What is mi
"MI" can mean several things depending on context. The most common interpretations are:
- Myocardial Infarction (heart attack) - a medical emergency where blood flow to the heart is blocked
- Michigan - the US state (abbreviation MI)
- Mission Impossible - the film/TV franchise
- Machine Intelligence - sometimes used as a synonym for AI/ML
- Motivational Interviewing - a counseling technique
Could you clarify what you meant? That way I can give you a precise, useful answer.
Explain it
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND "pathophysiology"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a thorough explanation of Myocardial Infarction (MI):
Myocardial Infarction (MI) - Heart Attack
Definition
A myocardial infarction is necrosis (death) of heart muscle resulting from ischemia - an inadequate blood supply to the myocardium. The 2018 joint U.S./European Cardiology task force defines it as "the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia." - Robbins & Kumar Basic Pathology
Causes & Pathogenesis
The vast majority (~90%) of MIs result from acute coronary artery thrombosis, typically triggered by rupture or erosion of an atherosclerotic plaque. The sequence is:
- An atheromatous plaque is disrupted by endothelial injury, intraplaque hemorrhage, or mechanical forces - exposing subendothelial collagen and necrotic plaque contents to blood
- Platelets adhere, aggregate, and release thromboxane A2, ADP, and serotonin - causing further platelet clumping and vasospasm
- Coagulation is activated by exposure of tissue factor, adding to the growing thrombus
- Within minutes, the enlarging thrombus can completely occlude the coronary artery lumen
Less common causes (~10%) include coronary artery vasospasm, embolization from mural thrombi (e.g., in atrial fibrillation), or disorders of small intramyocardial arteries (vasculitis, amyloid deposition, sickle cell disease). - Robbins & Kumar Basic Pathology
What Happens to the Myocardium
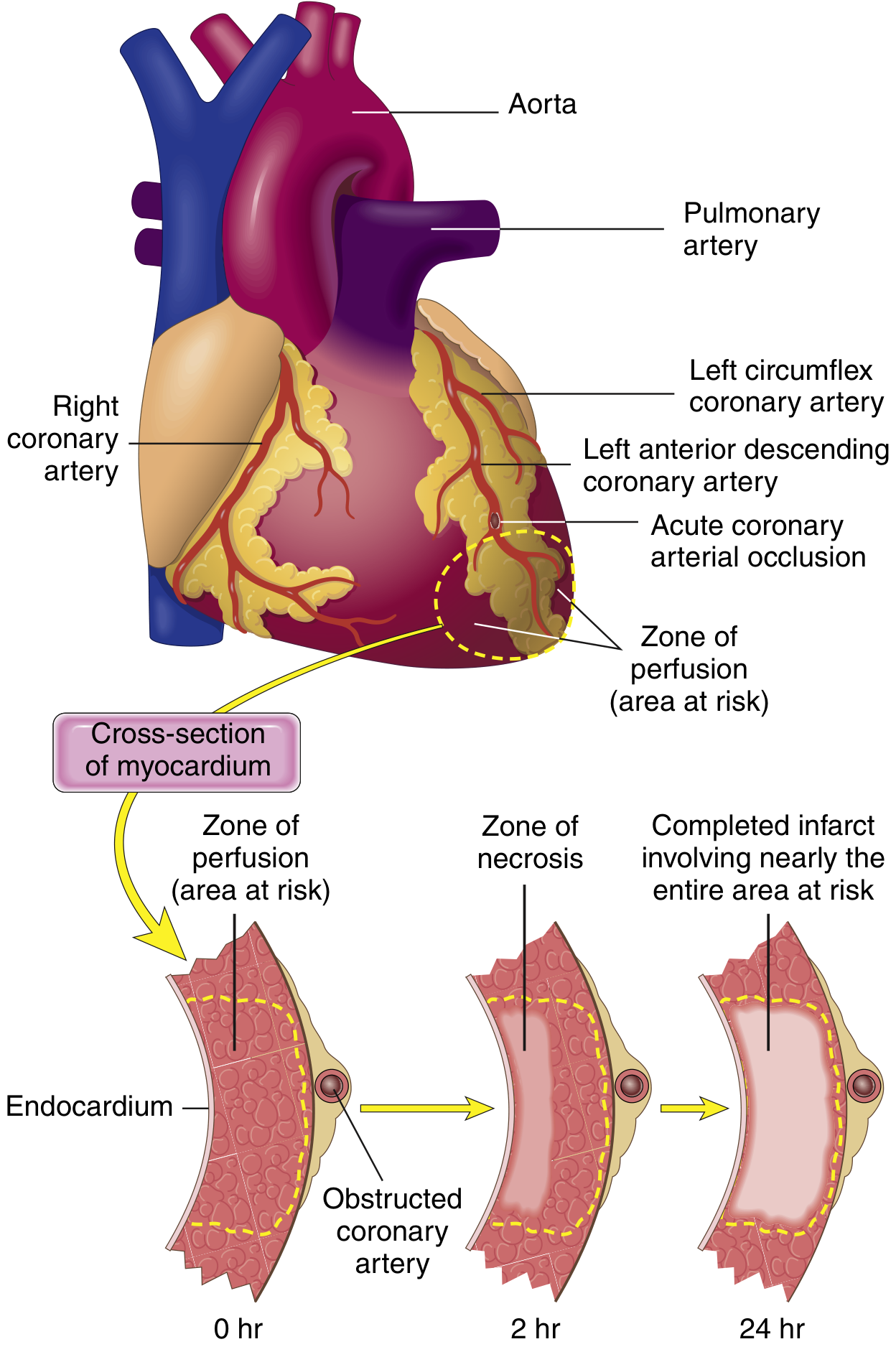
- Immediately: Blood flow ceases beyond the occlusion. The heart muscle requires ~1.3 mL O₂/100g/min just to survive; central infarct zones with near-zero collateral flow quickly die
- Within seconds: Aerobic metabolism ceases, ATP drops, lactic acid accumulates - contractility is lost within minutes
- 20-40 minutes: If ischemia persists, irreversible damage and coagulative necrosis begin. Sarcolemmal membrane disrupts, releasing cardiac enzymes (troponin, CK-MB) into the bloodstream - which is how MI is detected by blood tests
- 3-6 hours: A full transmural (full-thickness) infarct can be established without intervention
- Subendocardial zone: Necrosis always starts here first, since this region is most distal to blood supply and subjected to the highest intramural pressures
Guyton and Hall Textbook of Medical Physiology; Robbins & Kumar Basic Pathology
Which Arteries Are Involved
| Artery Occluded | Area Affected | % of MIs |
|---|---|---|
| Left Anterior Descending (LAD) | Anterior LV wall, anterior 2/3 of septum, heart apex | 40-50% |
| Right Coronary Artery (RCA) | Much of the right ventricle, inferior LV | 30-40% |
| Left Circumflex (LCX) | Lateral left ventricle | 15-20% |
ECG Changes (How MI Is Detected on Electrocardiogram)
Three electrical changes happen in infarcted muscle: rapid repolarization, decreased resting membrane potential, and delayed depolarization. All three produce ST segment elevation in leads overlying the infarct area. Over days to weeks:
- ST elevation subsides
- Q waves may appear (sign of electrically silent dead tissue)
- Leads on the opposite side of the heart show ST depression (reciprocal changes)
Ganong's Review of Medical Physiology
Causes of Death After MI
- Decreased cardiac output - damaged muscle can't pump effectively; the non-infarcted muscle is burdened by "systolic stretch" (it contracts but just pushes against floppy dead tissue)
- Pulmonary edema - backed-up blood in the pulmonary circulation
- Ventricular fibrillation - the most common cause of cardiac death in MI (80-90% of cases); ischemic tissue becomes electrically irritable
- Cardiac rupture - rare but catastrophic
Guyton and Hall Textbook of Medical Physiology
Ischemia-Reperfusion Injury
Even when blood flow is restored (via thrombolysis or angioplasty), restoring circulation can paradoxically worsen damage through:
- Burst of reactive oxygen species (ROS) from recovering but damaged mitochondria
- Calcium influx into injured cells
- Inflammatory cascade from infiltrating leukocytes
This is why "stunned myocardium" (viable but non-contractile heart muscle) can persist for days even after successful reperfusion. - Robbins & Kumar Basic Pathology
Risk Factors
- Atherosclerosis (the underlying driver in most cases)
- Age (risk rises progressively; ~10% of MIs occur before age 40, 45% before age 65)
- Male sex (women are partially protected during reproductive years by estrogen; risk equalizes after menopause)
- Hypertension, diabetes, smoking, high cholesterol, family history
Key Point
The core principle is time is muscle - the earlier intervention (thrombolysis, angioplasty/stenting) restores blood flow, the more heart muscle is saved. An infarct reaches its full size in 3-6 hours, so prompt treatment is critical.
This is a shared conversation. Sign in to Orris to start your own chat.