Drugs used in peptic ulcer - classify pharmacology basic of uses
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
Drugs Used in Peptic Ulcer Disease - Classification & Pharmacology
Pathophysiological Basis
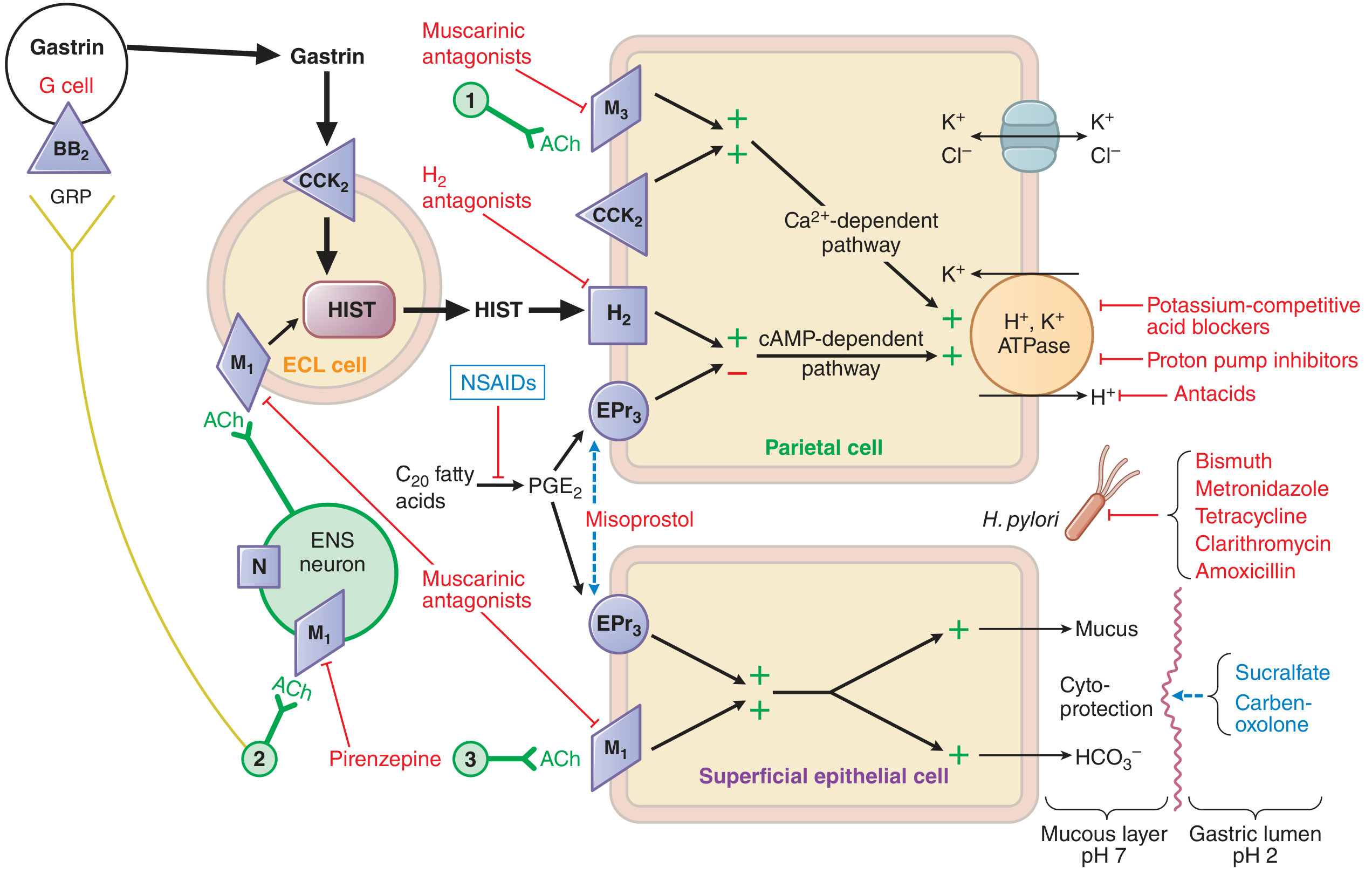
Peptic ulcer results from an imbalance between aggressive factors (acid, pepsin, H. pylori, NSAIDs) and defensive factors (mucus, bicarbonate, prostaglandins, mucosal blood flow). Drug therapy targets one or more of these components.
Classification of Anti-Ulcer Drugs
Group I - Drugs That Reduce Acid (Antisecretory Agents)
A. Proton Pump Inhibitors (PPIs) - Drug of Choice
| Drug | Dose |
|---|---|
| Omeprazole | 20-40 mg OD |
| Esomeprazole (S-isomer of omeprazole) | 20-40 mg OD |
| Lansoprazole | 15-30 mg OD |
| Dexlansoprazole (R-enantiomer) | 30-60 mg OD |
| Pantoprazole | 40 mg OD |
| Rabeprazole | 20 mg OD |
Mechanism: PPIs are prodrugs that require acid for activation. After oral absorption, they diffuse into parietal cell secretory canaliculi, where acid converts them to a tetracyclic sulfenamide (the active form). This irreversibly binds covalently to sulfhydryl groups of cysteines on H⁺/K⁺-ATPase (the proton pump), blocking the final common pathway of acid secretion regardless of the stimulus (histamine, gastrin, or ACh).
Key pharmacology points:
- Given before the first meal (H⁺/K⁺-ATPase increases after fasting; meal activates pumps)
- Plasma t½ ~0.5-3 h, but acid suppression lasts 24-48 hours (new pump synthesis needed to restore secretion)
- Enteric-coated / delayed-release formulations protect drug from premature acid degradation
- Rebound acid hypersecretion occurs on stopping long-term PPI therapy
- Omeprazole inhibits CYP2C19 - relevant drug interaction with clopidogrel
- IV forms available: esomeprazole sodium, omeprazole sodium, pantoprazole
B. H₂ Receptor Antagonists (H₂RAs)
| Drug | Notes |
|---|---|
| Famotidine | Preferred (least drug interactions) |
| Cimetidine | First H₂RA; now limited use (CYP inhibitor) |
| Ranitidine | Withdrawn from market (NDMA contamination) |
| Nizatidine | Fewest CYP interactions |
Mechanism: Competitively block histamine at H₂ receptors on parietal cells, reducing cAMP-dependent acid secretion. Histamine from ECL cells is the primary amplifier of acid secretion (gastrin and ACh work partly via histamine), so H₂RAs reduce acid from all three stimuli, though less completely than PPIs.
Key pharmacology points:
- Oral bioavailability good; peak levels in 1-3 h
- Duration: famotidine 10-12 h > ranitidine 6-8 h > cimetidine 4-5 h
- Tolerance develops within 3 days (secondary hypergastrinemia stimulates ECL histamine release)
- Cimetidine - inhibits CYP1A2, CYP2C9, CYP2D6; causes gynecomastia and impotence (anti-androgenic); crosses placenta
- Dose reduction needed in renal failure (renally excreted)
- Less potent than PPIs but useful in pregnancy and mild GERD
C. Potassium-Competitive Acid Blockers (P-CABs) - Newer Class
- Vonoprazan, Revaprazan, Tegoprazan
- Mechanism: Weak bases that accumulate in parietal cell canaliculi and competitively, reversibly block the K⁺-binding site of H⁺/K⁺-ATPase (unlike PPIs which are irreversible). Can bind both active and inactive pump forms.
- Advantages over PPIs: faster onset (effect on day 1), longer duration, no requirement for acid activation, food-independent dosing, less CYP2C19 variability
- Currently licensed mainly in Asia; vonoprazan trials ongoing in USA/Europe
D. Anticholinergics (Muscarinic Antagonists)
- Pirenzepine (selective M₁ antagonist) - blocks ACh stimulation of parietal cells and ECL cells
- Reduces acid secretion but less effective than PPIs or H₂RAs
- Side effects: dry mouth, blurred vision, urinary retention (typical anticholinergic)
- Largely replaced by PPIs; still used occasionally as add-on therapy
Group II - Drugs That Neutralize Acid (Antacids)
React chemically with HCl in the gastric lumen to raise pH and inactivate pepsin (pepsin inactive at pH >4).
| Drug | Type | Notes |
|---|---|---|
| Magnesium hydroxide Mg(OH)₂ | Non-systemic | Fast-acting; causes diarrhea |
| Aluminium hydroxide Al(OH)₃ | Non-systemic | Slower; causes constipation |
| Calcium carbonate CaCO₃ | Non-systemic | Potent, rapid; "acid rebound" with high doses |
| Sodium bicarbonate NaHCO₃ | Systemic | Rapid but short-acting; systemic alkalosis risk |
| Magaldrate (Al-Mg combination) | Non-systemic | Balanced bowel effects |
- Provide rapid symptom relief; used as needed
- Reduce absorption of many drugs (tetracyclines, fluoroquinolones, iron) - give 2 hours apart
- Systemic antacids (NaHCO₃) avoided in renal failure and hypertension
- Mg/Al combinations balance diarrhea vs. constipation
Group III - Cytoprotective Agents
A. Sucralfate
- Mechanism: In acidic pH, polymerizes to form a sticky gel that coats and adheres to ulcer base (especially proteins/fibrin in the ulcer crater), creating a physical barrier against acid and pepsin. Also stimulates mucus and bicarbonate secretion; enhances prostaglandin synthesis.
- Minimal systemic absorption - very safe
- Requires acidic pH to work - do NOT give with PPIs/antacids simultaneously
- Constipation is main side effect; reduces absorption of fluoroquinolones, digoxin, phenytoin
- Given 30 min before meals and at bedtime
B. Misoprostol (Prostaglandin E₁ analogue)
- Mechanism: Binds EP₃ prostanoid receptors on parietal cells → decreases cAMP → reduces acid secretion. Also binds EP₃ on superficial epithelial cells → increases mucus and bicarbonate secretion (cytoprotection).
- Main use: Prevention of NSAID-induced ulcers (replaces PGE₂ that NSAIDs deplete)
- Side effects: diarrhea (dose-limiting), abdominal cramps, uterine contractions
- Contraindicated in pregnancy (abortifacient - used in medical abortion protocols)
C. Bismuth Compounds
- Colloidal bismuth subcitrate (CBS), bismuth subsalicylate
- Mechanism: Coat ulcer base (like sucralfate); also have direct anti-H. pylori activity (inhibit bacterial enzymes, disrupt cell wall)
- Stimulate mucus and bicarbonate secretion
- Blacken stools and tongue (warn patients)
- Included in H. pylori eradication regimens (bismuth quadruple therapy)
- Risk of bismuth encephalopathy with prolonged high-dose use
D. Carbenoxolone
- Derivative of liquorice; enhances mucus secretion, increases mucosal cell turnover
- Side effects: sodium retention, hypokalemia, hypertension (mineralocorticoid-like)
- Largely obsolete; replaced by more effective agents
Group IV - Anti-H. pylori Regimens
H. pylori causes ~90% of duodenal and ~70% of gastric ulcers. Eradication is essential for cure.
Standard Triple Therapy (7-14 days)
- PPI (standard dose BD) + Clarithromycin 500 mg BD + Amoxicillin 1 g BD
- First-line in low clarithromycin-resistance areas
Bismuth Quadruple Therapy (14 days)
- PPI + Bismuth + Metronidazole + Tetracycline
- Used where clarithromycin resistance is high, or as rescue therapy
Sequential Therapy
- PPI + Amoxicillin for 5 days, then PPI + Clarithromycin + Metronidazole for 5 days
Levofloxacin-based Triple Therapy
- PPI + Levofloxacin + Amoxicillin (rescue regimen)
Antibiotic mechanisms:
- Clarithromycin - macrolide, inhibits 50S ribosome
- Amoxicillin - β-lactam, inhibits cell wall synthesis
- Metronidazole - activated in anaerobic bacteria, damages DNA
- Tetracycline - inhibits 30S ribosome
- Bismuth - direct bactericidal (inhibits urease, disrupts cell wall)
Summary Table
| Class | Example | Primary Target |
|---|---|---|
| PPI | Omeprazole | H⁺/K⁺-ATPase (irreversible) |
| P-CAB | Vonoprazan | H⁺/K⁺-ATPase (competitive) |
| H₂RA | Famotidine | H₂ receptor on parietal cell |
| Anticholinergic | Pirenzepine | M₁ receptor |
| Antacid | Mg(OH)₂ | Neutralizes luminal HCl |
| Sucralfate | Sucralfate | Ulcer coating / cytoprotection |
| Misoprostol | Misoprostol | EP₃ receptor (cytoprotection) |
| Bismuth | CBS | Coating + anti-H. pylori |
| Antibiotics | Clarithromycin | H. pylori eradication |
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Chapter 53 (Acid-Peptic Diseases)
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 63
- Lippincott Illustrated Reviews: Pharmacology
- Goodman & Gilman, H₂ receptor antagonists, p. 1076-1098
This is a shared conversation. Sign in to Orris to start your own chat.