Describe anatomy and physiology of lens
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Anatomy and Physiology of the Lens
Overview
The lens is a transparent, biconvex, avascular structure located immediately behind the iris in the posterior chamber of the eye. Its principal function is to focus light precisely on the retina by adjusting its curvature - a process called accommodation. It contributes approximately +15 to +20 diopters of the eye's total refractive power (~60 D total), with the remainder provided by the cornea.
Embryological Development
The lens develops entirely from the surface ectoderm. During eye development, the optic vesicle (outgrowth of the developing brain) contacts the overlying surface ectoderm and induces it to thicken into a lens placode. This placode invaginates to form the lens vesicle, which pinches off from the surface ectoderm.
- The anterior wall of the vesicle (cuboidal epithelium) becomes the subcapsular lens epithelium
- The tall columnar cells of the posterior wall elongate, lose their nuclei, and become the primary lens fibers, obliterating the central cavity
- At the equatorial zone, cuboidal epithelial cells continue to proliferate throughout life, elongate, lose nuclei, and become secondary lens fibers - these are continuously added around the primary fibers
Key transcription factors required: PAX6, SOX2 (lens induction); PITX3, GATA3, FOXE3 (lens fiber differentiation).
During fetal development, the lens is supplied by the hyaloid artery via the tunica vasculosa lentis. This vascular supply degenerates in the late fetal period; thereafter the lens is entirely avascular and depends on diffusion from aqueous humor (anteriorly) and vitreous humor (posteriorly).
- The Developing Human: Clinically Oriented Embryology, p. 1136
Structural Anatomy
1. Lens Capsule
The outermost layer is a very thick (10-20 μm), homogeneous external lamina composed of proteoglycans and type IV collagen. It surrounds the entire lens and is the thickest basement membrane in the body. It originates as the basement membrane of the invaginating lens vesicle and provides the attachment site for the microfibrils of the ciliary zonule (suspensory ligaments).
2. Lens Epithelium (Subcapsular Epithelium)
A single layer of cuboidal cells present only on the anterior surface of the lens (not the posterior surface). Key features:
- Basal ends attach to the lens capsule; apical surfaces bind to the internal lens fibers
- These cells are metabolically active - they carry out the bulk of the lens's oxidative metabolism and active transport
- At the equatorial region (germinative zone), cells undergo mitosis to produce new cells that differentiate into lens fibers - this continues at a slow, decreasing rate throughout life
3. Lens Fibers
The bulk of the lens is composed of highly elongated, terminally differentiated cells called lens fibers:
- Each fiber is typically 7-10 mm long with a 2 × 8 μm cross-section
- During differentiation, the cytoplasm fills with crystallins (structural proteins unique to the lens)
- Followed by autophagy of all organelles including the nucleus - this elimination is required to avoid light scattering
- Packed tightly together in a hexagonal arrangement to form a perfectly transparent refractive tissue
- Older fibers are buried deeper (nucleus of the lens); newer fibers are more peripheral (cortex)
Histological appearance (H&E): Shows lens capsule (LC) outermost, then the single-layer lens epithelium (LE), then differentiating lens fibers (DLF) still retaining nuclei, and finally mature lens fibers (MLF) with no nuclei, densely packed.

- Junqueira's Basic Histology, p. 1191-1193
Crystallins
Crystallins are the dominant structural proteins of the lens (~90% of total protein), responsible for the high refractive index and optical transparency. The main types are:
- α-crystallins - also act as molecular chaperones, preventing protein aggregation
- β-crystallins and γ-crystallins - structural proteins
With aging, crystallins may denature and aggregate, causing opacity - this is the basis of cataract formation. Exposure to ultraviolet radiation, trauma, diabetes mellitus, and hypertension accelerate this process.
Gross Dimensions and Position
| Feature | Detail |
|---|---|
| Shape | Biconvex |
| Diameter | ~9-10 mm (equatorial) |
| Thickness | ~4 mm (increases during accommodation) |
| Anterior radius of curvature | ~10 mm (at rest) |
| Posterior radius of curvature | ~6 mm (more curved) |
| Location | Posterior chamber, behind iris, in front of vitreous |
| Suspension | Ciliary zonule (zonule of Zinn) |
Zonule of Zinn (Ciliary Zonule)
The lens is suspended centrally within the eye by the ciliary zonule, which consists of fine microfibrils (fibrillin-based) arising from the ciliary body and attaching to the lens capsule at the equatorial region. These zonular fibers (suspensory ligaments) transmit the forces of ciliary muscle contraction/relaxation to change lens shape.
- Junqueira's Basic Histology, p. 1192-1195
Physiology
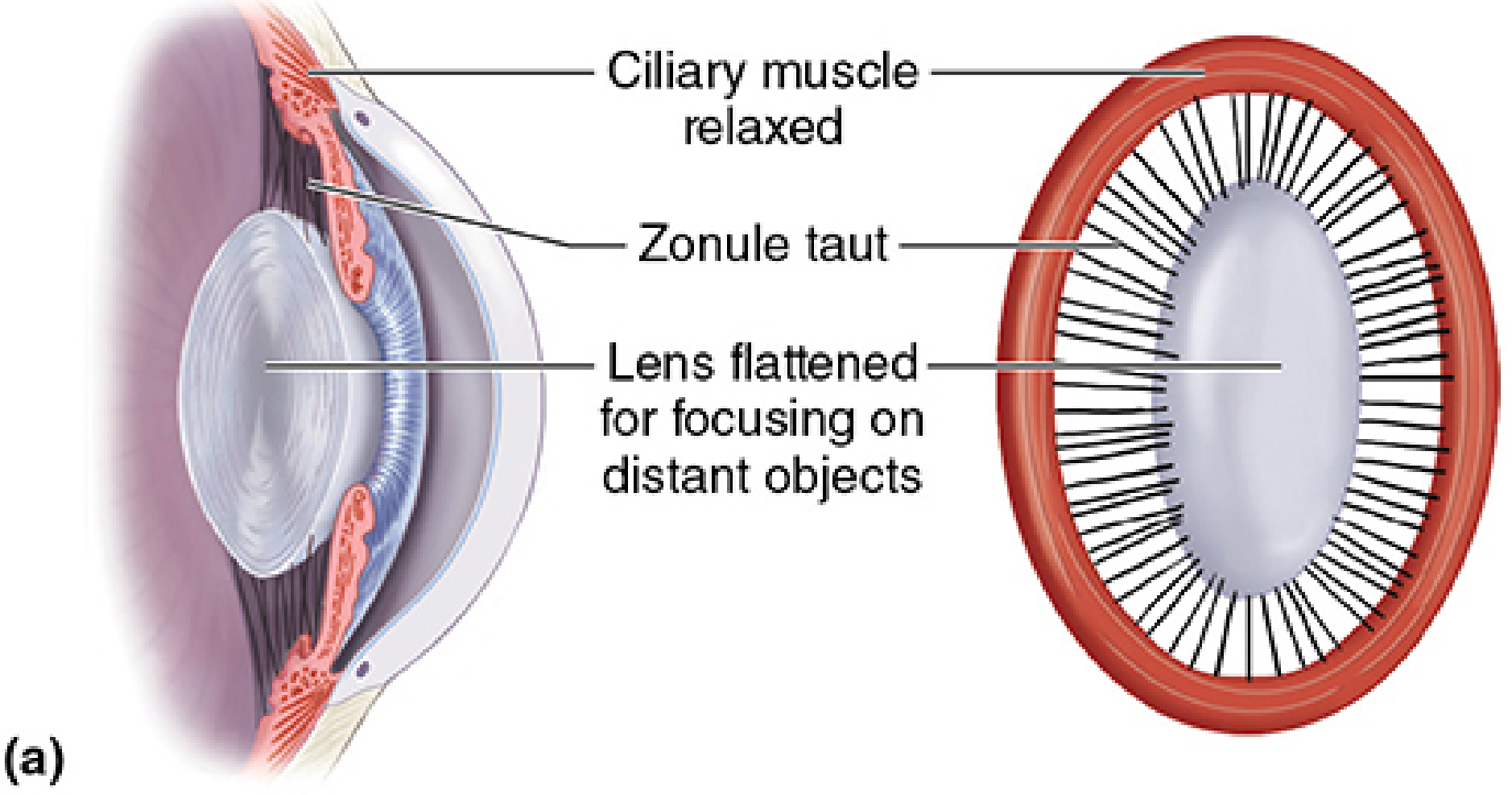
Accommodation
Accommodation is the ability of the lens to change its curvature to focus on objects at different distances. It operates via the ciliary muscle-zonule-lens unit:
For distant vision (distance focus):
- Ciliary muscle relaxes
- Ciliary body ring widens outward
- Zonular fibers become taut (under tension)
- Lens is pulled flat (reduced curvature) → lower refractive power
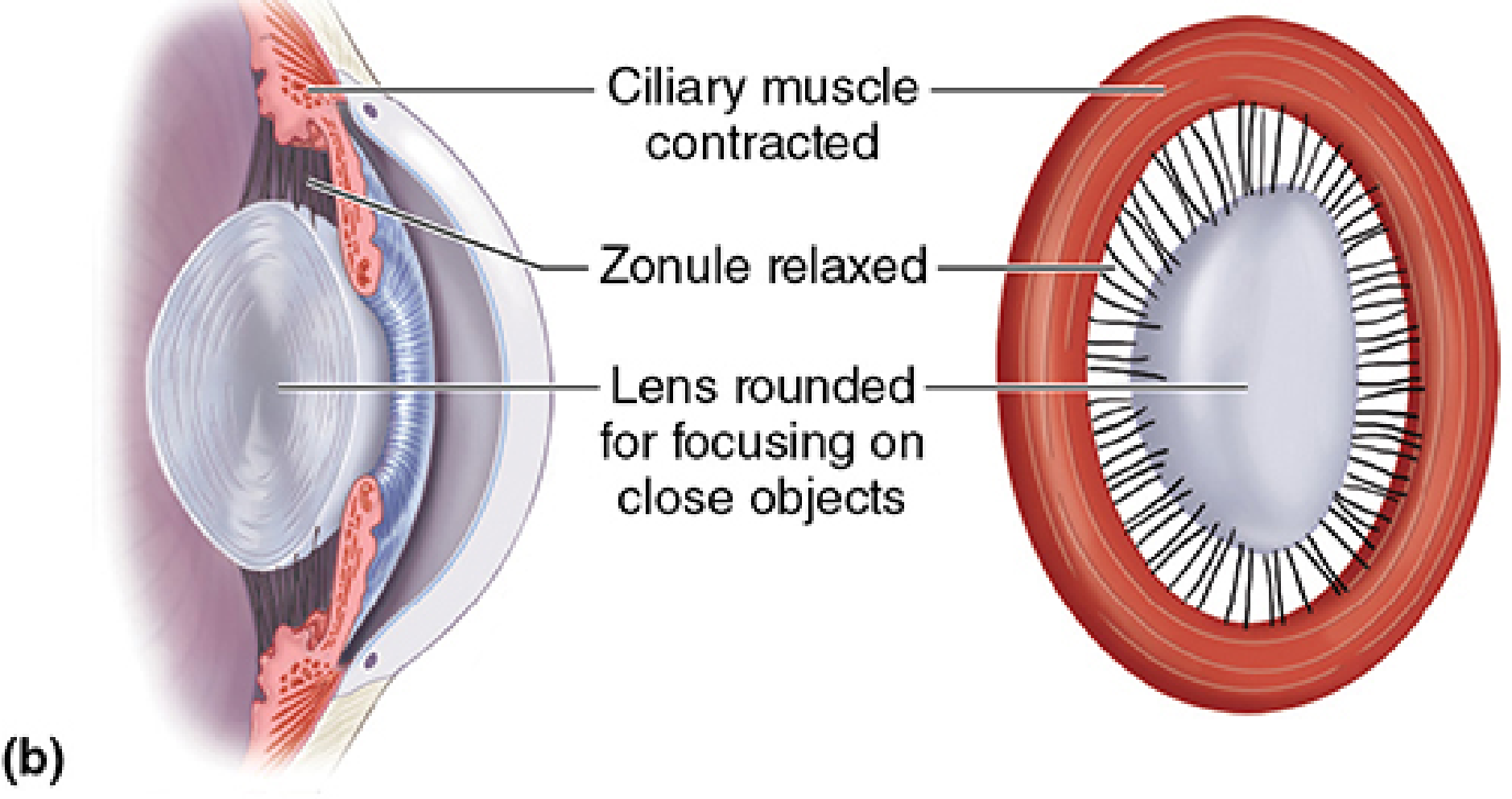
For near vision (near focus):
- Ciliary muscle contracts and swells inward
- Ring diameter decreases (smaller hole inside the ciliary ring)
- Tension on zonular fibers decreases
- Lens assumes a rounder, more spherical shape due to its inherent elasticity → increased refractive power
- Neuroscience: Exploring the Brain, 5th ed., p. 839
Presbyopia
With aging, the lens gradually loses elasticity because of ongoing addition of lens fibers and stiffening of the crystallin-filled core. By middle age (~45 years), accommodation decreases markedly - the lens can no longer become sufficiently rounded to focus on near objects. This condition is presbyopia, corrected with convex reading glasses.
An infant can focus on objects just a few centimeters away; many middle-aged adults cannot focus clearly on objects closer than arm's length. Presbyopia is not a refractive error - it is a loss of accommodative reserve.
- Neuroscience: Exploring the Brain, 5th ed., p. 839
Nutrition and Metabolism
Because the lens is entirely avascular, it relies on:
- Aqueous humor - bathes the anterior surface and provides glucose, amino acids, ascorbate, and oxygen
- Vitreous humor - supplies the posterior surface
The lens epithelial cells carry out the primary metabolic work:
- Anaerobic glycolysis - the predominant pathway for ATP generation (even though oxygen is available, the lens uses glycolysis preferentially to minimize reactive oxygen species)
- Active transport (Na⁺/K⁺-ATPase) - maintains ionic homeostasis critical for transparency. The lens interior is high in K⁺ and low in Na⁺ relative to extracellular fluid
- Sorbitol pathway (polyol pathway) - in diabetics, excess glucose is converted to sorbitol by aldose reductase in the lens, causing osmotic swelling and cataract
Transparency
The extraordinary optical clarity of the lens depends on:
- Elimination of all organelles from mature fiber cells (no light-scattering particles)
- Short-range order in crystallin packing - proteins are packed so densely and regularly that destructive interference prevents light scattering
- Maintenance of cellular dehydration - Na⁺/K⁺-ATPase keeps water content low (~65%)
- Antioxidant systems - high concentrations of glutathione protect crystallins from oxidative aggregation
Age-Related Changes Summary
| Age | Change |
|---|---|
| Infancy | Maximum accommodation (~14 D near point); soft, maximally elastic lens |
| Adulthood | Gradual stiffening; accommodation decreases |
| Middle age (45+) | Presbyopia onset; reduced near focus |
| Older age | Crystallin denaturation/aggregation → nuclear sclerosis → cataract |
Clinical Correlates
-
Cataract: Opacity of the lens fibers due to crystallin denaturation. Causes: UV exposure, trauma, diabetes, steroids, aging. Treated surgically by phacoemulsification (ultrasonic emulsification + aspiration), with implantation of an intraocular lens (IOL) into the residual capsular bag
-
Lens subluxation/dislocation: Disruption of zonular fibers (from trauma, Marfan syndrome, homocystinuria, pseudoexfoliation) causes lens to shift, producing uniocular diplopia, iridodonesis, and phakodonesis
-
Posterior subcapsular cataract: Classic pattern with steroid use (systemic or topical) and in diabetics
-
Congenital lens anomalies: Persistent pupillary membrane, congenital cataract, lens coloboma (associated with PAX6 mutations)
-
Junqueira's Basic Histology, p. 1194; Kanski's Clinical Ophthalmology, p. 914, 932; The Developing Human, p. 1136
This is a shared conversation. Sign in to Orris to start your own chat.