Osteology of scapula w.r.t. MS 1 level, easy explanation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have excellent diagrams and comprehensive content. Let me compile the full, well-structured MS1-level answer.
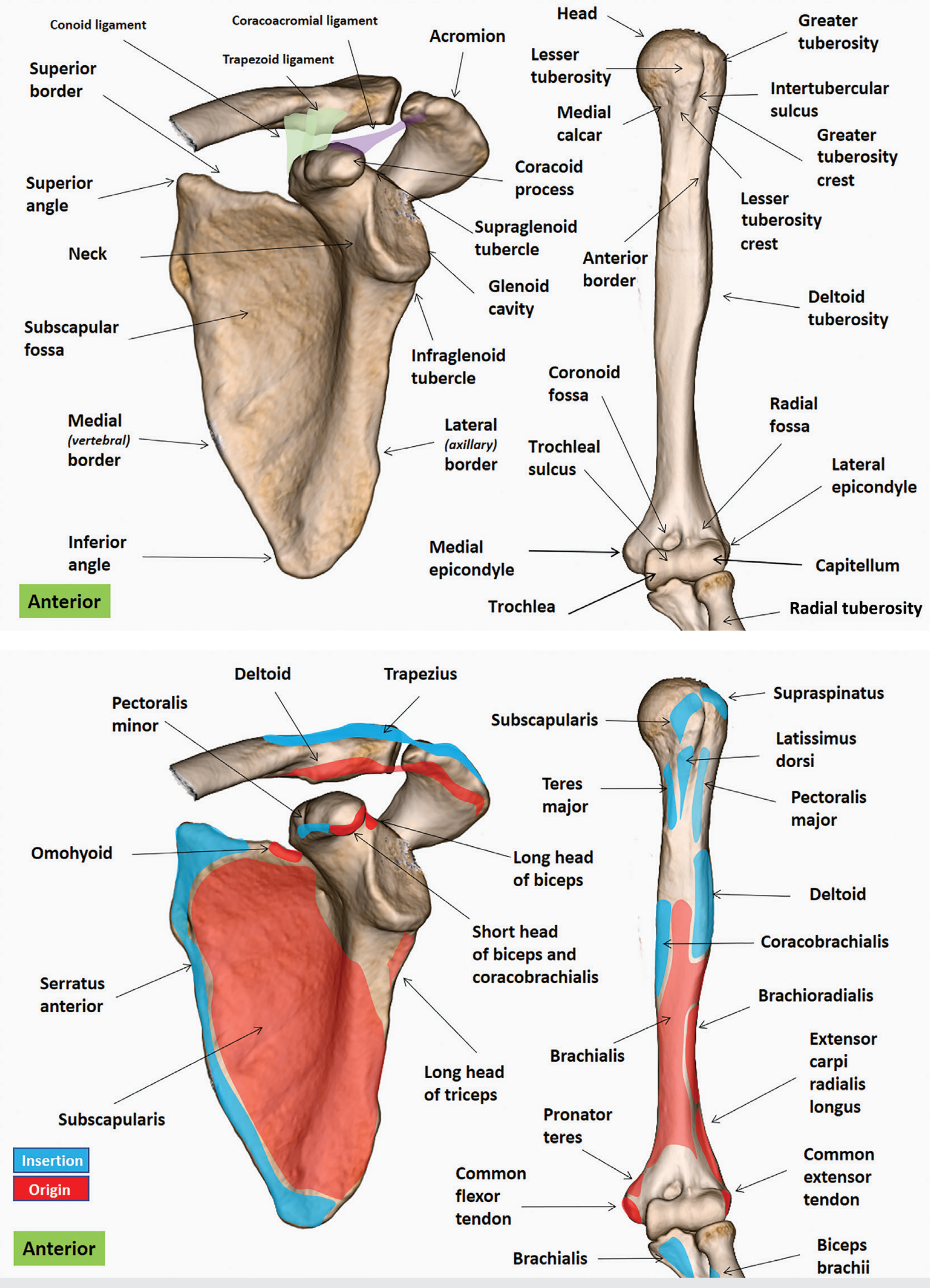
Osteology of the Scapula - MS1 Level
The scapula ("shoulder blade") is a large, flat, triangular bone on the posterolateral aspect of the thoracic wall, lying over ribs 2-7. It connects the upper limb to the axial skeleton by articulating with the clavicle (at the acromioclavicular joint) and with the humerus (at the glenohumeral joint).
Anterior (Costal) View
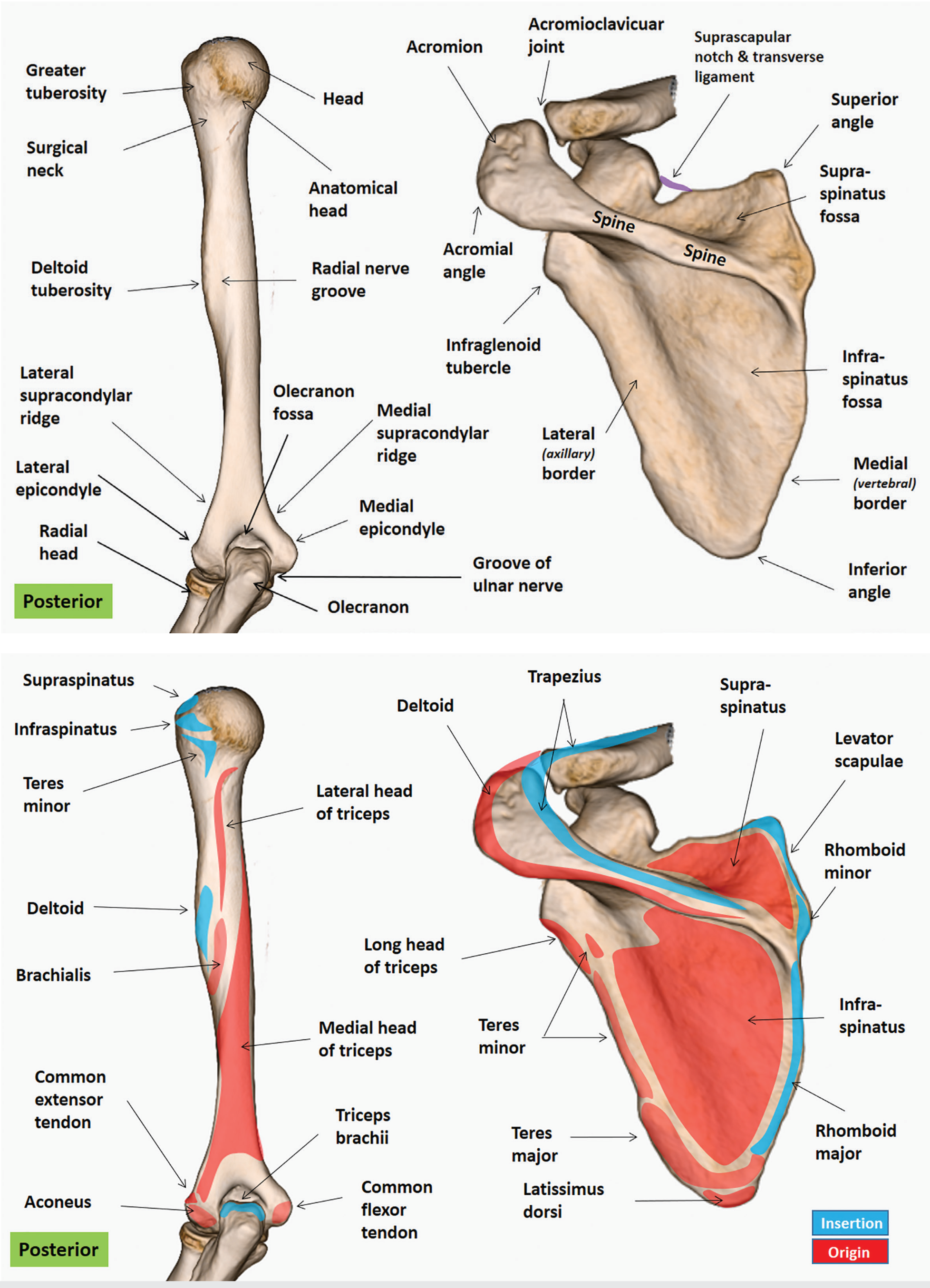
Posterior View
The "3-3-2-3" Framework (Easy Memory Tool)
The scapula has:
- 3 Angles
- 3 Borders
- 2 Surfaces
- 3 Processes
1. Three Angles
| Angle | Location | Key Feature |
|---|---|---|
| Superior angle | Upper medial corner | Covered by trapezius |
| Inferior angle | Bottom tip | Palpable landmark; covered by latissimus dorsi |
| Lateral angle | Outer corner | Bears the glenoid cavity (shoulder joint socket) |
The lateral angle is the most important - it is expanded into the neck of the scapula and ends in the glenoid cavity.
2. Three Borders
| Border | Also Called | Key Attachment |
|---|---|---|
| Superior border | Shortest | Contains the suprascapular notch (covered by transverse scapular ligament; suprascapular nerve passes through the notch, artery passes over it) |
| Medial border | Vertebral border | Rhomboid major + minor, levator scapulae, serratus anterior (serrated attachments) |
| Lateral border | Axillary border | Infraglenoid tubercle at top (long head of triceps origin); teres major + teres minor attachments |
3. Two Surfaces
Costal (Anterior) Surface
- Mostly hollow = subscapular fossa
- Filled by the subscapularis muscle (a rotator cuff muscle)
- The serratus anterior attaches along the medial edge
Posterior (Dorsal) Surface
- Divided by the spine of the scapula into two fossae:
- Supraspinous fossa (above spine) - smaller; origin of supraspinatus
- Infraspinous fossa (below spine) - larger; origin of infraspinatus medially, teres minor superolaterally, teres major inferolaterally
- The two fossae communicate at the spinoglenoid notch (important - suprascapular nerve passes through here to reach infraspinatus)
4. Three Processes
A. Spine of the Scapula
- A triangular bony ridge on the posterior surface
- Divides the posterior surface into supra- and infraspinous fossae
- Trapezius inserts on its superior surface; deltoid originates from its inferior surface
- Continues laterally as the acromion
B. Acromion
- The "roof" of the shoulder joint
- Projects laterally/anteriorly over the glenohumeral joint
- Articulates with the clavicle at the acromioclavicular (AC) joint
- Middle deltoid originates here
- Clinically: os acromiale = failure of fusion of ossification centers (seen in 7-15% of people); can cause impingement syndrome
C. Coracoid Process ("Crow's Beak")
- Hook-shaped projection from the superior border of the scapular neck
- Projects anteriorly and laterally
- Origin: Short head of biceps brachii + coracobrachialis (from tip); pectoralis minor (from medial surface)
- Ligaments: coracoacromial ligament (to acromion), coracoclavicular ligaments = conoid + trapezoid (to clavicle)
- Important landmark - brachial plexus and axillary vessels lie medial and inferior to it
5. The Glenoid Cavity
- Shallow, comma-shaped socket at the lateral angle
- Only 1/3 to 1/4 the size of the humeral head (hence the shoulder's wide range of motion - but also instability)
- Supraglenoid tubercle - above the cavity; origin of long head of biceps brachii (intracapsular tendon)
- Infraglenoid tubercle - below the cavity; origin of long head of triceps brachii (extracapsular)
6. Quick Muscle Attachment Summary
| Region | Muscle Origin (O) / Insertion (I) |
|---|---|
| Subscapular fossa | Subscapularis (O) |
| Supraspinous fossa | Supraspinatus (O) |
| Infraspinous fossa | Infraspinatus (O) |
| Lateral border | Teres minor (O), Teres major (O) |
| Medial border | Serratus anterior (I), Rhomboids (I), Levator scapulae (I) |
| Coracoid tip | Short head biceps + Coracobrachialis (O) |
| Supraglenoid tubercle | Long head biceps (O) |
| Infraglenoid tubercle | Long head triceps (O) |
| Spine/Acromion | Trapezius (I), Deltoid (O) |
| Costal medial edge | Serratus anterior (I) |
7. Clinical Points (MS1 High-Yield)
- Suprascapular notch - suprascapular nerve entrapment here causes supraspinatus + infraspinatus weakness (external rotation + abduction weakness)
- Spinoglenoid notch - a second site of suprascapular nerve compression; only affects infraspinatus (external rotation weakness alone)
- Winged scapula - loss of serratus anterior function (long thoracic nerve injury); medial border of scapula protrudes posteriorly when pushing against a wall
- AC joint injury - acromion forced downward relative to clavicle when falling on an outstretched arm
Sources: Gray's Anatomy for Students; Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3
Gross anatomy of breast and axillary lymph nodes. MS1 level,. easy explanation with mnemonics etc
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I have everything I need for a thorough, well-illustrated MS1-level answer. Let me now compile it.
Gross Anatomy of the Breast & Axillary Lymph Nodes - MS1 Level
PART 1: GROSS ANATOMY OF THE BREAST
Position & Extent
The breast lies between the skin and the superficial pectoral fascia, overlying the pectoralis major muscle. Its base spans:
- Vertically: Rib 2 to Rib 6
- Horizontally: Sternum to mid-axillary line
- It also overlies the serratus anterior and external oblique muscles laterally
Mnemonic for borders: "2 to 6, Sternum to Side"
The Axillary Tail (of Spence)
A tongue of breast tissue wraps around the lower margin of pectoralis major and enters the axilla. This is the axillary tail (process) of Spence. It is clinically important - cancer can arise here and be mistaken for an axillary mass.
Breast Cross-Section - Complete Diagram
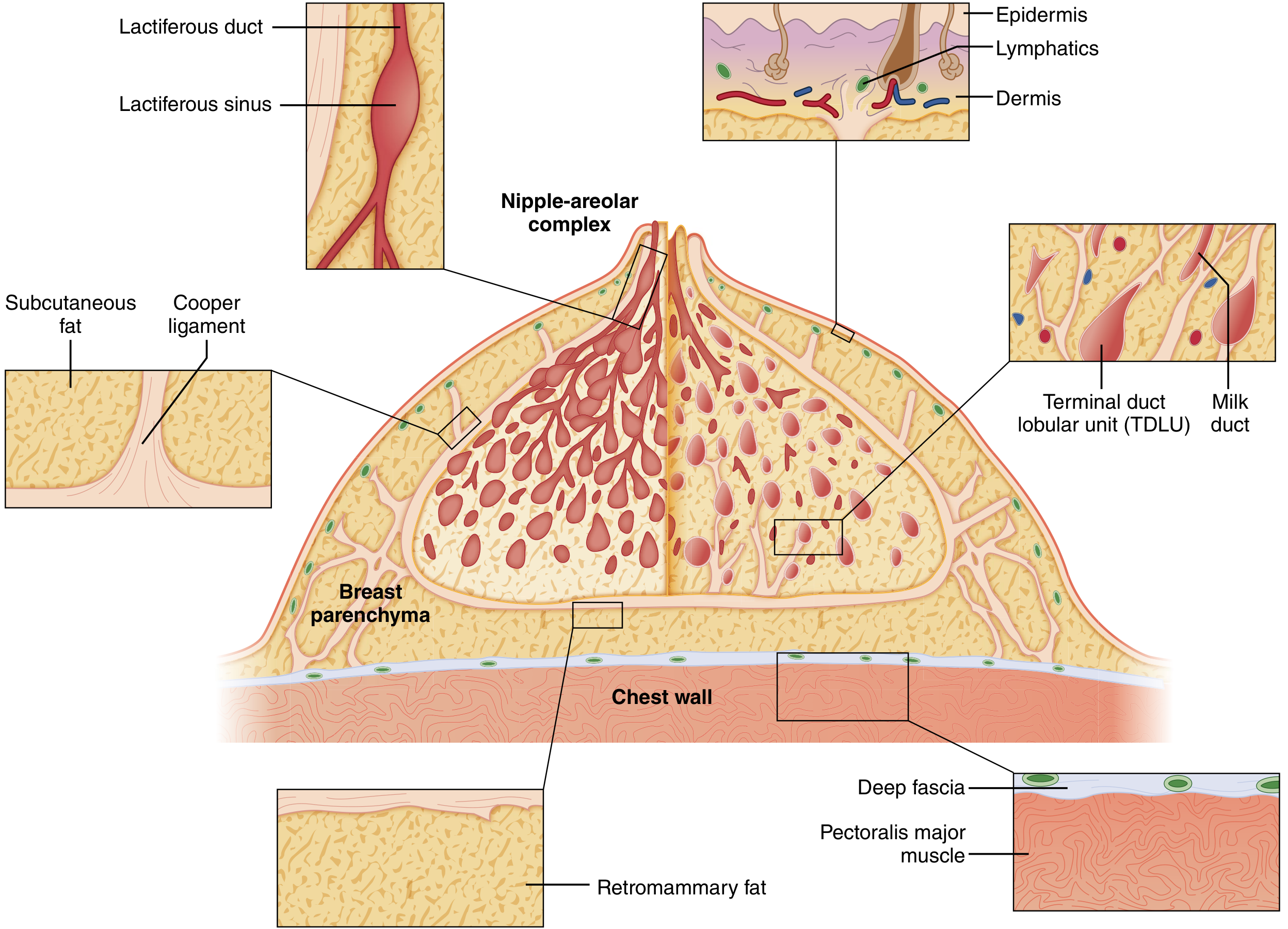
Structural Layers (Surface to Deep)
Think: "Skin - Fat - Gland - Fat - Fascia - Muscle"
| Layer | Contents |
|---|---|
| Skin | Nipple-areolar complex (NAC) |
| Subcutaneous fat | Surrounds glandular tissue |
| Glandular parenchyma | Lobes, ducts, TDLU |
| Retromammary fat | Behind the breast, before fascia |
| Superficial pectoral fascia | Deep boundary of breast |
| Pectoralis major muscle | The "floor" |
Three Tissue Components
Mnemonic: "GFA" - Gland, Fat, Architecture
- Glandular epithelium - the secretory machinery
- Adipose tissue - dominant in postmenopausal women
- Fibrous stroma - connective tissue scaffold
The Duct System (like an inverted tree)
Nipple (15-20 openings)
↑
Lactiferous sinuses (ampullae - dilated just below NAC)
↑
Lactiferous ducts (major ducts, 15-20 total)
↑
Segmental ducts → Subsegmental ducts
↑
Terminal ductules → Acini
= TDLU (Terminal Duct Lobular Unit)
Key fact: There are 15-20 lobes, each with its own lactiferous duct opening at the nipple. The TDLU is where most breast cancers originate.
Cooper's Ligaments (Suspensory Ligaments)
- Fibrous bands running from the chest wall (deep fascia) to the dermis
- Give the breast its shape and support
- When infiltrated by cancer, they shorten and pucker the skin
- This causes skin dimpling and the classic "peau d'orange" (orange peel) appearance
Memory hook: Cooper's ligaments = the "tent pegs" of the breast. When cancer pulls on them, the tent surface dimples.
Blood Supply
Mnemonic: "ILI" - Internal thoracic, Lateral thoracic, Intercostals
| Source | Branch | Region supplied |
|---|---|---|
| Internal thoracic artery | Medial mammary perforators (2nd-4th intercostal spaces) | Medial breast (major supply) |
| Lateral thoracic artery | Lateral mammary branches | Lateral breast |
| Intercostal arteries (2nd-5th) | Mammary branches | Various quadrants |
The internal thoracic artery (via perforators) is the dominant supply - this is why medial breast tumors can spread to internal mammary nodes.
Nerve Supply
Sensory innervation from intercostal nerves T2-T6 (lateral + medial mammary branches) and supraclavicular nerves (cervical plexus) to the upper breast.
High yield: The T4 intercostal nerve provides sensation to the nipple. Injury during breast surgery can cause nipple anesthesia.
PART 2: AXILLARY LYMPH NODES
Lymphatic Drainage of the Breast - Overview
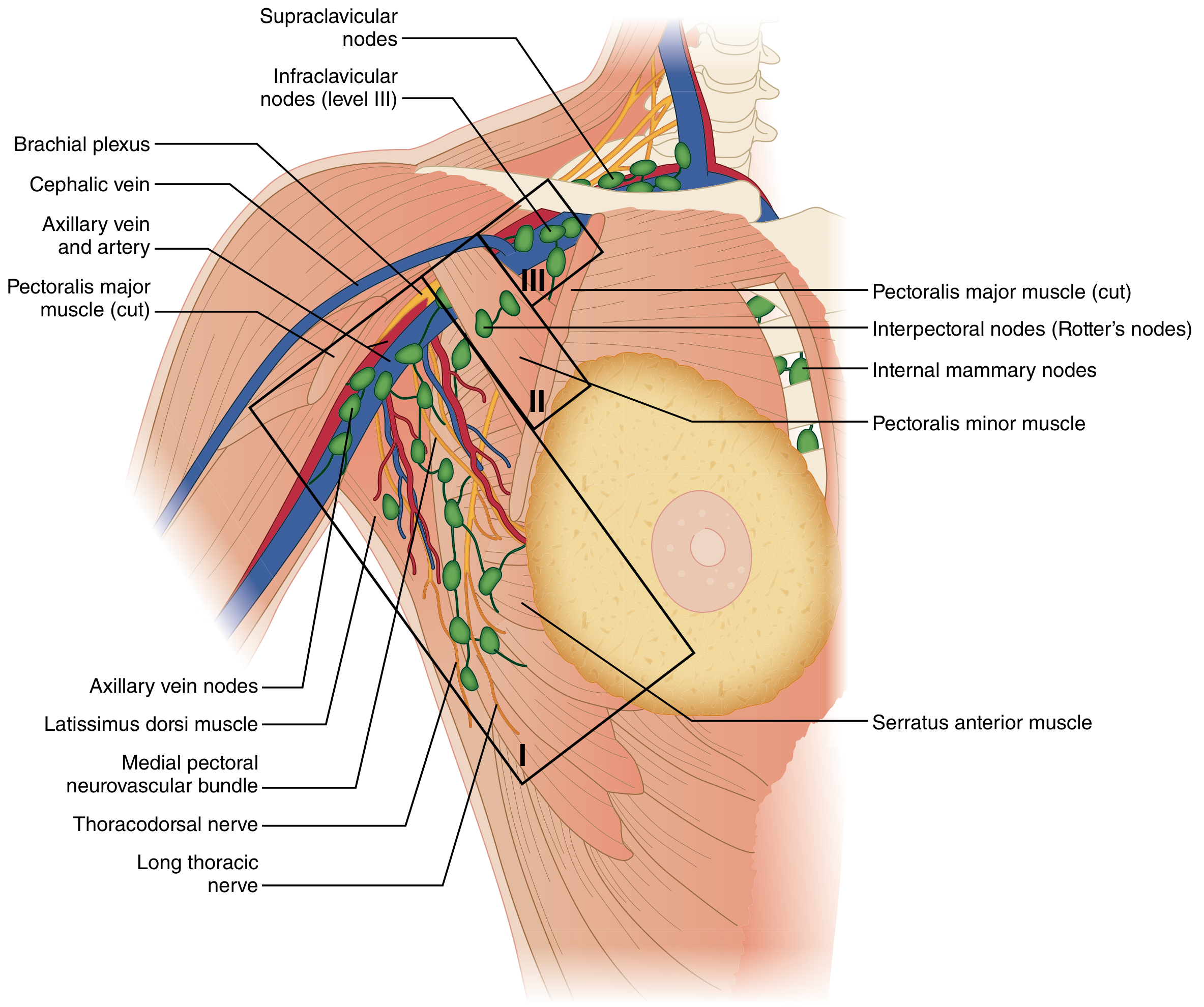
~75-97% of breast lymph drains to axillary nodes. The rest goes to internal mammary (parasternal) nodes.
The Three Levels of Axillary Nodes
The landmark for all three levels is the pectoralis minor muscle:
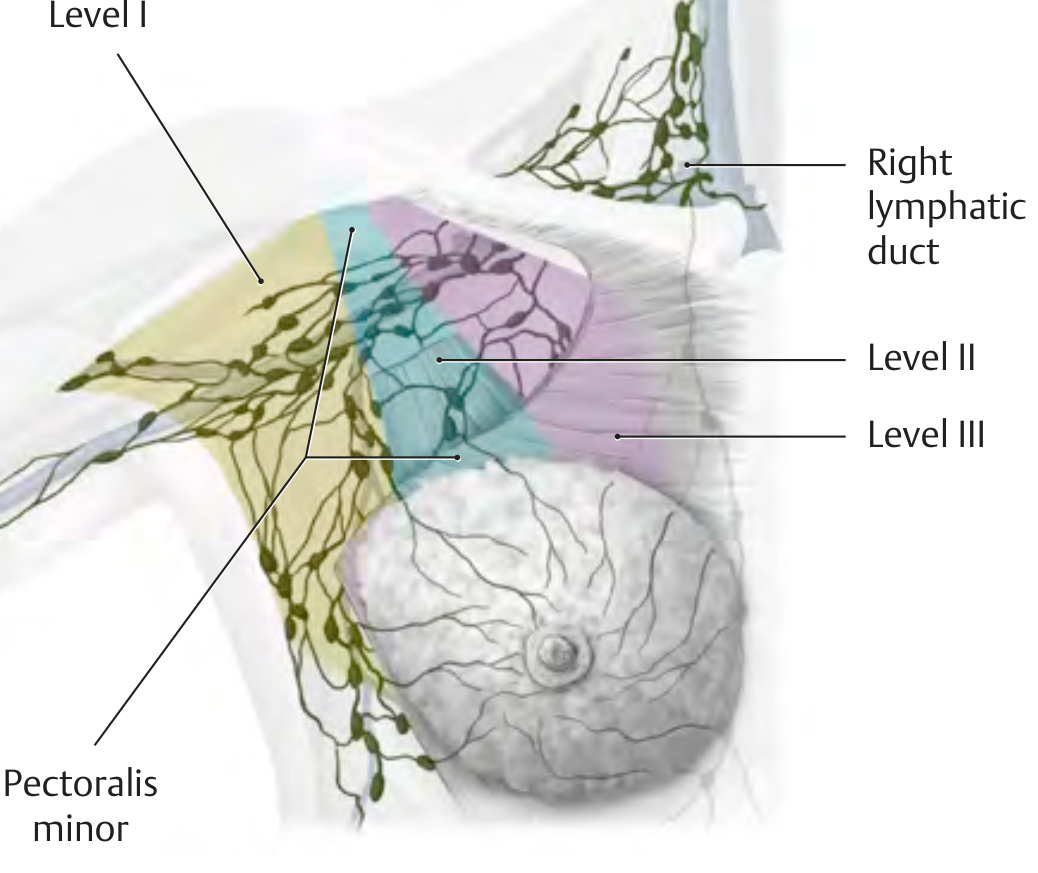
Mnemonic: "LAM" - Lateral, Along, Medial (relative to pectoralis minor)
| Level | Position relative to pec minor | Nodes included | Drainage |
|---|---|---|---|
| Level I (lower) | Lateral to pec minor | Pectoral (anterior), Subscapular (posterior), Humeral (lateral), Paramammary | First station - primary drainage |
| Level II (middle) | Along pec minor | Central axillary, Interpectoral (Rotter's nodes) | Second station |
| Level III (upper) | Medial to pec minor (infraclavicular) | Apical axillary nodes | Final axillary station |
Complete Axillary Node Map (with all named groups)
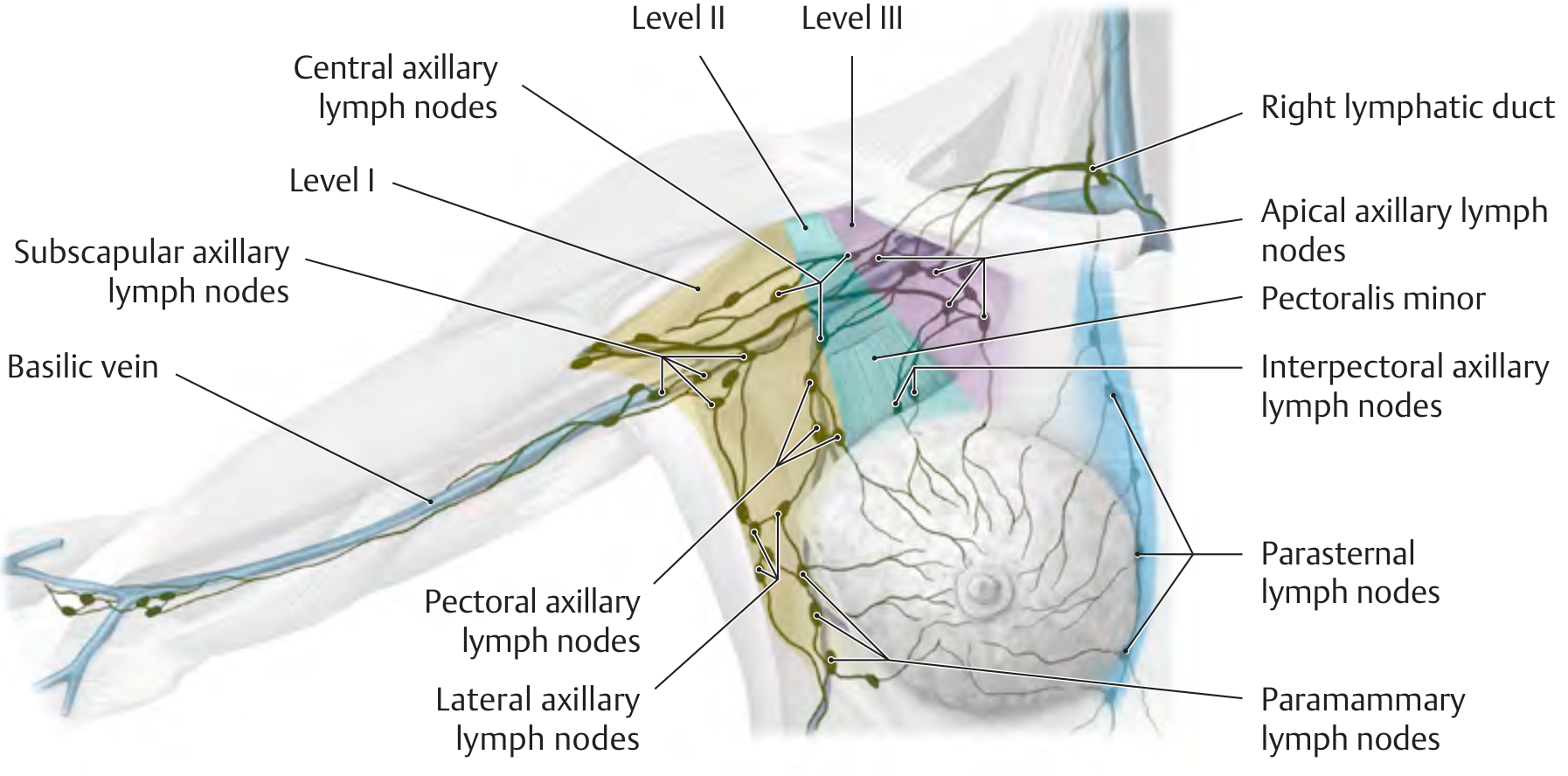
Named Groups - Easy Memory System
"PSHCIA" for Level I (Pectoral, Subscapular, Humeral, Central gets divided here too, Interpectoral, Apical):
More simply:
| Group | Location | Drains |
|---|---|---|
| Pectoral (anterior) | Along medial wall of axilla / lateral chest | Anterior breast |
| Subscapular (posterior) | Along posterior axillary wall | Back, posterior shoulder |
| Humeral (lateral) | Along medial side of humerus / axillary vein | Upper limb |
| Central | Fat of axilla, behind pec minor | All Level I groups drain here |
| Interpectoral (Rotter's) | Between pec major and minor | Deep breast, goes straight to Level II |
| Apical | Above/medial to pec minor | All axillary nodes drain here |
Drainage Pathway
Breast → Level I → Level II → Level III (Apical)
↓
Subclavian lymphatic trunk
↓
Right lymphatic duct (right side)
Thoracic duct (left side)
↓
Junction of subclavian + internal jugular veins
Rotter's Nodes (Interpectoral nodes) - Exam Favorite
- Located between pectoralis major and pectoralis minor
- Part of Level II
- Can be bypassed by cancer skipping Level I entirely ("skip metastases")
- Surgically important: must be removed in modified radical mastectomy
Other Lymphatic Drainage Routes (Minor Pathways)
| Route | Destination | When important |
|---|---|---|
| Internal mammary (parasternal) nodes | Along internal thoracic vessels | Medial breast quadrant tumors |
| Supraclavicular nodes | Above clavicle | Advanced disease (N3 in staging) |
| Cross-drainage | Contralateral breast | Rare, explains contralateral spread |
| Subdiaphragmatic | Abdominal nodes | Inferior breast, very rare |
Important Nerves at Risk During Axillary Surgery
| Nerve | Muscle innervated | Injury consequence |
|---|---|---|
| Long thoracic nerve (C5,6,7) | Serratus anterior | Winged scapula |
| Thoracodorsal nerve | Latissimus dorsi | Weak arm adduction/extension |
| Medial pectoral nerve | Pectoralis major (and minor) | Pectoral wasting |
| Intercostobrachial nerve | Sensory - medial upper arm | Numbness/pain of inner upper arm |
Mnemonic: Nerves to protect = "Long Thoraco-Medial Intercostal" = LTMI - "Let The Muscle live, Intercostal too"
Clinical High-Yield Summary
| Concept | Key point |
|---|---|
| Sentinel node | First node(s) in lymphatic chain; usually in pectoral/external mammary group (Level I) |
| Skip metastases | Tumor bypasses Level I, goes directly to Level II or III; seen in ~5% |
| Peau d'orange | Cooper's ligament infiltration + dermal lymphatic obstruction |
| Axillary tail of Spence | Breast tissue in axilla; can be mistaken for axillary lymphadenopathy |
| Levels = surgical staging | Level I dissection standard; Level III = radical mastectomy territory |
Sources: Sabiston Textbook of Surgery; Gray's Anatomy for Students; General Anatomy and Musculoskeletal System (Thieme Atlas); Imaging Anatomy, Vol. 3
This is a shared conversation. Sign in to Orris to start your own chat.