Ards
Reading File
Finding Sources
Searching PubMed
"acute respiratory distress syndrome"[MeSH Terms] AND management
Finding Sources
Searching PubMed
"acute respiratory distress syndrome" AND treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material to write a thorough ARDS overview. Let me compose the final answer.
Acute Respiratory Distress Syndrome (ARDS)
Definition - Berlin Criteria (2012)
The Berlin definition replaced the older 1994 AECC criteria and requires all of the following:
| Criterion | Details |
|---|---|
| Timing | Onset within 1 week of a known clinical insult, or new/worsening respiratory symptoms over the past week |
| Chest imaging | Bilateral opacities on CXR or CT not fully explained by effusions, collapse, or nodules |
| Cause of edema | Respiratory failure not fully explained by cardiac failure or fluid overload (exclude cardiogenic edema, using echo if no clear ARDS risk factor) |
| Hypoxemia | Stratified by PaO2/FiO2 (P/F ratio) on PEEP/CPAP ≥5 cm H2O |
Severity classification by P/F ratio:
- Mild ARDS: P/F 201-300 mmHg
- Moderate ARDS: P/F 101-200 mmHg
- Severe ARDS: P/F ≤100 mmHg
Severity correlates with mortality: ~27% mild, ~32% moderate, ~45% severe, and also with duration of mechanical ventilation (5, 7, and 9 days respectively). - Murray & Nadel's Textbook of Respiratory Medicine
Epidemiology & Risk Factors
Direct (pulmonary) causes:
- Pneumonia (most common)
- Aspiration of gastric contents
- Pulmonary contusion
- Inhalation injury
Indirect (extrapulmonary) causes:
- Sepsis (most common overall trigger)
- Major trauma
- Severe pancreatitis
- Blood product transfusions (TRALI)
- Shock/hypotension
- Burns
Pathophysiology
Alveolar-Capillary Barrier Injury
ARDS is fundamentally a disorder of increased alveolar-capillary permeability resulting in non-cardiogenic pulmonary edema. The Starling equation governs fluid exchange; in ARDS, increased permeability (Lp) allows massive protein-rich fluid flux into the interstitium and alveolar spaces that overwhelms lymphatic drainage capacity.
Key cellular events:
- Alveolar epithelial injury - disrupts barrier integrity, prevents alveolar fluid clearance, and impairs surfactant production. Type I pneumocytes (covering 90% of alveolar surface) are highly vulnerable; type II cells (surfactant-producing, progenitor cells) are more resistant but also damaged.
- Pulmonary vascular endothelial injury - loss of endothelial barrier integrity is both necessary and sufficient to produce ARDS.
- Neutrophil-mediated damage - activated neutrophils release reactive oxygen species, proteases (including elastase which degrades surfactant-A protein), and proinflammatory cytokines.
- Surfactant dysfunction - qualitative (reduced dipalmitoylphosphatidylcholine) and quantitative (decreased large active aggregates) changes impair alveolar stability and promote collapse.
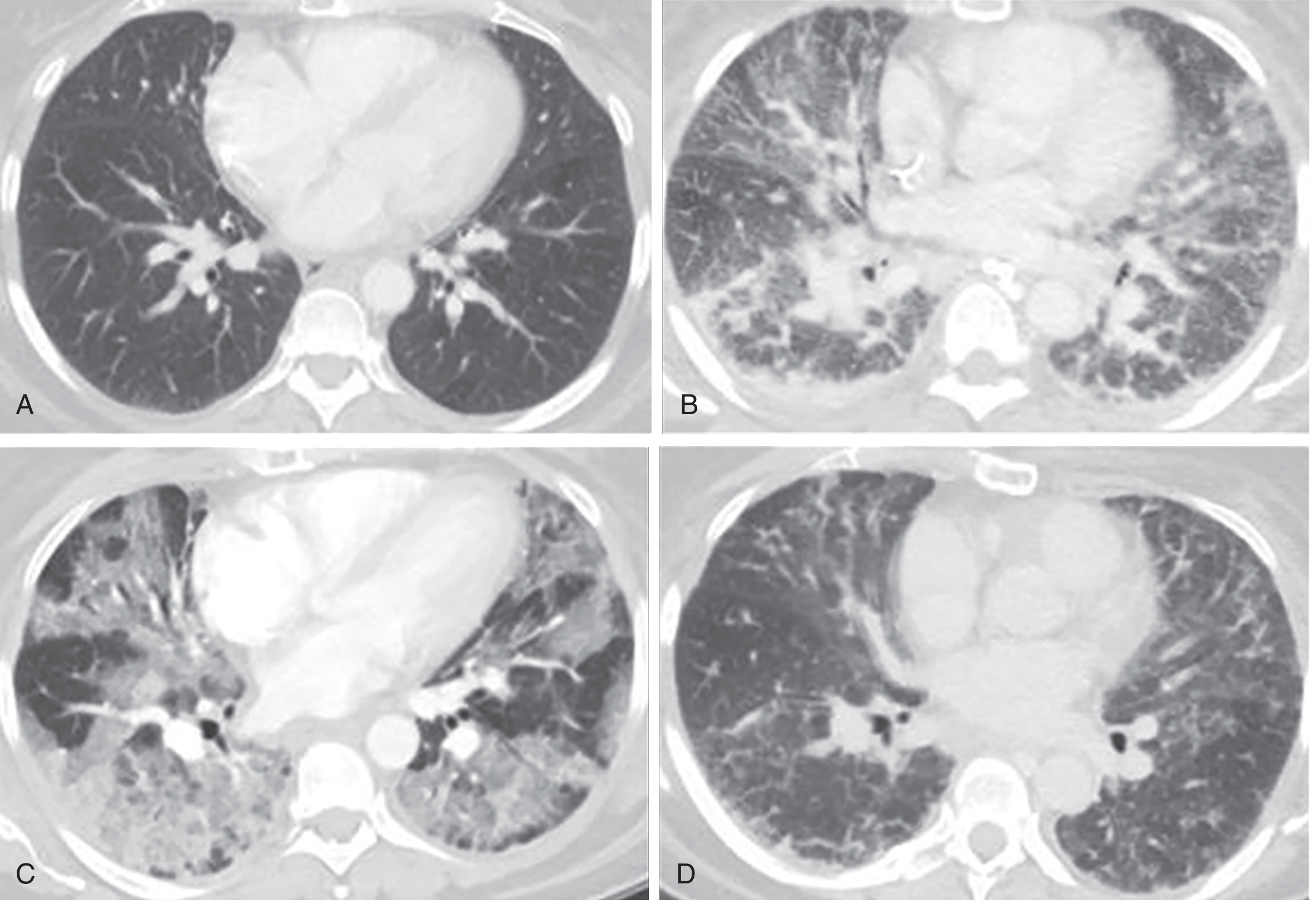
Phases of ARDS
Three histological/radiological phases occur:
- Exudative phase (days 1-7): Diffuse alveolar damage, protein-rich edema, hyaline membrane formation, neutrophil influx, bilateral ground-glass opacities on CT.
- Proliferative phase (days 7-21): Type II pneumocyte proliferation, early fibrosis, organization of exudate.
- Fibrotic phase (weeks-months, in some patients): Progressive fibrosis with residual architectural distortion; linear and reticular opacities on CT.
These CT phases are illustrated below:
Ventilator-Induced Lung Injury (VILI)
A major complication of managing ARDS is that the ventilator itself causes additional injury through two mechanisms:
- Volutrauma/barotrauma - overdistension of already-open alveoli at high lung volumes
- Atelectrauma - repeated collapse and recruitment of unstable alveoli at low lung volumes
This drives the rationale for lung-protective ventilation. - Goldman-Cecil Medicine
Management
1. Lung-Protective Mechanical Ventilation (Cornerstone)
Based on the landmark ARDSNet trial (ARMA), the standard ventilatory targets are:
| Parameter | Target |
|---|---|
| Tidal volume (Vt) | 6-8 mL/kg predicted body weight (PBW) |
| Plateau pressure | ≤30 cm H2O |
| PEEP | Titrated to oxygenation (minimizes atelectrauma) |
| PaO2 | 55-80 mmHg |
| SpO2 | 88-95% |
| pH | 7.30-7.45 (permissive hypercapnia accepted) |
The mode is typically volume-controlled assist-control ventilation. Permissive hypercapnia is accepted to limit plateau pressures. - Sabiston Textbook of Surgery
2. PEEP Strategy
Higher PEEP reduces atelectrauma and improves oxygenation but can worsen hemodynamics and overinflate compliant lung units. Titration is done using FiO2/PEEP tables per the ARDSNet algorithm or via individualized approaches (esophageal manometry, lung recruitment assessment).
3. Prone Positioning
Proven to reduce mortality in moderate-severe ARDS (P/F <150). The PROSEVA trial showed a 28-day mortality reduction from 32.8% to 16% with 16+ hours/day of prone positioning applied early. It redistributes perfusion, recruits dorsal lung regions, and improves V/Q matching. It requires experienced personnel and careful coordination. - Sabiston Textbook of Surgery; Murray & Nadel's
4. Fluid Management
A conservative fluid strategy (targeting a lower CVP/PCWP) reduces the number of ventilator days compared to a liberal strategy (FACTT trial), without increasing non-pulmonary organ failure. Diuresis to reduce extravascular lung water is a sensible early step.
5. Neuromuscular Blockade
Cisatracurium infusion for 48 hours in early moderate-severe ARDS was associated with improved outcomes in the ACURASYS trial, thought to be due to elimination of ventilator asynchrony and reduction in respiratory muscle oxygen consumption. The ROSE trial subsequently showed no benefit in an era of lighter sedation - the debate continues. Deep sedation alone may suffice if ventilator synchrony is achieved.
6. ECMO
Venovenous ECMO is the salvage option for refractory ARDS (P/F <80 despite optimal conventional management). The CESAR trial showed benefit from referral to ECMO centers. The EOLIA trial showed a non-significant mortality reduction that was stopped early - its interpretation remains debated. ECMO provides gas exchange rest while the lungs recover. - Sabiston Textbook of Surgery
7. Corticosteroids
- Early ARDS: Methylprednisolone may improve oxygenation and reduce ventilator days but mortality benefit is uncertain. The 2024 updated SCCM guidelines conditionally recommend corticosteroids in ARDS. [PMID 38240492]
- Late ARDS (>14 days): ARDSNet trial showed a harmful effect when steroids were started after day 14 (increased 60- and 180-day mortality) - avoid late initiation.
8. Interventions With NO Mortality Benefit
The following improve oxygenation transiently but have not shown survival benefit in large RCTs:
- Inhaled nitric oxide (transient oxygenation improvement in 60%, no survival benefit)
- Inhaled prostacyclin (well tolerated as rescue, no RCT mortality data)
- Exogenous surfactant (4 large RCTs negative)
- High-frequency oscillatory ventilation (OSCAR/OSCILLATE - no benefit, possible harm)
- β2-adrenergic agonists (BALTI-2 - no benefit)
- Inverse ratio ventilation
Murray Lung Injury Score
An older quantitative tool sometimes used to characterize severity:
| Parameter | Score 0-4 |
|---|---|
| Chest radiograph infiltrates (0-4 quadrants) | 0-4 |
| P/F ratio (>300 to ≤100) | 0-4 |
| PEEP level (≤5 to >15 cm H2O) | 0-4 |
| Respiratory system compliance (>80 to <19 mL/cm H2O) | 0-4 |
Score = sum / 4. Score >2.5 suggests severe ARDS. - Current Surgical Therapy 14e
Prognosis & Outcomes
- Overall mortality ranges from 27-45% depending on severity; survivors often have prolonged ICU stays.
- Most survivors recover to near-normal lung function within 6-12 months, but significant long-term sequelae exist including cognitive impairment, post-traumatic stress disorder, muscle weakness, and reduced quality of life (post-intensive care syndrome).
- Patients who develop the fibrotic phase have prolonged ventilator dependence and worse prognosis.
- Reduced functional residual capacity (FRC) and decreased lung compliance are the hallmark physiological abnormalities.
Key references:
- Murray & Nadel's Textbook of Respiratory Medicine (primary)
- Fishman's Pulmonary Diseases and Disorders
- Goldman-Cecil Medicine
- Sabiston Textbook of Surgery
- Current Surgical Therapy, 14e
- 2024 Corticosteroid guidelines update (PMID 38240492)
Hoffman sign
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have all the material needed for a thorough answer.
Hoffmann Sign
Definition
The Hoffmann sign is an upper motor neuron (UMN) / pyramidal tract sign in the upper limb, analogous to the Babinski sign in the lower limb. It reflects hyperactivity of the deep tendon reflex arc due to loss of descending corticospinal inhibition.
How to Elicit It
- Hold the patient's middle finger (digit III) in slight extension at the proximal interphalangeal joint, with the hand relaxed.
- Flick (snap) the distal phalanx of the middle finger downward - sharply extending the distal interphalangeal joint and then releasing it.
- Observe the thumb and index finger.
Positive response: Involuntary flexion of the thumb (interphalangeal joint) and/or flexion of the index finger.
- Bailey and Love's Short Practice of Surgery: "forced flexion of the distal phalanx of the middle finger results in flexion of the thumb and index finger"
- Firestein & Kelley's Textbook of Rheumatology: "holding the middle finger extended and suddenly extending the distal interphalangeal joint, resulting in flexion of the index finger and thumb"
Mechanism
The sign works via a stretch reflex of the long flexors of the thumb and index finger (flexor pollicis longus and flexor digitorum profundus). Normally, these reflexes are suppressed by descending corticospinal inhibition. When the corticospinal tract is damaged, this inhibition is lost, and the abrupt stretch of the finger flexor tendons (via the flicking maneuver) triggers an exaggerated reflex response. - Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Clinical Significance
Primary Indication: Corticospinal (UMN) Tract Dysfunction
A positive Hoffmann sign is a pathological reflex indicating pyramidal tract disease. It appears in the list of UMN signs alongside:
-
Spasticity ("clasp-knife" phenomenon)
-
Pathological hyperreflexia
-
Babinski sign (extensor plantar response)
-
Loss of abdominal superficial reflexes
-
Clonus (ankle, patellar)
-
Pseudobulbar palsy
-
Bradley and Daroff's Neurology in Clinical Practice
Most Common Clinical Contexts
| Setting | Notes |
|---|---|
| Cervical spondylotic myelopathy | Most common cause; present alongside finger escape sign, inverted radial reflex, myelopathy hand |
| Cervical disc herniation / stenosis | Compressive myelopathy above C5 level |
| Multiple sclerosis | Demyelinating lesions in cervical cord |
| ALS (motor neuron disease) | Mixed UMN + LMN picture; Hoffmann sign expected in UMN-predominant cases |
| Spinal cord tumors / syringomyelia | Any cord lesion at or above the C5-C6 level |
| Cervical spine instability | Early clinical manifestation, alongside Babinski and hyperreflexia - Campbell's Operative Orthopaedics |
Important Caveats
- Can be bilateral in normal subjects - particularly in anxious or hyperthyroid individuals with generalised brisk reflexes. A bilaterally positive Hoffmann sign alone, in the absence of other UMN signs, may not be pathological. - Kaplan & Sadock's
- A unilateral or asymmetric Hoffmann sign is more strongly indicative of pathology.
- In cervical myelopathy, UMN signs including Hoffmann sign may not always be present in all patients, especially early in the disease course. - Miller's Review of Orthopaedics
- At the level of cord compression (e.g., C5-C6 disc), there may paradoxically be LMN signs (weakness, atrophy, reduced reflexes in the deltoid/biceps), with UMN signs including Hoffmann below that level.
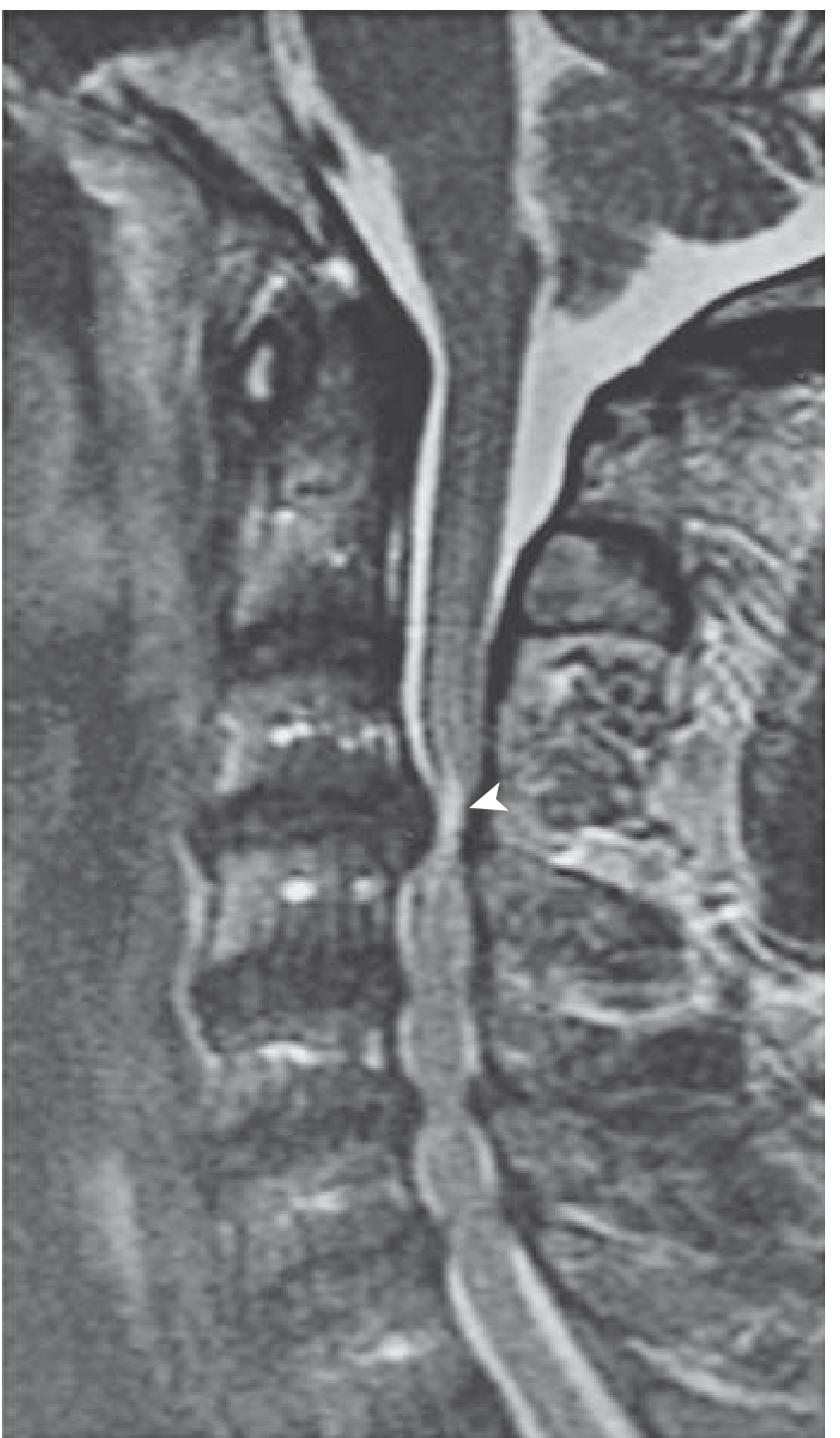
Associated Signs in Cervical Myelopathy
When evaluating for myelopathy, Hoffmann sign is assessed alongside:
| Sign | Description |
|---|---|
| Finger escape sign | Small finger spontaneously abducts/flexes when trying to hold all fingers extended and adducted - weak ulnar intrinsics |
| Grip-release test | Inability to rapidly open and close the fist (>20 cycles in 10 seconds) due to hand spasticity |
| Inverted radial reflex | Eliciting brachioradialis reflex produces finger flexion rather than wrist extension - C5/6 level lesion |
| Lhermitte sign | Electric shock-like sensation down the spine/limbs on neck flexion - white matter change |
| Babinski sign | Extensor plantar response - the lower-limb equivalent |
The underlying pathology in cervical spondylotic myelopathy is illustrated here:
Summary
| Feature | Detail |
|---|---|
| Type | Pathological upper limb reflex (UMN sign) |
| Technique | Snap/flick the distal phalanx of the middle finger downward |
| Positive response | Flexion of thumb + index finger |
| Pathway | Exaggerated stretch reflex of long flexors (loss of corticospinal inhibition) |
| Indicates | Corticospinal tract dysfunction at or above C5-C6 |
| Most common cause | Cervical spondylotic myelopathy |
| Caveat | Bilateral positivity can be a normal variant; unilateral is more significant |
Key references:
- Bradley and Daroff's Neurology in Clinical Practice
- Firestein & Kelley's Textbook of Rheumatology
- Miller's Review of Orthopaedics, 9th Edition
- Bailey and Love's Short Practice of Surgery, 28th Edition
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- Campbell's Operative Orthopaedics, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.