Can u explain me nephrotic nephrotic syndromes pathology in detail, so I can’t forget it and also a digital like with images flowchart, you can say digital something which contains the pneumonic in one page like you know what there should be like image based flow
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Running Command
Writing File
Running Command
Here's everything you need — the full detailed explanation plus your downloadable visual guide:
🫘 Nephrotic Syndrome — Full Pathology Deep Dive
What IS Nephrotic Syndrome?
Nephrotic syndrome is NOT a single disease — it's a clinical syndrome resulting from damage to the glomerular filtration barrier (specifically the podocytes and slit diaphragms), causing massive protein leakage into urine.
🔤 MNEMONIC: "PUFFA" — The 5 Features
| Letter | Feature | Detail |
|---|---|---|
| P | Proteinuria | >3.5 g/day (adults) / >40 mg/m²/hr (children) — MASSIVE, frothy urine |
| U | hypo-Ulbuminemia | <3 g/dL — urinary loss outpaces hepatic synthesis |
| F | Fluid (Oedema) | Periorbital (classic in kids), pedal, ascites — caused by ↓oncotic pressure |
| F | Fat (Lipiduria) | Maltese cross birefringent oval fat bodies in urine under polarized light |
| A | hyper-lipid-Aemia | ↑LDL, ↑VLDL, ↑cholesterol — liver compensates for low oncotic pressure by making more lipoproteins |
⚙️ Central Pathogenesis Flow
Podocyte Injury
↓
Foot Process Effacement (actin cytoskeleton disruption)
↓
Slit Diaphragm Breakdown
↓
GBM Charge + Size Barrier Lost
↓
Massive Proteinuria (>3.5 g/day)
↓
↓ Albumin → ↓ Oncotic Pressure → Oedema
↘ Liver ↑ Lipoprotein synthesis → Hyperlipidaemia + Lipiduria
The podocyte is the key cell — on electron microscopy, foot process effacement (foot processes fused/flattened into the GBM) is the universal hallmark across ALL causes of nephrotic syndrome.
🔬 The 4 Major Causes — Mnemonic: "FIRM"
F = Focal Segmental (FSGS) | I = Idiopathic MCD | R = Ridged GBM (Membranous) | M = Membranoproliferative (MPGN)
🟢 1. Minimal Change Disease (MCD)
"Baby Clean" — Nothing to see, but EM tells the truth
- Most common nephrotic syndrome in children (65% of pediatric cases), peak age 1-7 years
- Pathogenesis: T-cell-derived circulating permeability factor injures podocytes → selective proteinuria (mainly albumin). Strongly associated with Hodgkin lymphoma, NSAIDs, atopy
- LM: COMPLETELY NORMAL (hence "minimal change")
- IF: Negative — no immune deposits
- EM: Diffuse foot process effacement ONLY — no deposits
- Steroid response: Excellent — >90% in children respond to prednisone
- Prognosis: Excellent — may relapse but rarely progresses to ESRD
- Memory: MCD = Maximum Corticosteroid Dependence — steroids fix it. Clean glomerulus = empty canvas.
🔴 2. Focal Segmental Glomerulosclerosis (FSGS)
"Scar on the Map"
- Most common primary nephrotic syndrome in adults, especially Black Americans (APOL1 risk alleles on chromosome 22)
- Focal = only SOME glomeruli involved | Segmental = only PART of each glomerulus scarred
- Pathogenesis:
- Primary FSGS: Circulating factor (cardiotrophin-like cytokine-1 candidate) + podocyte gene mutations (NPHS1, NPHS2/podocin, WT1)
- Secondary FSGS: Adaptive scarring due to nephron loss (obesity, reflux, sickle cell, reduced renal mass)
- Collapsing FSGS: HIV/Parvovirus B19 — podocyte proliferates + tuft collapses → massive proteinuria, worst prognosis
- LM: Focal, segmental areas of sclerosis (collagen deposition) and hyalinosis in some glomeruli
- IF: Non-specific IgM and C3 trapped in scarred areas (not diagnostic)
- EM: Foot process effacement + epithelial denudation (bare GBM)
- Steroid response: Poor — often steroid-resistant
- Key complication: Recurs rapidly post-renal transplant (hours!) — confirms circulating factor
- Memory: "Few Scars, Going South" — progressive, steroid-resistant, FSGS is MCD's evil twin
🟣 3. Membranous Nephropathy (MN)
"Spike Hedgehog"
- Most common primary nephrotic syndrome in white adults (age 40-60), 30% of adult cases
- Subepithelial immune complex disease
- Pathogenesis:
- Anti-PLA2R (M-type phospholipase A2 receptor) IgG4 autoantibodies bind podocyte surface receptor → in-situ immune complex formation → C5b-9 (MAC) complement activation → podocyte injury → proteinuria
- Anti-PLA2R positive in ~70% of idiopathic cases — diagnostic and can monitor disease activity
- Deposits are SUBEPITHELIAL (between podocyte and GBM surface)
- Secondary causes: HBV, SLE, gold/penicillamine, malignancy (lung, colon)
- LM: Diffuse GBM thickening; "spike and dome" on silver stain — GBM matrix grows up between deposits like spikes
- IF: Granular IgG + C3 along GBM — "lumpy bumpy" fluorescence
- EM: Subepithelial electron-dense deposits (EDD) — above the GBM
- Prognosis: "Rule of Thirds" — 1/3 spontaneous remission, 1/3 persistent proteinuria, 1/3 progress to ESRD
- Memory: Hedgehog back = silver stain spikes. PLA2R = "PLease Ask 2 Recall the receptor"
🟠 4. MPGN (Membranoproliferative GN)
"Tram Tracks" — Nephrotic + Nephritic overlap
- Can present as both nephrotic AND nephritic syndrome
- "Membrano" = GBM changes | "Proliferative" = mesangial cell proliferation
- Pathogenesis:
- Type I MPGN: Subendothelial immune complexes (HCV, SBE, cryoglobulinemia) → classical complement activation → mesangial cell proliferates and "interposes" between endothelium and GBM → GBM splits into two layers ("tram-track")
- Type II (Dense Deposit Disease/DDD): C3 Nephritic Factor (C3NeF, an IgG autoAb against C3bBb convertase) → uncontrolled alternative complement pathway activation → ↓↓C3 → intramembranous dense deposits
- LM: Lobular glomeruli; "tram-track" GBM splitting (double contour) on silver/PAS stain; mesangial proliferation
- IF: Type I — granular IgG + C3 + C1q; Type II — C3 ONLY (no immunoglobulin)
- EM: Type I — subendothelial deposits; Type II — dense osmiophilic intramembranous "ribbon" deposits
- Labs: ↓↓ Serum C3 (KEY diagnostic clue — hypocomplementemia)
- Prognosis: Poor — 50% reach ESRD within 10 years
- Memory: TRAM-TRACK = Two Rails Are Mesangial-Mediated. DDD = Dense deposits Deeply embedded.
📍 Deposit Location — The Ultimate Cheat
BLOOD SIDE URINE SIDE
[Endothelium] --- [GBM] --- [Podocyte foot processes]
↑ ↑ ↑
MPGN Type I DDD (intramembranous) MN (subepithelial)
(subendothelial)
MCD = NO deposits | FSGS = NO immune deposits
⛓️ Consequences of Nephrotic Syndrome
| Loss in Urine | Consequence |
|---|---|
| Antithrombin III, Proteins C & S | Hypercoagulability → DVT, renal vein thrombosis (esp. MN!), PE |
| IgG, complement factors | ↑ Infection risk (especially encapsulated organisms — Streptococcus pneumoniae) |
| Vit D-binding protein | Hypocalcaemia → secondary hyperparathyroidism → bone disease |
| Albumin | Oedema, drug toxicity (↓albumin = ↑free drug fraction) |
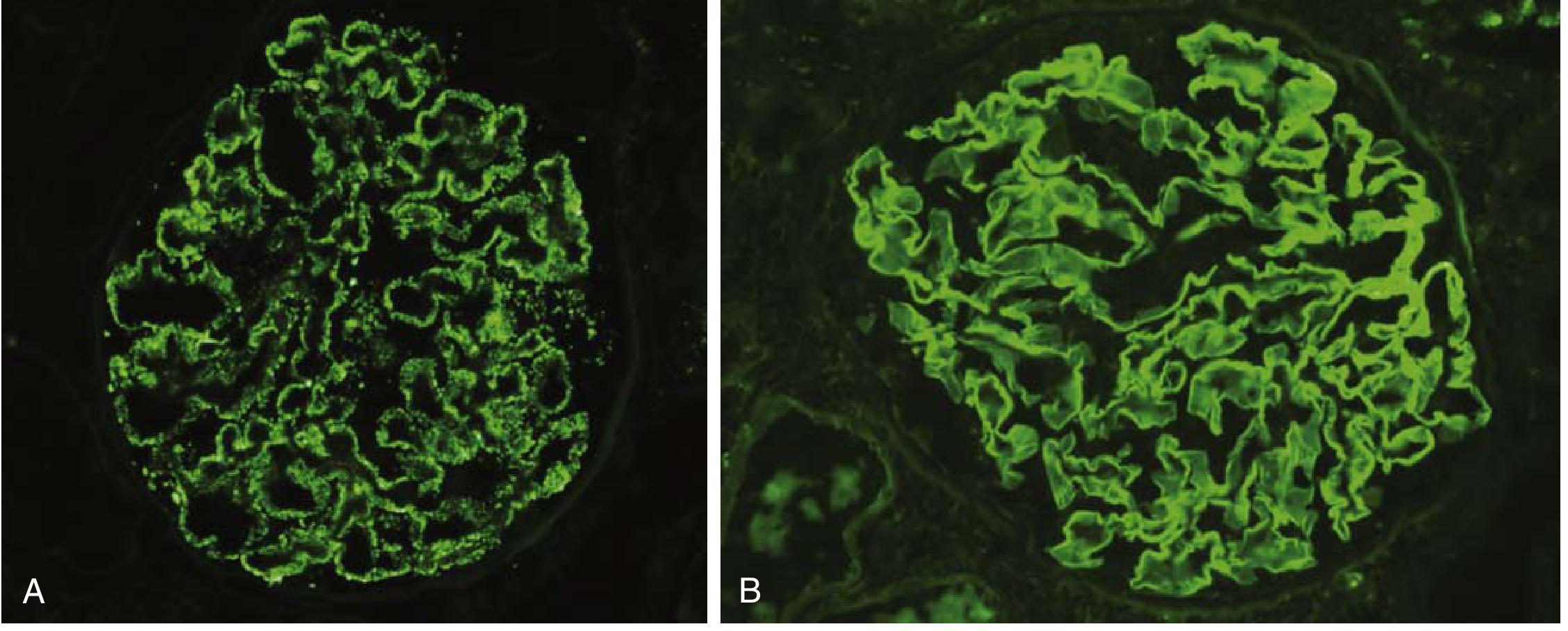
🎯 Textbook Histology Images
This is the immunofluorescence pattern comparison (granular vs. linear) from Robbins Pathology:
🖥️ Your Visual Flowchart/Infographic
A full-page, color-coded, image-rich digital guide with:
- PUFFA mnemonic decoded
- FIRM mnemonic for the 4 causes
- All 4 disease cards with LM/IF/EM findings
- Side-by-side comparison table
- Deposit location diagram
- Downstream consequences
- Memory pegs for each disease
nephrotic syndrome visual
HTML File · HTML
Open in any browser — works offline, dark theme, mobile-responsive.
Sources: Robbins & Kumar Basic Pathology, p. 503-510 | Comprehensive Clinical Nephrology 7th Ed, p. 256-260 | Brenner & Rector's The Kidney
Make a quick reference poster comparing all 4 nephrotic syndromes side-by-side
Generating Image
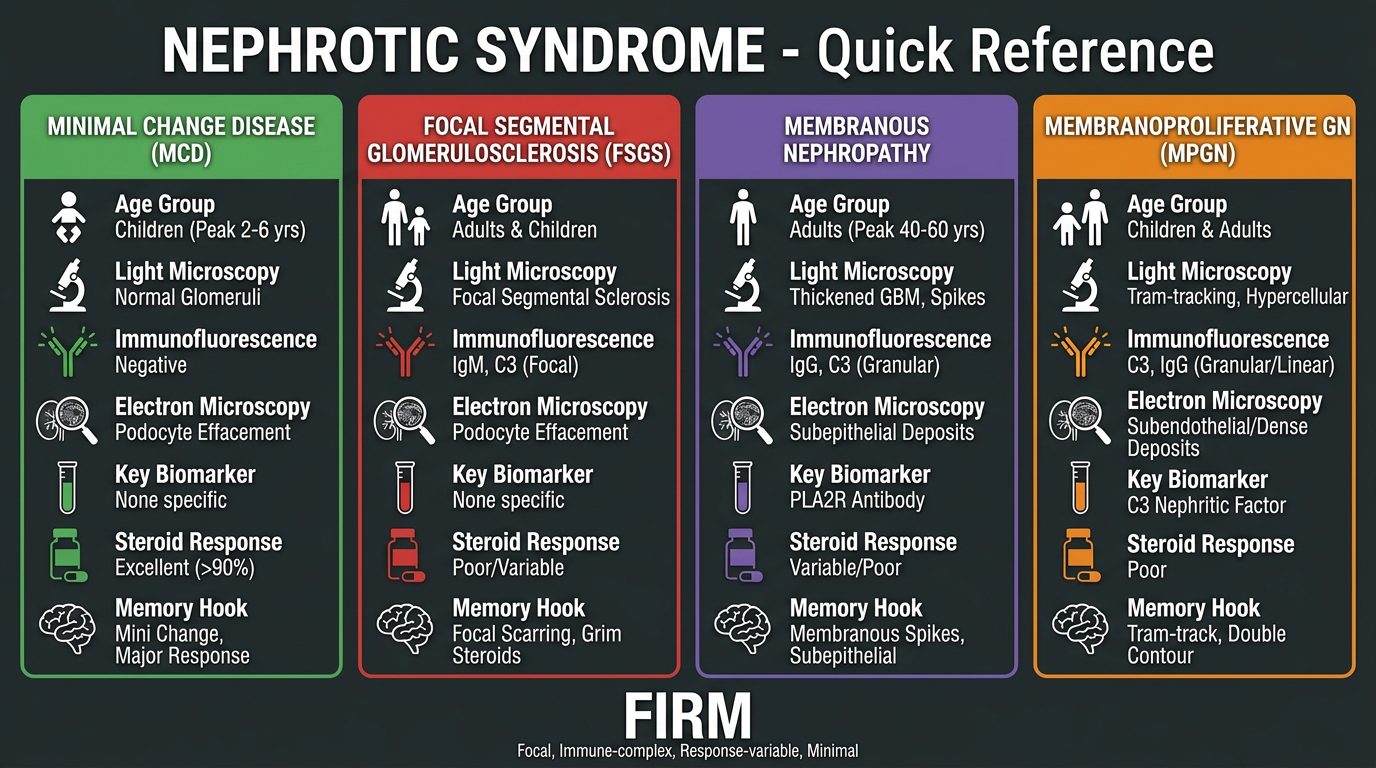
That's your quick reference poster! It's also packed into the visual HTML guide from before if you want the fully interactive version:
nephrotic syndrome visual
HTML File · HTML
Here's a fast cheat at a glance for the 4 columns:
| 🟢 MCD | 🔴 FSGS | 🟣 Membranous | 🟠 MPGN | |
|---|---|---|---|---|
| Age | Kids 1-7 | Adults (Black) | White adults 40-60 | Young adults |
| LM | NORMAL | Focal segmental sclerosis | Spike & dome | Tram-track |
| IF | Negative | IgM/C3 (non-specific) | Granular IgG+C3 GBM | IgG+C3 (Type I) / C3 only (DDD) |
| EM | Effacement only | Effacement + denudation | SUBepithelial deposits | SUBendothelial / intramembranous |
| Key marker | Steroid response | APOL1 / podocin | Anti-PLA2R Ab | ↓C3 / C3NeF |
| Steroids | ✅ Excellent | ❌ Resistant | Variable | ❌ Poor |
| Hook | Baby Clean | Scar on Map | Spike Hedgehog | Tram Tracks |
What’s happed ?
Could you clarify what you mean? Are you asking:
- What happened with the poster/output? — Did something not load or look wrong?
- What happened in nephrotic syndrome? — Like the pathological events/cascade?
- Something else entirely?
Let me know and I'll sort it out!
Generate a PDF version of the nephrotic syndrome quick reference poster
Reading File
Running Command
Running Command
Running Command
PDF generated successfully (604 KB). Here it is:
nephrotic syndrome poster
PDF Document · PDF
The PDF is a full render of the visual guide — dark theme, all 4 disease cards, the PUFFA + FIRM mnemonics, comparison table, deposit location diagram, and memory pegs. Ready to print or share.
This is a shared conversation. Sign in to Orris to start your own chat.