Yo
Hey! How can I help you today?
A patient complaint of sleepless night
Reading File
Finding Sources
Searching PubMed
"insomnia" AND "treatment"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive clinical overview of Insomnia for your patient:
Insomnia - Clinical Overview
Definition
Insomnia is the complaint of difficulty initiating or maintaining sleep, or of unrefreshing sleep, resulting in daytime symptoms such as fatigue, irritability, impaired cognition, and reduced performance. The key distinction from simply needing less sleep is the presence of daytime sequelae.
- Acute/Short-term insomnia: <3 months; affects >30% of adults
- Chronic insomnia: >3 months; affects ~10% of adults
(Harrison's Principles of Internal Medicine 22E, Goldman-Cecil Medicine)
Epidemiology & Risk Factors
- More common in women, older adults, lower socioeconomic status
- Strong association with psychiatric and chronic medical illness
- Personality traits: obsessive-compulsive tendency, frequent rumination, poor coping
Differential Diagnosis
The following chart from Goldman-Cecil shows the major categories:
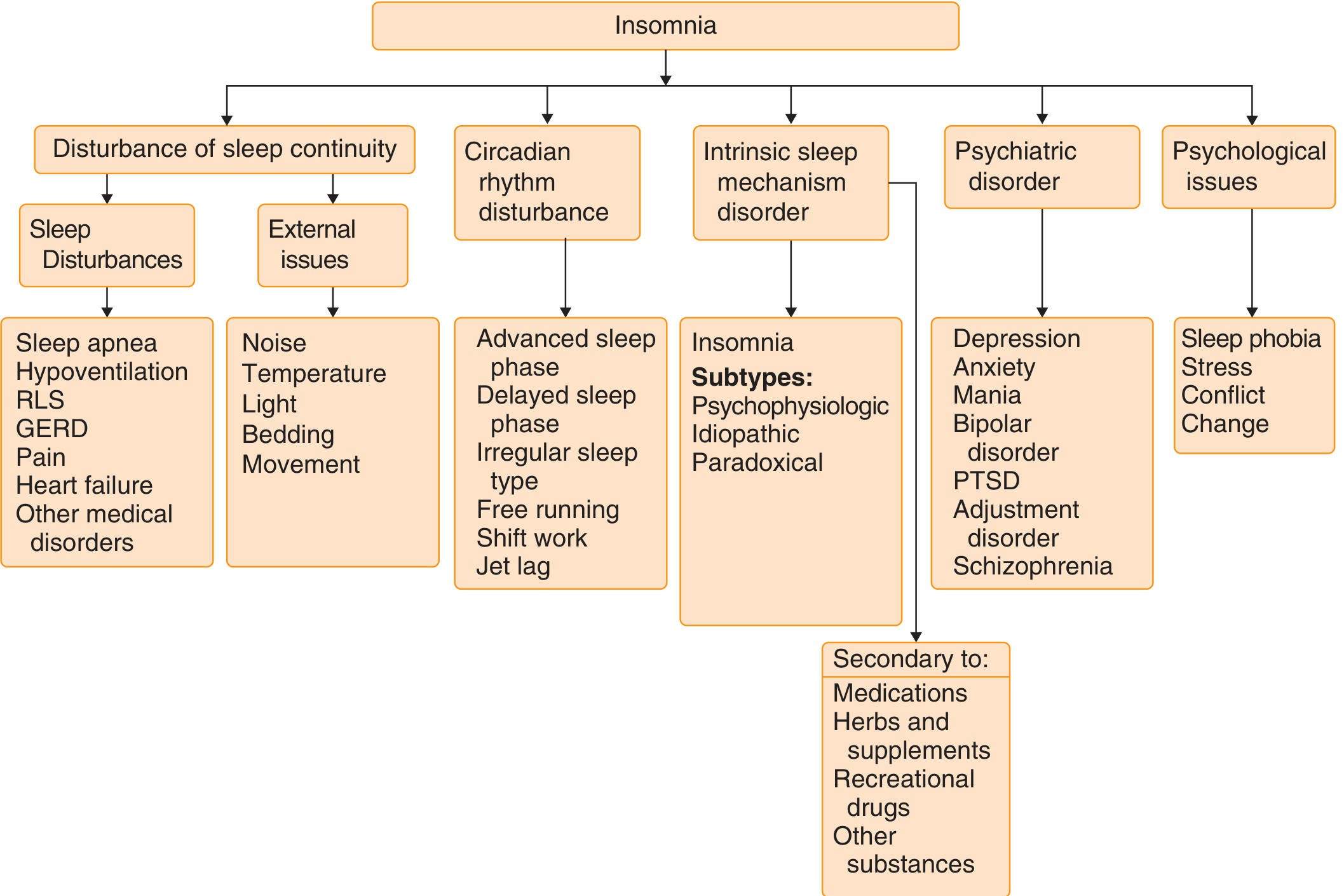
Classification of Adult Insomnia
| Category | Subtype | Description |
|---|---|---|
| Primary | Psychophysiologic | Conditioned arousal - associating bed with wakefulness; sleep better in new environment |
| Idiopathic | Starts in childhood, lifelong; impaired intrinsic sleep mechanisms | |
| Paradoxical | Marked mismatch between subjective complaint and objective polysomnogram | |
| Secondary | Adjustment insomnia | Acute psychosocial stressor |
| Inadequate sleep hygiene | Lifestyle habits impairing sleep | |
| Comorbid psychiatric | Anxiety, depression, mania, PTSD, schizophrenia | |
| Comorbid medical | Renal/hepatic failure, pain, GERD, heart failure, hot flashes | |
| Drug/substance-induced | Medications, alcohol, caffeine, recreational drugs |
History - The 3 "P" Framework
- Predisposing factors - lighter-than-normal sleep baseline, anxious personality
- Precipitating factors - illness, loss, job change, new medication
- Perpetuating factors - maladaptive behaviors that maintain the insomnia
Key questions to ask:
- Timing: difficulty falling asleep (delayed sleep phase, phobia) vs. early morning awakening (depression, advanced sleep phase)
- Caffeine, alcohol, tobacco intake and timing
- Medications review
- Bed partner report (snoring, limb movements suggesting sleep apnea or RLS)
- 24-hour schedule and nap habits
(Harrison's 22E, Goldman-Cecil Medicine)
Common Contributing Factors
Psychiatric (~80% of psychiatric patients have sleep complaints)
- Depression - classic early morning awakening, but also onset/maintenance problems
- Anxiety - racing thoughts, rumination
- Mania/hypomania - substantially reduced sleep
- PTSD, schizophrenia
Medical
- Pain (rheumatologic disorders, neuropathy)
- Respiratory: asthma, COPD, heart failure, OSA
- GERD, menopause (hot flashes)
- Neurologic: dementia, Parkinson's disease
- ~60% of long-COVID patients report insomnia
Medications / Substances
- Caffeine (half-life 6-9 h - can disrupt sleep up to 8-14 h after ingestion)
- Alcohol (disrupts sleep architecture)
- Many psychoactive, cardiovascular, and respiratory drugs
Poor Sleep Hygiene
- Daytime napping
- Irregular sleep-wake schedule
- Screen use in bed (blue light suppresses melatonin)
- Using the bedroom for work, TV, arguing
Treatment
Step 1 - Treat the Underlying Cause
Address any medical or psychiatric condition (pain, depression, GERD, etc.)
Step 2 - Sleep Hygiene (ALL patients)
| Do | Avoid |
|---|---|
| Use bed only for sleep and sex | Napping, especially after 3 PM |
| Fixed bedtime and wake time every day | Caffeine after lunchtime |
| 20-30 min wind-down routine (bath, meditation, reading) | Alcohol and smoking near bedtime |
| Dark, quiet, comfortable bedroom | Screens and smartphones in bed |
| If awake >20 min, get out of bed | Heavy meals or vigorous exercise within 2-3 h of bed |
Step 3 - Cognitive Behavioral Therapy for Insomnia (CBT-I) - First-line
- Cognitive restructuring - reframe faulty beliefs and worries about sleep
- Stimulus control therapy - break conditioned bed-wakefulness association
- Sleep restriction therapy - limit time in bed to consolidate sleep
- Relaxation techniques - progressive muscle relaxation, meditation
- Can be delivered online/digitally with similar efficacy
CBT-I is the standard first-line treatment and provides long-term success.
Step 4 - Pharmacotherapy (adjunct to CBT-I, short-term preferred)
| Drug Class | Agents | Notes |
|---|---|---|
| BzRA (Z-drugs) | Zaleplon 5-20 mg (t½ 1-2h), Zolpidem 5-10 mg (t½ 2-4h), Eszopiclone 1-3 mg (t½ 5-8h), Temazepam 15-30 mg (t½ 8-20h) | Match half-life to problem (onset vs. maintenance). Use intermittently. |
| Benzodiazepines | Lorazepam, Triazolam, Clonazepam | First-line per Goldman-Cecil; risk of dependence with long-term use |
| Orexin antagonists | Suvorexant 10-20 mg, Daridorexant 25-50 mg, Lemborexant | Block hypocretin to promote sleep maintenance; newer agents |
| Melatonin receptor agonist | Ramelteon 8 mg | Good for sleep-onset issues; minimal dependence risk |
| Antidepressants | Trazodone, Doxepin | Useful when comorbid depression/anxiety present |
| Antihistamines | Diphenhydramine | OTC; tolerance develops quickly; avoid in elderly (anticholinergic effects) |
Note: For comorbid depression/anxiety, combining a short-term hypnotic with a long-term antidepressant/anxiolytic is better than either alone.
Recent evidence (2025): A network meta-analysis found daridorexant, lemborexant, and suvorexant (orexin antagonists) are effective and safe for insomnia - daridorexant showing favorable tolerability. Melatonin timing and dosing optimization is also well-supported by recent meta-analysis.
Prognosis
- Most patients improve; some relapse
- CBT-I is key to long-term success
- Chronic insomnia may herald an affective disorder and is associated with higher dementia risk in older adults
- Sleep diary for 2 weeks is a useful tool in management
- Polysomnography only if sleep apnea is suspected or multiple therapies have failed
(Goldman-Cecil Medicine, Harrison's 22E)
This is a shared conversation. Sign in to Orris to start your own chat.