How to diagnose different types of radiculopathies of the cervical and lumbosacral region from history, physical examination, and motor, sensory testing. How to remember which nerve root supplies which dermatome, myotome, and reflexes, and muscles ? Also give images and illustrations to remember them easily .. Give me mnemonics wherever possible and make this topic easy for me to remember for my first FCPS Part 2 exam, MRCP and USMLE steps exam.
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
cervical lumbosacral radiculopathy dermatome myotome reflex mnemonic USMLE MRCP
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Searching the Web
lumbar radiculopathy L3 L4 L5 S1 dermatome myotome reflex table diagram illustration
Reading File
Loading Image
Loading Image
Finding Sources
Now I have all the information needed. Let me compile this comprehensive guide:
Radiculopathies: Cervical & Lumbosacral - Complete Exam Guide
The Big Picture First
Radiculopathy = nerve root compression giving a triad:
- Pain radiating in a dermatomal pattern
- Sensory loss/paresthesias in the dermatome
- Motor weakness in the myotome + reflex loss
The key exam question is always: "Which level?" - answered by matching the pattern of weakness + sensory loss + reflex change.
PART 1: CERVICAL RADICULOPATHY
Anatomy Concept to Know First
The cervical nerve root exits above its numbered vertebra (C5 root exits between C4-C5). This means:
- C4-C5 disc herniation → compresses C5 root
- C5-C6 disc herniation → compresses C6 root
- C6-C7 disc herniation → compresses C7 root
- C7-T1 disc herniation → compresses C8 root
Mnemonic: "Cervical roots exit ABOVE = disc number = root below it"
C5, C6, C7 are the most commonly affected roots (levels of greatest cervical mobility and disc degeneration) - as confirmed in Bradley and Daroff's Neurology in Clinical Practice.
Cervical Radiculopathy at a Glance
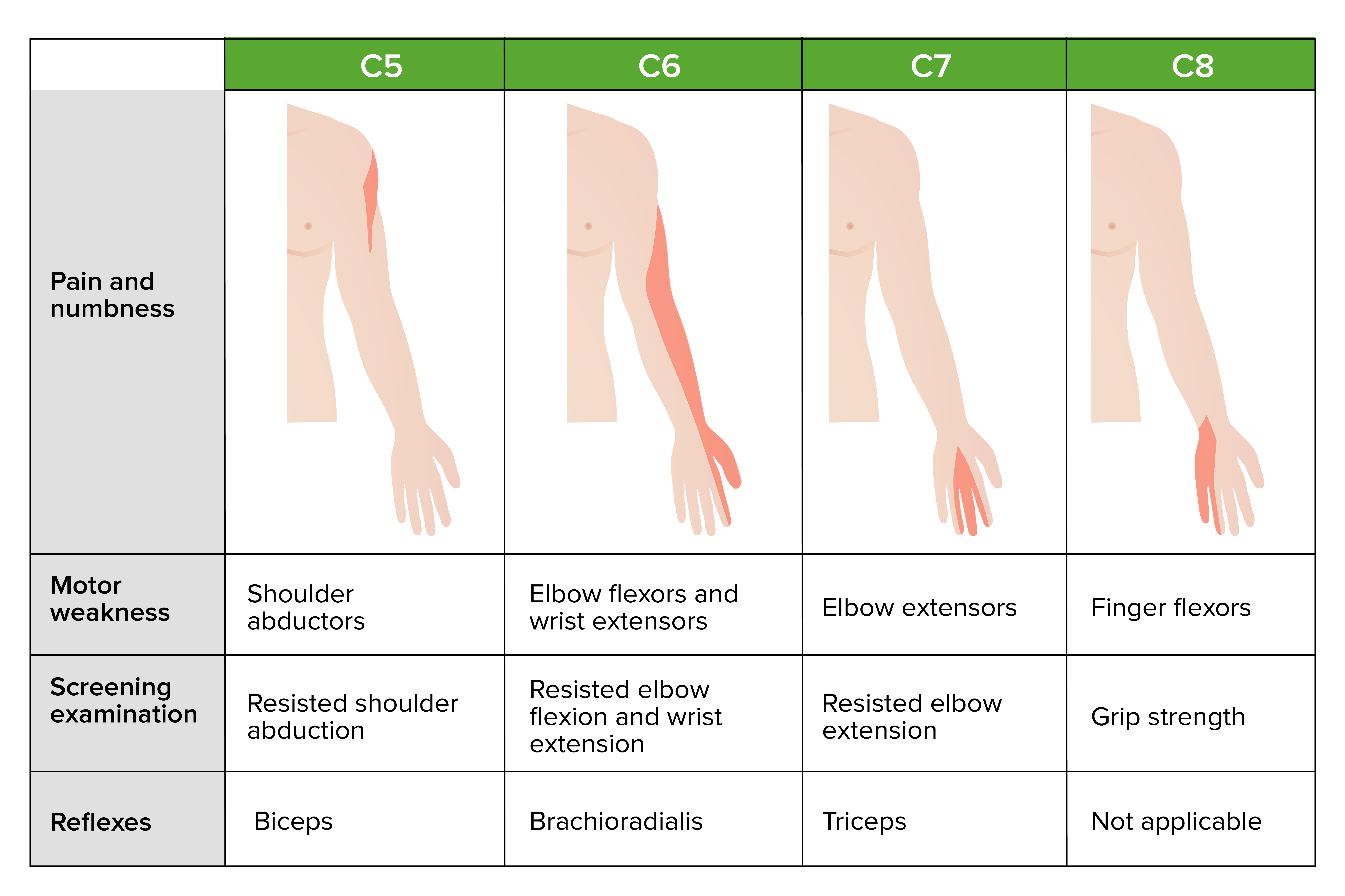
The "5-6-7-8 Ladder" - Master Mnemonic for Cervical Roots
| Root | Pain/Sensory area | Key Muscle | Test movement | Reflex | Mnemonic |
|---|---|---|---|---|---|
| C5 | Shoulder/lateral arm | Deltoid, Biceps | Shoulder abduction | Biceps | "C5 = Shoulder shrug/abDuct" |
| C6 | Lateral forearm, thumb + index | Biceps, Brachioradialis, Wrist extensors | Elbow flexion + wrist extension | Brachioradialis | "C6 = siX-pack thumb (thumb is digit 1=index)" |
| C7 | Middle finger, posterior arm | Triceps, Wrist flexors, Pronators | Elbow extension | Triceps | "C7 = sEVEn = EXTEND (triceps)" |
| C8 | Ring + little finger, medial forearm | Finger flexors, Intrinsics | Grip strength / finger flexion | None | "C8 = grEIGHt (grip)" |
| T1 | Medial upper arm | Intrinsics (interossei) | Finger abduction/adduction | None | "T1 = Tiny interossei" |
Master Mnemonic: "BiBoTri-No" = C5 Biceps / C6 Brachioradialis / C7 Triceps / C8 No reflex
Or remember: B-B-T going down = Biceps (C5-C6), Brachioradialis (C6), Triceps (C7).
C5 Radiculopathy (C4-C5 disc)
History: Pain from neck → shoulder → lateral arm. Weakness lifting arm overhead.
Dermatome: Lateral shoulder, lateral upper arm ("epaulette" area)
Myotome weak: Deltoid (shoulder abduction), Biceps, Supraspinatus
Reflex lost: Biceps jerk (C5-C6)
Tip: Patient cannot comb their hair or lift arm above shoulder. "Shoulder problem, but no neck trauma."
Test: Resisted shoulder abduction - patient holds arm at 90° while you push down.
C6 Radiculopathy (C5-C6 disc) - Most common cervical level
History: Pain down lateral forearm into thumb + index finger. "My thumb goes numb."
Dermatome: Lateral forearm, thumb, index finger, lateral half of palm
Myotome weak: Biceps (elbow flexion), Brachioradialis, Wrist extensors (ECRL, ECRB)
Reflex lost: Biceps jerk AND Brachioradialis jerk
Special sign: "Inverted" or "paradoxical" brachioradialis reflex (tap BR → finger flexors contract but no BR contraction = myelopathy at same level)
Test: Resisted elbow flexion + resisted wrist extension
C7 Radiculopathy (C6-C7 disc) - Most common overall
History: Pain to middle finger (± ring finger). Weakness pushing things away ("can't do push-ups"). Subscapular/interscapular pain is classic.
Dermatome: Middle finger, dorsal forearm, posterior arm
Myotome weak: Triceps, Wrist flexors (FCR, FCU), Pronator teres, Finger extensors
Reflex lost: Triceps jerk (ONLY reflex exclusively for C7)
Tip: Triceps jerk = C7 exclusively. Test by tapping triceps tendon with elbow at 90°.
Test: Resisted elbow extension
C8 Radiculopathy (C7-T1 disc)
History: Pain/numbness to ring + little finger, medial forearm. Clumsy hand.
Dermatome: Medial forearm, ring + little finger
Myotome weak: Finger flexors (FDP, FDS), Intrinsic hand muscles, Abductor pollicis brevis
Reflex: No dedicated reflex (a common exam trap!)
Tip: C8 looks like ulnar nerve but SNAPS are normal in radiculopathy (preganglionic lesion)
T1 Radiculopathy
History: Medial upper arm pain/numbness, intrinsic hand weakness (often Pancoast tumor should be excluded)
Dermatome: Medial upper arm, inner elbow
Myotome: Intrinsic hand muscles (interossei, lumbricals)
Exam: Finger abduction/adduction weakness, look for Horner syndrome (ptosis, miosis, anhidrosis) - suggests Pancoast tumor
Special Provocation Tests for Cervical Radiculopathy
| Test | Technique | What positive means | Sens/Spec |
|---|---|---|---|
| Spurling Test | Extend neck + side-bend toward painful side + axial compression downward | Reproduces radicular arm pain | Low sensitivity, HIGH specificity |
| Cervical Distraction Test | Patient supine, lift head with hands under chin/occiput | Relief of radicular pain | Moderate sens, high spec |
| Upper Limb Tension Test (ULTT) | Scapular depression + shoulder abduction/flexion + elbow/wrist/finger extension, neck laterally bent away | Reproduces arm/hand pain | HIGH sensitivity (~90%), low specificity |
| Shoulder Abduction Relief Sign | Patient raises hand/arm above head | Relieves pain | Specific for C4-5 or C5-6 |
| Valsalva/Cough | Increases intrathecal pressure | Worsens radicular pain | ----- |
From Textbook of Family Medicine: Spurling test = low sens, high spec. Upper limb tension test = sensitivity >90%, low specificity. Straight-leg raise (lumbar) = sensitivity 91%, specificity 26%.
Mnemonic for Spurling: "SPECific for radiculopathy" = Spurling = SPECificity
PART 2: LUMBOSACRAL RADICULOPATHY
Key Anatomy Concept
In the lumbar region, roots exit below their numbered vertebra (unlike cervical). However, the disc at L4-L5 typically compresses the traversing L5 root (not L4), because L4 exits at L4-L5 foramen:
- L3-L4 disc → compresses L4 root (exiting at L3-L4 foramina) or traversing L4
- L4-L5 disc herniation → usually compresses traversing L5 root
- L5-S1 disc herniation → usually compresses traversing S1 root
Most common: S1 (from L5-S1 disc) and L5 (from L4-L5 disc)
Lumbosacral Radiculopathy Table

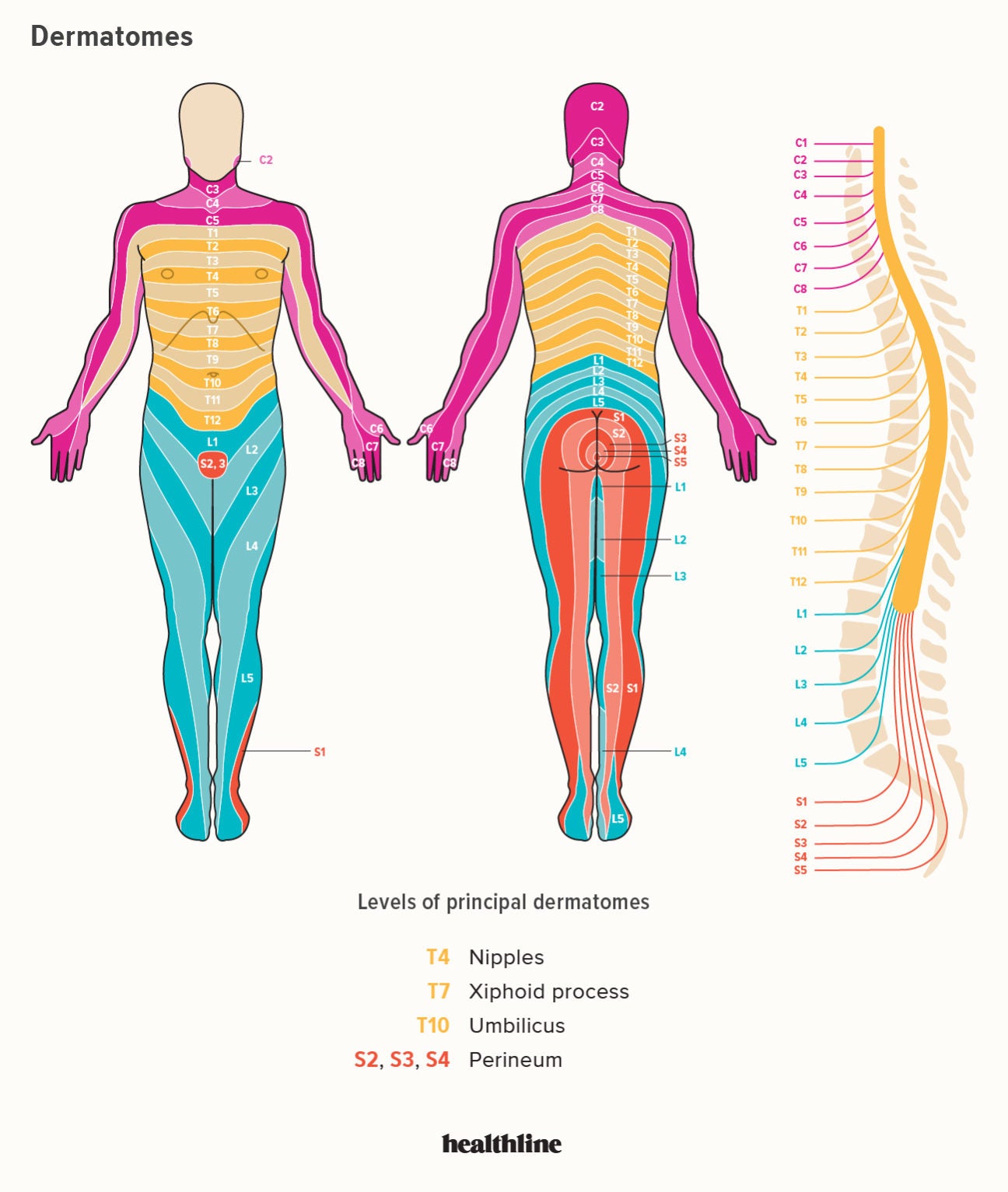
Body Dermatome Map
Lumbar Root Summary Table
| Root | Disc Level | Pain Pattern | Key Weakness | Reflex Lost | Sensory Area | Mnemonic |
|---|---|---|---|---|---|---|
| L2 | L1-L2 | Anterior thigh | Hip flexion | None | Anterior/medial upper thigh | "L2 = Loin to groin" |
| L3 | L2-L3 | Anterior thigh → medial knee | Knee extension, hip adduction | Patellar (partial) | Anterior thigh + medial knee | "L3 = Leg thREE, thigh/knee" |
| L4 | L3-L4 | Anterior thigh → medial shin | Knee extension (quads), foot inversion | Patellar/Knee jerk | Medial lower leg | "L4 = 4ward = kneecap" |
| L5 | L4-L5 | Buttock → lateral leg → dorsum foot → big toe | Foot/great toe dorsiflexion (EHL), hip abduction | Ankle jerk (sometimes, medial) | Lateral leg, dorsum foot, big toe | "L5 = L5ift foot up, big toe" |
| S1 | L5-S1 | Buttock → posterior thigh → lateral foot | Plantar flexion (calf), eversion | Ankle jerk / Achilles | Posterior thigh, calf, lateral foot/heel | "S1 = Soles of feet, Sole=S1, Ankle jerk" |
| S2-4 | - | Perineum, inner thighs | Bladder/bowel, sphincters | Bulbocavernosus/anal | Saddle area | "S2,3,4 keeps the poo off the floor" |
Lumbosacral Root Mnemonics
"2-3-4 in front, 5-1 behind"
- L2, L3, L4 radiculopathies → pain anteriorly (anterior thigh, medial leg) - tested by Femoral nerve stretch test
- L5, S1 → pain posteriorly (buttock, posterior leg) - tested by Straight Leg Raise (SLR)
Key Reflex Mnemonics
| Reflex | Root | Mnemonic |
|---|---|---|
| Biceps | C5-C6 | "B5-6 = Biceps 5 and 6" |
| Brachioradialis | C6 | "BR = Brachioradialis = Rad-6" |
| Triceps | C7 | "Tri7 = Triceps C7" |
| Patellar (knee jerk) | L3-L4 | "Patellar = L3-L4, knee goes fore" |
| Achilles (ankle jerk) | S1 | "Aching S1 ankle" or "S1 = Sole/Achilles" |
The "L4-L5-S1 Clinical Triad" (Exam Favourite)
| Feature | L4 | L5 | S1 |
|---|---|---|---|
| Weakness | Knee extension, foot inversion | Dorsiflexion of foot/big toe | Plantar flexion (stand on tiptoe) |
| Sensory | Medial shin | Dorsum foot, big toe | Lateral foot, heel |
| Reflex | Knee jerk ↓ | Ankle jerk (sometimes) or absent | Ankle jerk ↓ |
| Quick test | Walk on heels (tests L4/L5) | Cannot lift big toe | Cannot stand on tiptoes |
| Disc | L3-L4 | L4-L5 | L5-S1 |
Memory hook:
- L4 = "4wards walking" = knee extension, heel walking
- L5 = "L5ft the foot up" = dorsiflexion, extensor hallucis longus (EHL)
- S1 = "S1 = Sole" = plantar flexion, ankle jerk
Clinical Provocation Tests for Lumbosacral Radiculopathy
| Test | Technique | Roots tested | Sens/Spec |
|---|---|---|---|
| Straight Leg Raise (SLR / Lasègue) | Supine, passively raise straight leg. Positive: radicular pain at 30-70° (NOT just back pain) | L5, S1 | Sensitivity 91%, specificity 26% |
| Crossed SLR | Raising the contralateral leg reproduces ipsilateral radicular pain | L5, S1 | Low sensitivity, high specificity (~90%) |
| Femoral Nerve Stretch Test | Prone, flex knee to 90°, extend hip. Positive: anterior thigh pain | L2, L3, L4 | For upper lumbar roots |
| Slump Test | Seated, slump forward + extend knee + dorsiflex ankle. Positive: sciatic pain | L5, S1 | High sensitivity |
| Bowstring Sign | After positive SLR, flex knee slightly - if pain returns with popliteal fossa pressure, positive | L5, S1 | High specificity |
Key from Rheumatology textbook: Femoral stretch test = L2/L3/L4; SLR/Bowstring = L5/S1
Mnemonic: "SLR for LOW (L5-S1 = low lumbar), Femoral for HIGH (L2-3-4 = upper lumbar)"
PART 3: RED FLAGS (Cauda Equina - Must Not Miss!)
Cauda equina syndrome = massive central disc herniation (usually L4/5 or L5/S1) compressing multiple roots:
- Bilateral leg pain/weakness
- Saddle anesthesia (S2-4 dermatome - perineum, inner thighs)
- Bladder retention or incontinence (most reliable sign)
- Anal sphincter laxity (loss of anal tone)
- Decreased/absent bilateral ankle jerks
"Saddle + Bladder = Emergency Surgery" - From Bradley and Daroff's and Textbook of Family Medicine: sphincter disturbance from lumbar disease requires urgent surgical consideration.
Historical red flags for any back pain:
- Fever, weight loss (infection/malignancy)
- History of cancer
- Bowel/bladder dysfunction (CES)
- Saddle anesthesia
- Bilateral leg weakness
- Recent major trauma
- IV drug use / immunosuppression
PART 4: DIAGNOSTIC INVESTIGATIONS
| Test | Radiculopathy Finding | Notes |
|---|---|---|
| MRI spine | Disc herniation or osteophyte compressing root | Investigation of choice |
| CT myelography | Same as MRI; better for calcified lesions, post-op patients | If MRI contraindicated |
| NCS | Normal SNAPs (lesion is preganglionic, proximal to DRG) | Differentiates from peripheral neuropathy |
| EMG (needle) | Fibrillations/PSWs in myotome distribution + paraspinals | Confirms radiculopathy; paraspinals are key |
| F-waves | May be delayed in affected root | Less sensitive |
| H-reflex | Absent/asymmetric = S1 radiculopathy (sensitivity 50%, specificity 91%) | Very specific for S1 |
Key NCS point for exams: In radiculopathy, the dorsal root ganglion (DRG) is outside the spinal canal, so sensory axons peripheral to the DRG are intact → SNAPs normal despite sensory symptoms. CMAPs may be reduced if significant motor axon loss. This distinguishes radiculopathy from peripheral neuropathy/plexopathy.
"Normal SNAP = preganglionic = radiculopathy" - Bradley and Daroff's Neurology
PART 5: MASTER MEMORY TABLE
Upper Limb Reflexes - "BiBoTri No" Mnemonic
C5 = Biceps (and Brachioradialis shares)
C6 = Brachioradialis (and Biceps shares)
C7 = Triceps (exclusive)
C8 = Nothing (no reflex)
Lower Limb Reflexes
L3-L4 = Patellar (knee jerk) → "kneecap = L34"
S1 = Achilles (ankle jerk) → "sole/ankle = S1"
PART 6: DERMATOMAL KEY LANDMARKS (USMLE/MRCP Favourites)
| Landmark | Root |
|---|---|
| Nipple line | T4 |
| Xiphoid process | T7 |
| Umbilicus | T10 |
| Groin / inguinal ligament | L1 |
| Anterior thigh | L2-L3 |
| Medial shin/knee | L4 |
| Dorsum of foot / big toe | L5 |
| Lateral foot / heel / sole | S1 |
| Perineum / saddle area | S2-S4 |
Thoracic landmarks mnemonic: "T4 = Tits (nipples), T10 = TEN = Tummy button (umbilicus)"
PART 7: HISTORY TAKING - THE RADICULOPATHY TEMPLATE
A structured history for FCPS/MRCP/USMLE OSCEs:
- Character of pain: burning, shooting, lancinating (neuropathic quality)
- Radiation: Does it radiate beyond the knee (lumbar) or elbow (cervical)?
- Aggravating factors: Cough/sneeze/Valsalva worsens → increased intrathecal pressure → radiculopathy
- Relieving factors: Arm raised above head relieves cervical pain (shoulder abduction relief sign)
- Duration and onset: Acute (disc) vs. gradual (spondylosis/stenosis)
- Neurological symptoms: Numbness, tingling in which finger/toe?
- Weakness: Specific activities - can't open jars (C8/T1), can't comb hair (C5), can't walk on tiptoes (S1), dragging foot (L5)
- Red flags: Bilateral, bowel/bladder, saddle numbness
Quick Summary Card for Exams
Cervical
- C5: Shoulder abduction weak, Biceps reflex ↓, lateral arm numb
- C6: Elbow flex + wrist extend weak, Brachioradialis reflex ↓, thumb/index numb - most common
- C7: Elbow extend weak, Triceps reflex ↓, middle finger numb
- C8: Finger flex weak, NO reflex, ring/little finger numb
- Spurling = high spec, ULTT = high sens
Lumbosacral
- L4: Quad/knee extend weak, Knee jerk ↓, medial shin numb, heel walk
- L5: Foot/big toe dorsiflex weak (EHL), ankle jerk sometimes ↓, dorsum foot/big toe numb
- S1: Plantar flex weak (calf), Ankle jerk ↓, lateral foot numb, tiptoe test
- SLR tests L5/S1 (high sens), Femoral stretch tests L2/L3/L4 (high spec)
- Cauda equina = saddle anesthesia + bladder = EMERGENCY
Sources: Bradley and Daroff's Neurology in Clinical Practice (cervical radiculopathy chapters); Textbook of Family Medicine 9e (spine physical examination tables); Lecturio medical illustrations; neurological examination evidence from PMC scoping review on cervical radiculopathy.
This is a shared conversation. Sign in to Orris to start your own chat.