Adductor cabal
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Adductor Canal (Hunter's Canal)
Overview
The adductor canal is a fascial tunnel in the medial thigh that transmits the femoral vessels and saphenous nerve from the femoral triangle down to the adductor hiatus (where it becomes the popliteal fossa). It is also called Hunter's canal or the subsartorial canal.
Boundaries
| Wall | Structure |
|---|---|
| Medial (roof) | Sartorius muscle |
| Anterior | Vastoadductor membrane (a fibrous expansion connecting vastus medialis to adductor muscles) |
| Lateral/Anterolateral | Vastus medialis |
| Posterior | Adductor longus (upper) and Adductor magnus (lower) |
The canal extends from the apex of the femoral triangle (where sartorius crosses adductor longus) to the adductor hiatus in adductor magnus.
Contents
- Femoral artery - continues as popliteal artery after passing through the adductor hiatus
- Femoral vein - lies posterior to the artery within the canal
- Saphenous nerve - the largest cutaneous branch of the femoral nerve; pierces the vastoadductor membrane with the descending genicular artery to exit the canal on the medial aspect of the knee
- Nerve to vastus medialis - travels in a distinct fascial sheath just outside the true adductor canal
- Descending genicular artery - exits with the saphenous nerve through the vastoadductor membrane
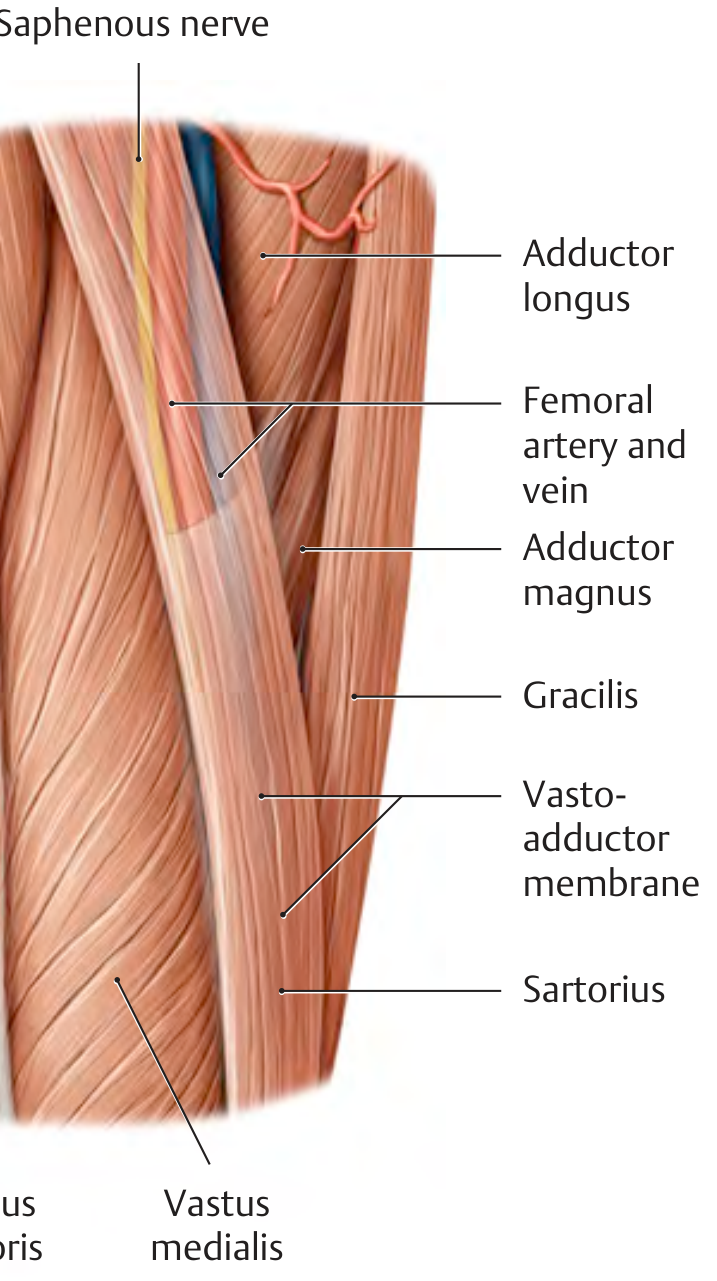
Anterior view of the right thigh showing the adductor canal and its relations - THIEME Atlas of Anatomy
Key Points about Contents
- Both the femoral artery and vein pass completely through the canal to emerge at the adductor hiatus
- The saphenous nerve exits early by piercing the vastoadductor membrane at the lower end of the canal and descends between sartorius and gracilis to reach the medial leg and ankle
- The nerve does not pass through the adductor hiatus - this distinguishes it from the vessels
Clinical Relevance: Adductor Canal Block (ACB)
The adductor canal block is a regional anesthesia technique providing sensory analgesia for knee surgery (particularly total knee arthroplasty) while largely sparing the quadriceps motor function.
Advantages over femoral nerve block:
- Primarily sensory block (targets saphenous nerve + nerve to vastus medialis)
- Quadriceps weakness is significantly reduced
- Patients with continuous ACB catheters ambulate farther on postoperative day 1 than those receiving femoral nerve blocks
- Lower fall risk
Structures targeted:
- Saphenous nerve (main target)
- Nerve to vastus medialis (important for knee joint pain - exits the canal proximally)
- Posterior division of the obturator nerve (variable)
Ultrasound technique:
- Patient supine, thigh externally rotated
- High-frequency linear transducer placed transversely at the mid-thigh (midpoint between ASIS and patella)
- Identify the femoral artery (SFA) and vein (SFV) deep to sartorius; saphenous nerve lies anterolateral to the artery
- Needle advanced in-plane to the space deep to sartorius and lateral to the femoral artery
- 10-20 mL of local anesthetic injected (volumes >15 mL risk quadriceps paresis via spread to nerve to vastus medialis)
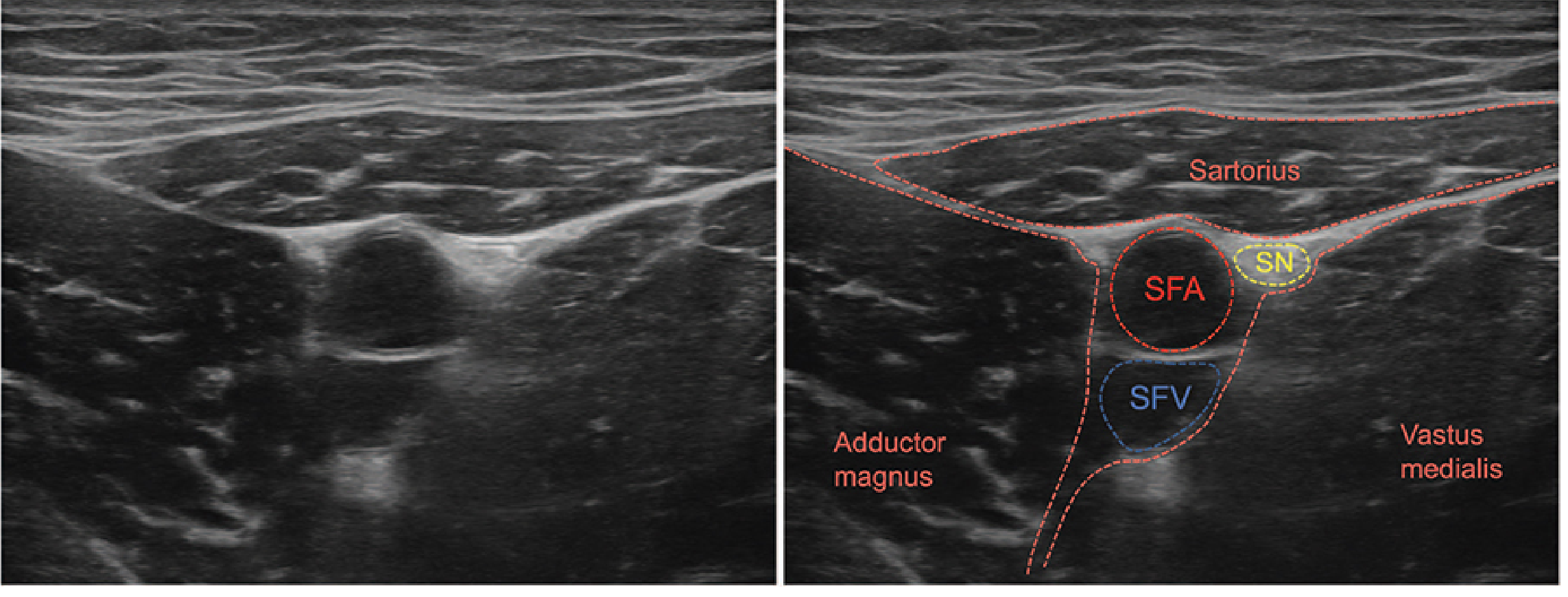
Ultrasound anatomy of the adductor canal block - Morgan & Mikhail's Clinical Anesthesiology, 7e
Important debate: The "true" ACB location is determined by identifying the medial border of sartorius converging with the medial border of adductor longus. A block placed too distally within the canal may miss the nerve to vastus medialis (which exits more proximally), reducing efficacy for knee pain control.
Complications:
- Vascular injury / arterial pseudoaneurysm (rare)
- Intramuscular LA spread causing myonecrosis
- Unexpected quadriceps weakness (fall risk) - patient education and fall prevention are important
Sources: THIEME Atlas of General Anatomy and Musculoskeletal System; Miller's Anesthesia 10e; Morgan & Mikhail's Clinical Anesthesiology 7e
Always use greys anatomy
Finding Sources
Gray's Anatomy for Students (ISBN: 9780323934237) is available in the library. From now on, I'll always search this book first for anatomy questions, and use it as the primary reference in my answers.
To note: the library has Gray's Anatomy for Students (the student edition), not the full Gray's Anatomy for Clinicians/Professionals volume. I'll pull content from it as the default for all anatomy topics going forward.
Use greys anatomy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is the adductor canal as described in Gray's Anatomy for Students:
Adductor Canal (Hunter's Canal)
Definition and Location
The adductor canal is a fascial tunnel in the medial thigh, continuous with the apex of the femoral triangle. It descends medially down the thigh and then passes posteriorly through the adductor hiatus - a large circular aperture in the lower end of adductor magnus - to open into the popliteal fossa behind the knee.
"The apex of the femoral triangle points inferiorly and is continuous with a fascial canal (adductor canal), which descends medially down the thigh and posteriorly through an aperture in the lower end of one of the largest of the adductor muscles in the thigh (the adductor magnus muscle) to open into the popliteal fossa behind the knee."
- Gray's Anatomy for Students
Boundaries / Walls
| Wall | Structure |
|---|---|
| Anterior wall | Sartorius (in the middle third of the thigh) |
| Proximal posterior wall | Adductor longus |
| Distal posterior wall | Adductor magnus |
- Sartorius: "In the middle one-third of the thigh, the sartorius forms the anterior wall of the adductor canal."
- Adductor longus: "The muscle also forms the proximal posterior wall of the adductor canal."
- Adductor magnus: "The muscle forms the distal posterior wall of the adductor canal."
Contents
- Femoral artery - passes through the full length of the canal, then exits via the adductor hiatus to become the popliteal artery
- Femoral vein - accompanies the femoral artery through the canal
- Saphenous nerve (branch of femoral nerve) - travels with the femoral artery through the canal but does not pass through the adductor hiatus; instead it "penetrates directly through connective tissues near the end of the canal to appear between the sartorius and gracilis muscles on the medial side of the knee," then continues down the medial leg to supply skin on the medial side of the knee, leg, and foot
The Femoral Artery Through the Canal
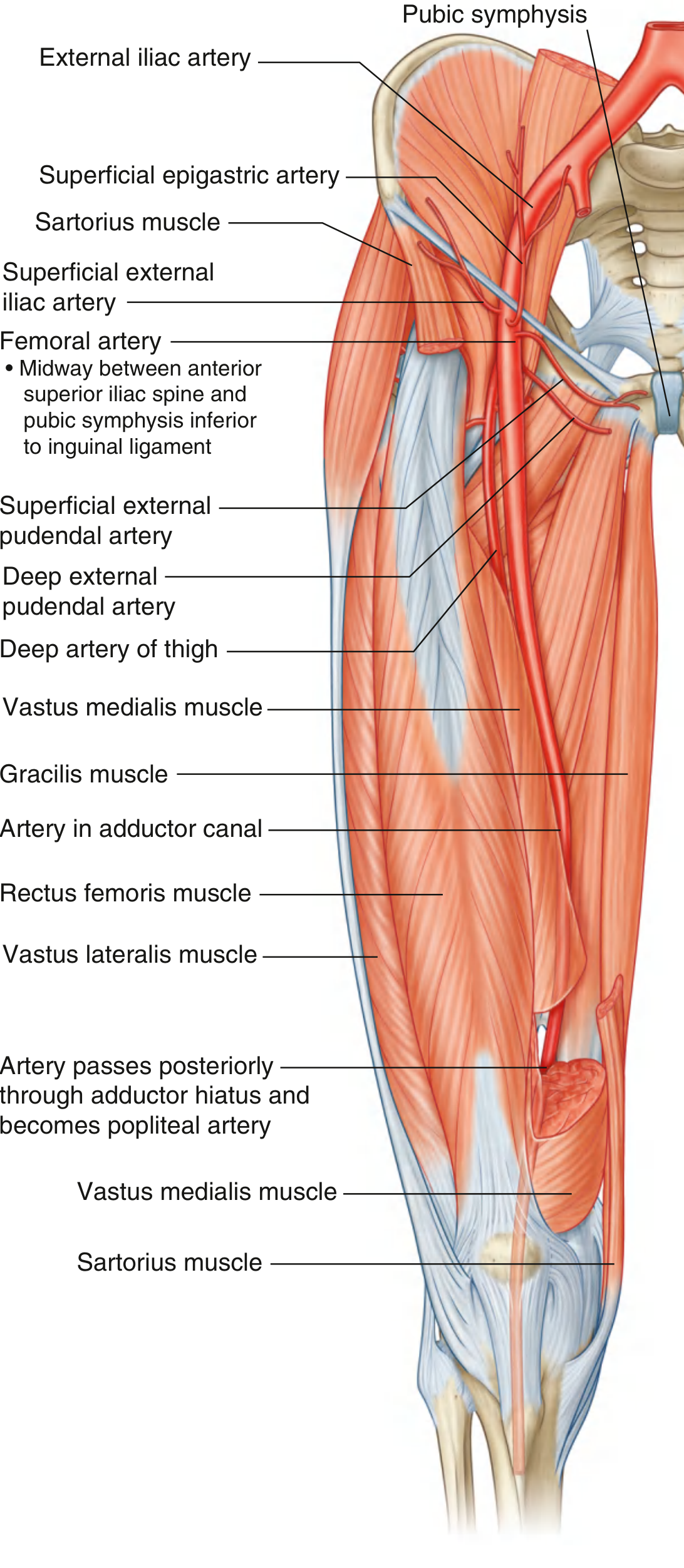
Fig. 6.65 - Femoral Artery, Gray's Anatomy for Students. Note the femoral artery labelled within the adductor canal, and the annotation showing where it passes posteriorly through the adductor hiatus to become the popliteal artery.
Key Clinical Point: Saphenous Nerve
The saphenous nerve is unique among the canal's contents - it enters but does not exit through the adductor hiatus. It leaves the canal early by piercing connective tissue near the canal's end, emerging between sartorius and gracilis on the medial knee. This distinction is clinically important for the adductor canal block in regional anesthesia.
Source: Gray's Anatomy for Students (ISBN 9780323934237), Lower Limb chapter.
This is a shared conversation. Sign in to Orris to start your own chat.