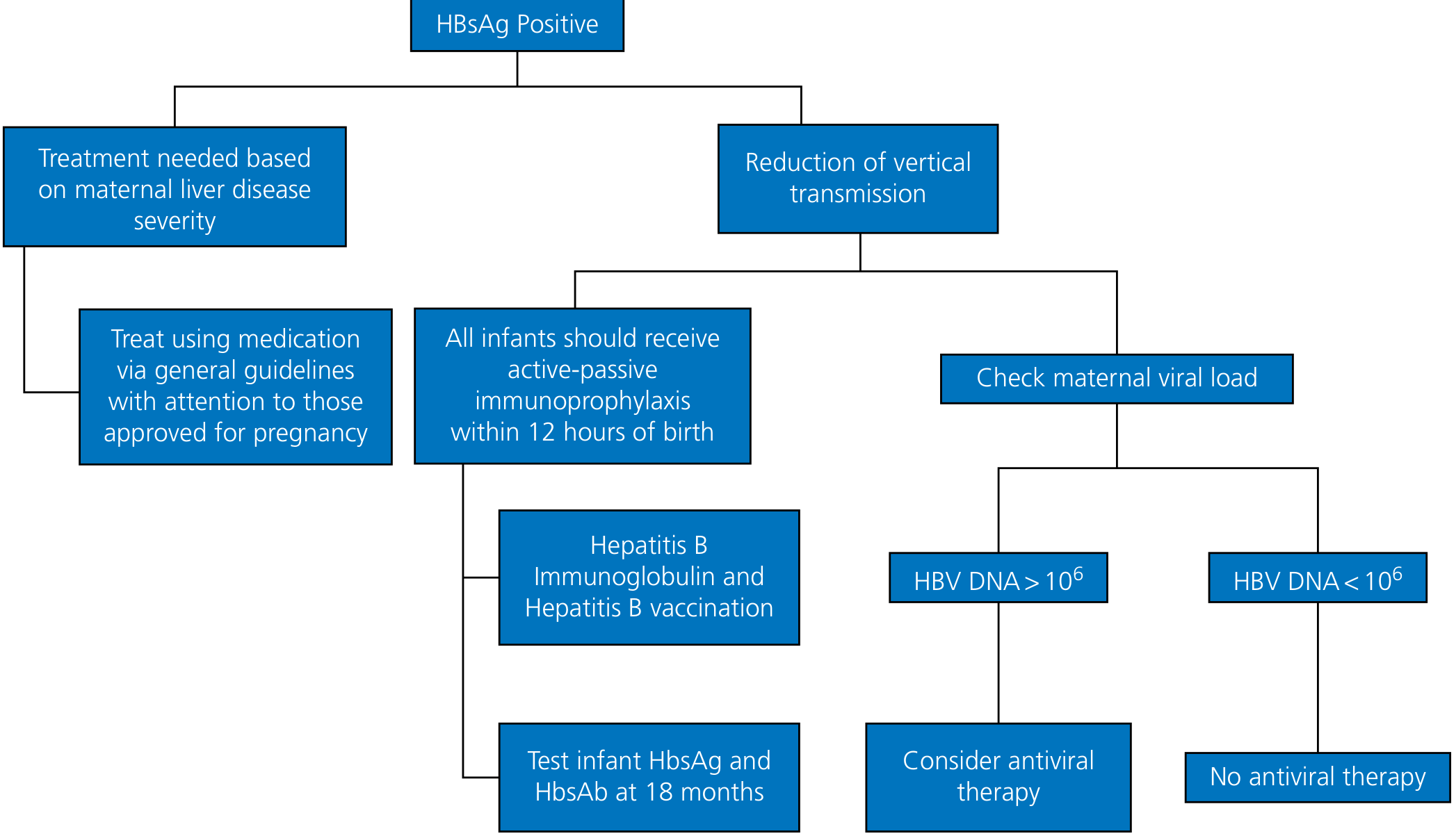
Figure: Management algorithm for HBsAg-positive pregnancy
1. Screening
- All pregnant women should be tested for HBsAg at their first prenatal visit, regardless of prior vaccination history.
- HBsAg-negative women at high risk (IV drug use, multiple sexual partners) or with clinical hepatitis should be re-tested at delivery admission.
- HBsAg-negative, high-risk women should be offered HBV vaccination - it is safe in pregnancy (except Heplisav-B, which lacks pregnancy safety data).
- Red Book 2021, p. 635-636
2. Initial Evaluation of HBsAg-Positive Mother
Once HBsAg positivity is confirmed, order:
| Test | Purpose |
|---|---|
| HBeAg | Marker of active replication; HBeAg+ = higher MTCT risk (70-90%) |
| HBV DNA | Quantifies viral load; key for antiviral decision |
| LFTs (ALT/AST) | Assess liver injury |
| HBsAb, HBcAb | Confirm infection vs. immunity status |
| Liver imaging/fibroscan | If cirrhosis suspected |
- HBeAg-negative mothers still carry 5-20% MTCT risk.
- High viral load (HBV DNA >200,000 IU/mL) is associated with immunoprophylaxis failure.
- Yamada's Textbook of Gastroenterology, p. 834
3. Antiviral Therapy in Pregnancy
When to treat
A. For maternal disease - Use the same general chronic HBV treatment criteria (active hepatitis, elevated ALT, significant fibrosis), adapted for pregnancy safety.
B. To reduce MTCT - Antiviral therapy in the late second or early third trimester is recommended for mothers with HBV DNA >200,000 IU/mL (AASLD guideline threshold) or equivalently >10^6 IU/mL by some guidelines.
Preferred agent
| Drug | Recommendation |
|---|---|
| Tenofovir disoproxil fumarate (TDF) | First choice - best safety data, low resistance risk, proven MTCT reduction |
| Tenofovir alafenamide (TAF) | Fewer bone/renal side effects but limited pregnancy data; use with caution |
| Lamivudine / Telbivudine | Effective but high resistance risk - not preferred |
| Entecavir | Limited pregnancy data; switch to TDF if patient is on entecavir before or during pregnancy |
| Interferon-alpha | Contraindicated in pregnancy - significant maternal side effects and fetal risk |
- TDF is classified pregnancy category B; antiretroviral registry data support its safety.
- Treatment is typically started in the third trimester and can be stopped shortly after delivery (some stop at delivery, some continue 4-12 weeks postpartum).
- Yamada's Textbook of Gastroenterology, p. 834-835
Note: A 2023 multicenter double-blind RCT raised questions about whether maternal TDF provides incremental benefit above strict immunoprophylaxis given within ~1 hour of birth. AASLD still recommends antiviral therapy for high-viral-load mothers, but this is an evolving area.
4. Obstetric Considerations
- Mode of delivery: Vaginal delivery is acceptable - cesarean section is not routinely recommended solely to prevent MTCT, as intrapartum transmission risk is not clearly reduced by C-section when immunoprophylaxis is given.
- Invasive procedures: Amniocentesis and chorionic villus sampling carry a theoretical risk of fetal exposure; discuss risks carefully if needed.
- Breastfeeding: Allowed once the neonate receives immunoprophylaxis (HBsAg vaccine + HBIG). HBV is present in breast milk, but passive-active immunoprophylaxis is protective.
- Fetal outcomes: Chronic HBV does not significantly increase risk of congenital malformations or spontaneous abortion. Some studies note modestly higher rates of gestational diabetes, antepartum hemorrhage, and preterm labor. Acute HBV in the third trimester carries the highest MTCT risk (60-90%).
- Yamada's Textbook of Gastroenterology, p. 835
5. Postpartum Monitoring of the Mother
- Nearly two-thirds of mothers experience an ALT flare postpartum as cortisol drops and immune reconstitution occurs.
- 12.5-17% spontaneously lose HBeAg or seroconvert in the postpartum period - this is generally favorable.
- Rarely, fulminant hepatitis can occur - monitor LFTs for at least 6 months after delivery.
- If antiviral therapy is stopped postpartum, monitor closely for flares; restart therapy if ALT rises significantly.
6. Neonatal Management (CRITICAL)
Figure: Birth-dose algorithm based on maternal HBsAg status and birth weight
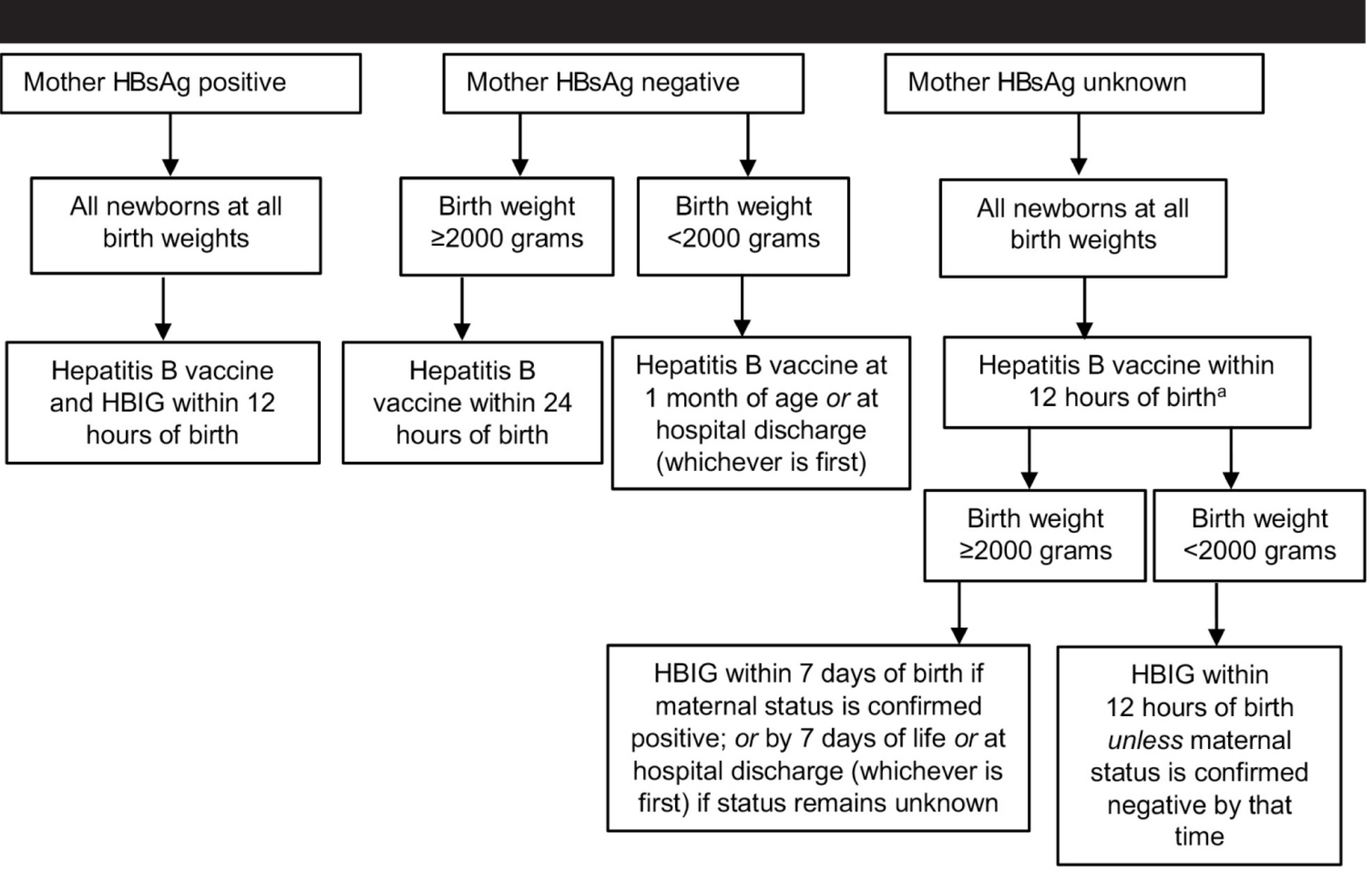
For infants of HBsAg-positive mothers:
| Action | Detail |
|---|---|
| HBV vaccine + HBIG (0.5 mL IM) | Within 12 hours of birth, at separate anatomic sites - applies to ALL birth weights |
| Complete 3-dose vaccine series | Months 1-2, and 6 after birth dose |
| If birth weight <2000 g | Give vaccine + HBIG within 12 hours; initial dose does NOT count - total 4 doses required |
| Post-vaccination serology | Test HBsAg and anti-HBs at 9-18 months (after vaccine series completion) |
- Passive-active immunoprophylaxis is 85-95% effective in preventing MTCT when given promptly.
- HBIG effectiveness diminishes rapidly; interval of effectiveness is unlikely to exceed 7 days.
- Infants who remain HBsAg-positive at testing have likely been infected in utero (accounts for <2% of cases).
- Red Book 2021, p. 636-638 | Yamada's Textbook of Gastroenterology, p. 835
7. Summary Checklist
| Timing | Action |
|---|---|
| First trimester | Screen all women with HBsAg; if positive, add HBeAg, HBV DNA, LFTs |
| Throughout pregnancy | Monitor LFTs; assess fibrosis if needed |
| Late 2nd / early 3rd trimester | Start TDF if HBV DNA >200,000 IU/mL (to reduce MTCT) |
| Delivery | Vaginal delivery acceptable; ensure neonatal team aware |
| Within 12 hours of birth | Give neonate HBV vaccine + HBIG at separate sites |
| Postpartum | Monitor mother's LFTs for 6 months; complete infant vaccine series |
| 9-18 months | Post-vaccination serology on infant |
Recent evidence: The ACOG Clinical Practice Guideline No. 6 (2023) and the AGA Clinical Practice Update (2024) both support TDF use in high-viral-load mothers and universal neonatal immunoprophylaxis. The question of whether TDF provides benefit above optimal immunoprophylaxis (given within 1 hour of birth) remains under active study.
This is a shared conversation. Sign in to Orris to start your own chat.