Introduction to Water and Electrolyte Balance and its Clinical Importance 5 10 Types, Clinical Features, Investigations and Management of 5 Hyponatremia 11 Causes, Clinical Features, Complications and Management of 5 Hypernatremia
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from the textbooks. Let me compile the complete structured answer.
Water and Electrolyte Balance, Hyponatremia, and Hypernatremia
PART 1: Introduction to Water and Electrolyte Balance and Its Clinical Importance
Body Fluid Compartments
Total body water (TBW) in a 70-kg adult male is approximately 42 litres, representing ~60% of body weight. This varies with age, sex, and body composition (females ~50% TBW; neonates 70-75%).
TBW is distributed across two major compartments:
| Compartment | Volume (70-kg male) | % Body Weight |
|---|---|---|
| Intracellular fluid (ICF) | ~28 L | ~40% |
| Extracellular fluid (ECF) | ~14 L | ~20% |
| - Interstitial fluid | 11 L | |
| - Plasma | 3 L | |
| - Transcellular fluid | 1-2 L |
The transcellular compartment includes synovial, peritoneal, pericardial, intraocular fluids, and CSF.
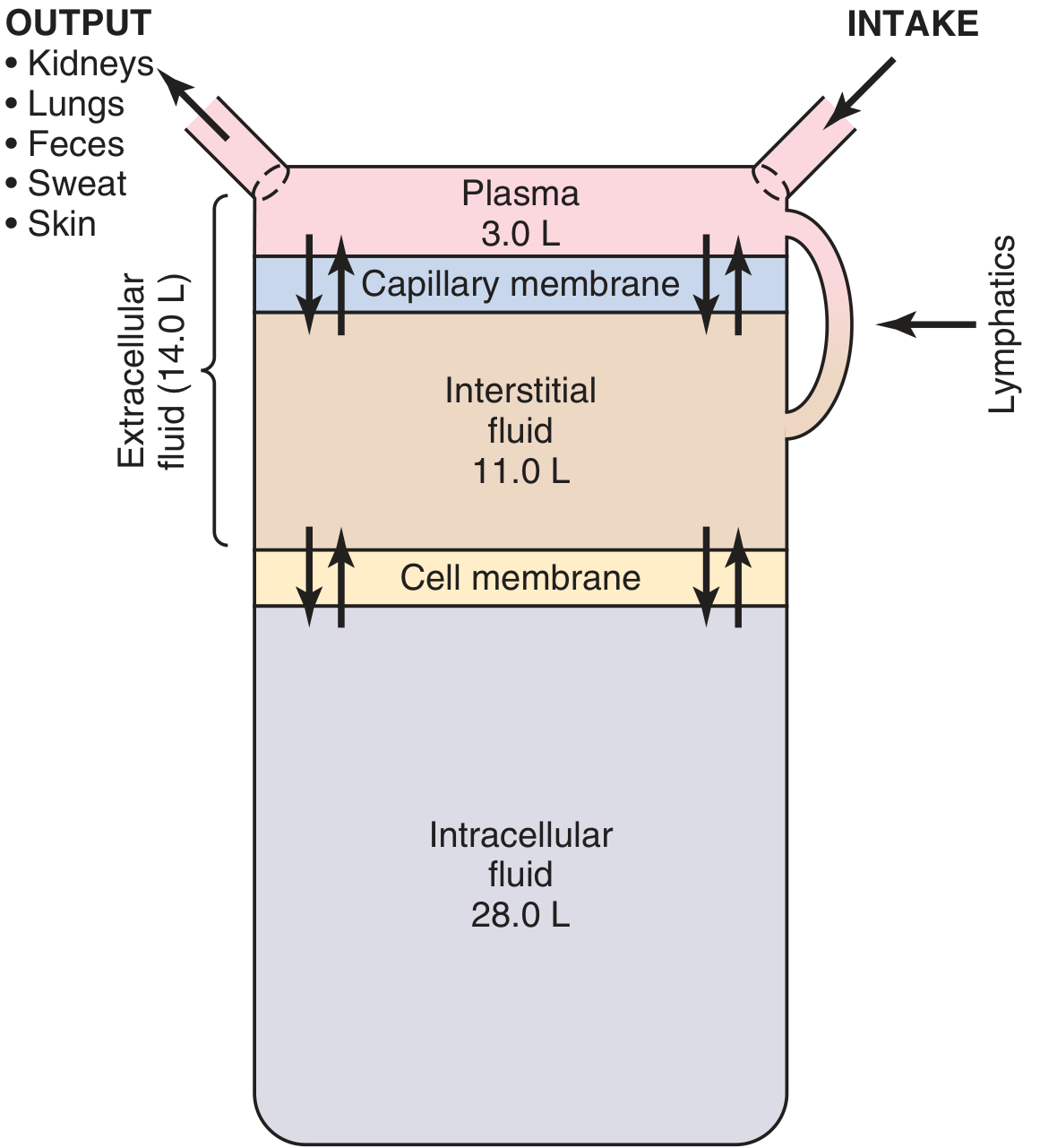
Figure: Body fluid compartments and regulation (Guyton & Hall Textbook of Medical Physiology)
Osmolality and Electrolyte Regulation
- Normal plasma osmolality: 280-295 mOsm/kg
- Sodium (Na+) is the dominant ECF cation and the primary determinant of ECF osmolality
- Potassium (K+) is the dominant ICF cation
- Osmolality is tightly regulated by ADH (vasopressin) from the posterior pituitary and by the thirst mechanism
Role of Hormones in Electrolyte Balance
Aldosterone (mineralocorticoid):
- Acts on distal tubule and collecting ducts
- Enhances Na+ reabsorption, promotes K+ and H+ excretion
- Hyperaldosteronism: Na+ retention, expanded ECF, hypokalemia, alkalosis, hypertension
- Aldosterone deficiency: Na+ wasting, hyponatremia, hyperkalemia, acidosis, hypotension
ADH (Vasopressin):
- Promotes water reabsorption in collecting ducts
- Released in response to increased osmolality (1-2% rise) or significant volume depletion
- Dysfunction leads to diabetes insipidus
Glucocorticoids: Permissive role in free water excretion; glucocorticoid deficiency causes water retention and hyponatremia (via increased ADH secretion).
Clinical Importance
Electrolyte and water disorders are among the most common clinical problems encountered in all specialties. Hyponatremia incidence in hospitalized patients ranges from 15-30%. Electrolyte disturbances cause:
-
Neurological symptoms (altered consciousness, seizures, coma)
-
Cardiovascular instability
-
Acid-base disorders
-
Muscle weakness and paralysis
-
Increased morbidity and mortality
-
Guyton and Hall Textbook of Medical Physiology, p. 310
-
Tietz Textbook of Laboratory Medicine, 7th Edition, p. 1938
-
Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1030
PART 2: Hyponatremia - Types, Clinical Features, Investigations, Management
Definition
Hyponatremia is defined as serum Na+ < 135 mmol/L. It is the most common electrolyte disorder in hospitalized patients (incidence 15-30%).
Classification by Osmolality
| Type | Plasma Osmolality | Mechanism |
|---|---|---|
| Hypoosmotic | Low (<280 mOsm/kg) | Most common; true Na+ deficit or water excess |
| Iso-osmotic (Pseudohyponatremia) | Normal (280-295) | Hyperlipidemia, hyperproteinemia |
| Hyperosmotic | High (>295) | Hyperglycemia, mannitol, uremia |
Classification by Volume Status (Hypoosmotic Hyponatremia)
1. Hypovolemic Hyponatremia
- Decreased ECF + greater relative Na+ loss
- Extrarenal causes (urine Na+ <20 mEq/L): vomiting, diarrhea, sweating, GI suction, burns, third spacing (bowel obstruction, pancreatitis, rhabdomyolysis)
- Renal causes (urine Na+ >20 mEq/L): diuretics (especially thiazides), mineralocorticoid deficiency, RTA, salt-wasting nephropathy, osmotic diuresis
2. Hypervolemic Hyponatremia
- Increased total body Na+ but greater increase in TBW
- Urine Na+ <20 mEq/L: Congestive heart failure, hepatic cirrhosis, nephrotic syndrome
- Urine Na+ >20 mEq/L: Renal failure
- Mechanism: Reduced effective circulating volume stimulates aldosterone and ADH, causing Na+ and water retention, but water excess predominates
3. Euvolemic Hyponatremia
- Increased TBW with near-normal Na+
- Causes: SIADH (most important), psychogenic polydipsia, beer potomania, hypothyroidism, adrenal insufficiency, MDMA use, exercise-associated, postoperative state, water intoxication
Pseudohyponatremia
- Falsely low sodium reading
- Causes: severe hypertriglyceridemia, hyperproteinemia (multiple myeloma, macroglobulinemia)
- Plasma osmolality is normal
- No actual water shifts occur
SIADH (Syndrome of Inappropriate ADH Secretion)
A common cause of euvolemic hyponatremia. ADH is secreted inappropriately, causing excess water retention without edema.
Three major causes:
- Pulmonary: Small cell lung cancer (10-15% of cases), pneumonia, tuberculosis, abscess
- CNS: Meningitis, brain abscess, subdural hematoma, CVA, psychosis
- Drugs: Thiazide diuretics, narcotics, barbiturates, oral hypoglycemics, antineoplastics (cyclophosphamide, cisplatin, vincristine, vinblastine), carbamazepine, scopolamine
Features of SIADH: No edema, no ascites, no heart failure, urine Na+ >20 mEq/L, urine osmolality inappropriately high despite low serum osmolality.
Differential Diagnosis Algorithm
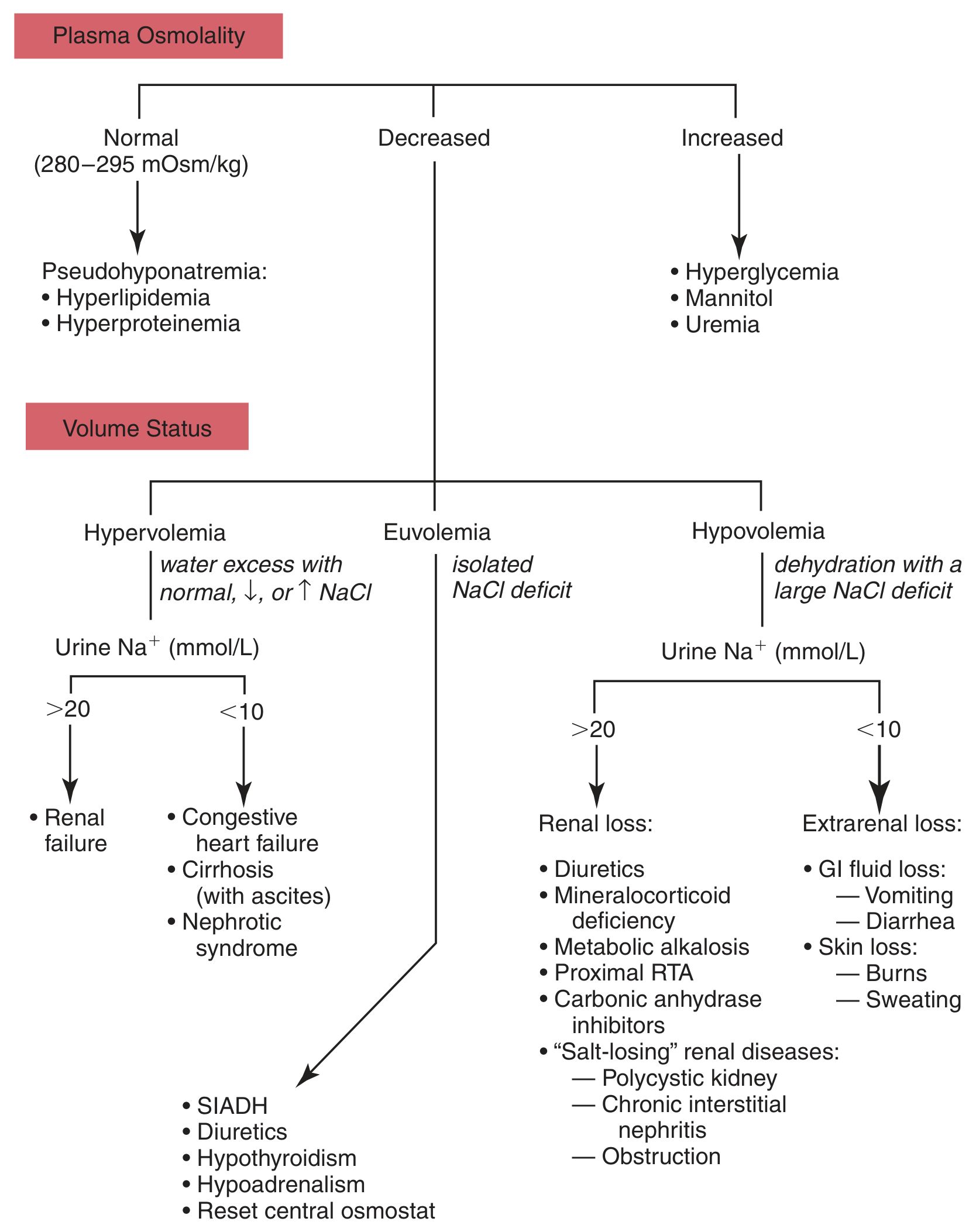
Figure: Differential diagnosis of hyponatremia (Tietz Textbook of Laboratory Medicine, 7th Ed., Fig. 50.3)
Clinical Features
Symptoms correlate with both the degree and rate of fall of serum Na+:
| Severity | Serum Na+ | Symptoms |
|---|---|---|
| Mild | 130-135 mmol/L | Often asymptomatic |
| Moderate | 120-130 mmol/L | Nausea, generalized weakness, malaise, headache |
| Severe | <120 mmol/L | Confusion, lethargy, seizures, coma |
| Critical/Rapid | <120 mmol/L (acute) | Brainstem herniation, respiratory arrest |
- Symptoms due to cerebral edema from water movement into cells (CNS cells swell)
- Symptoms appear at higher Na+ levels (~125 mmol/L) in acute hyponatremia
- Children are at particularly high risk for rapid CNS manifestations
- Geriatric note: Risk doubles in patients presenting with large-bone fractures
Volume-related signs:
- Hypovolemic: Decreased skin turgor, dry mucous membranes, tachycardia, orthostasis
- Hypervolemic: JVD, peripheral edema, pulmonary congestion
- SIADH: No edema, normal skin turgor
Investigations
First-line:
- Serum sodium, serum osmolality
- Urine sodium and osmolality (spot urine)
- Blood glucose, lipids, protein (to exclude pseudohyponatremia)
Interpretation of spot urine Na+:
| Clinical State | Cause | Urine Na+ |
|---|---|---|
| Hypovolemic - nonrenal | GI loss, sweating, burns | <20 mEq/L |
| Hypovolemic - renal | Diuretics, mineralocorticoid deficiency | >20 mEq/L |
| Euvolemic - SIADH | Volume expansion | >20 mEq/L |
| Euvolemic - polydipsia | Dilute urine | <20 mEq/L |
| Hypervolemic - CHF/cirrhosis | Renal hypoperfusion | <20 mEq/L |
| Hypervolemic - renal failure | Renal solute loss | >20 mEq/L |
For SIADH diagnosis: Urine osmolality inappropriately >100 mOsm/kg despite low serum osmolality.
Correction for hyperglycemia: Add 1.6 mEq/L to measured Na+ for every 100 mg/dL glucose above 100 (some guidelines use 2.4 mEq/L for glucose >400 mg/dL above normal).
Management
General Principles
- Correct the underlying cause
- Rate of correction: no more than 6-8 mmol/L per day in chronic hyponatremia (risk of osmotic demyelination syndrome - ODS, formerly central pontine myelinolysis)
- Maximum safe correction rate: 10-12 mmol/L in 24 hours
By Volume Status:
Hypovolemic hyponatremia:
- Restore ECF volume with isotonic (0.9%) saline
- Correct underlying cause (stop diuretics, treat GI losses)
Hypervolemic hyponatremia (CHF, cirrhosis, nephrotic syndrome):
- Fluid restriction (primary treatment)
- Treat underlying disease
- Loop diuretics as needed
- Vasopressin receptor antagonists (vaptans - tolvaptan, conivaptan) in refractory cases
Euvolemic hyponatremia (SIADH):
- Free water restriction (~500 mL less than urine output) - mainstay of therapy
- Treat underlying cause
- Demeclocycline (inhibits ADH action) in chronic SIADH
- Vaptans (tolvaptan) where available
Acute symptomatic hyponatremia (seizures, coma):
- 3% hypertonic saline as small boluses or continuous infusion
- Raise serum Na+ by 4-6 mmol/L - sufficient to resolve severe neurologic symptoms
- Two groups requiring active treatment: (1) Na+ ≤110 mEq/L (severe, even if asymptomatic), (2) acute symptomatic hyponatremia with Na+ <120 mEq/L
Osmotic Demyelination Syndrome (ODS): Risk from over-rapid correction. Patients with malnutrition, alcoholism, liver disease, hypokalemia are at highest risk. Presents with locked-in syndrome, quadriplegia, pseudobulbar palsy.
- ROSEN's Emergency Medicine, p. 2432-2527
- Tietz Textbook of Laboratory Medicine, 7th Edition, p. 1938-1941
- Brenner and Rector's The Kidney, p. 1901-1930
PART 3: Hypernatremia - Causes, Clinical Features, Complications, Management
Definition
Hypernatremia is serum Na+ > 145 mEq/L (mmol/L). It is always hyperosmolar.
It is less common than hyponatremia because even a 1% rise in serum osmolality triggers thirst. Most cases occur in patients who cannot access or sense thirst: elderly, infants, patients with mental impairment, sedated/intubated patients.
Carries a very poor prognosis in critically ill patients - mortality 40-60%, with prolonged ICU stay.
Causes (Three Physiologic Categories)
Type 1: Hypernatremia with Dehydration (Low Total Body Na+ and Low TBW)
- Heatstroke
- Increased insensible losses: burns, excessive sweating
- Gastrointestinal losses: diarrhea, protracted vomiting, continuous GI suction
- Osmotic diuresis: hyperglycemia, mannitol, enteral feeding
Type 2: Hypernatremia with Normal Total Body Na+ (Pure Water Deficit)
Diabetes Insipidus (DI) - most important in this category
-
Central DI (insufficient ADH production):
- Idiopathic, familial
- Head trauma
- CNS tumors (suprasellar/infrasellar)
- Hypoxic encephalopathy
- Infiltrative disorders (sarcoidosis, histiocytosis)
- Anorexia nervosa
- Post-surgical hypophysectomy
-
Nephrogenic DI (renal resistance to ADH):
- Drugs: lithium, demeclocycline, amphotericin, aminoglycosides, propoxyphene, methoxyflurane, phenytoin
- Electrolyte disorders: hypercalcemia, hypokalemia
- Sickle cell anemia, Sjögren syndrome (affect collecting duct responsiveness)
- Chronic renal insufficiency, polycystic kidney disease
- Mutant vasopressin receptors (rare)
-
Elderly with "reset" osmostat
-
Hypothalamic dysfunction
Type 3: Hypernatremia with Increased Total Body Na+ (Na+ Gain in Excess of Water)
- Salt tablet ingestion, saltwater ingestion
- IV hypertonic saline infusions
- IV sodium bicarbonate administration
- Saline enemas
- Poorly diluted infant formula or oral rehydration solutions
- Intentional salt poisoning (soy sauce ingestion in suicide attempts)
- Primary hyperaldosteronism (Conn syndrome)
- Cushing syndrome
- Hemodialysis errors
Differential Diagnosis Algorithm
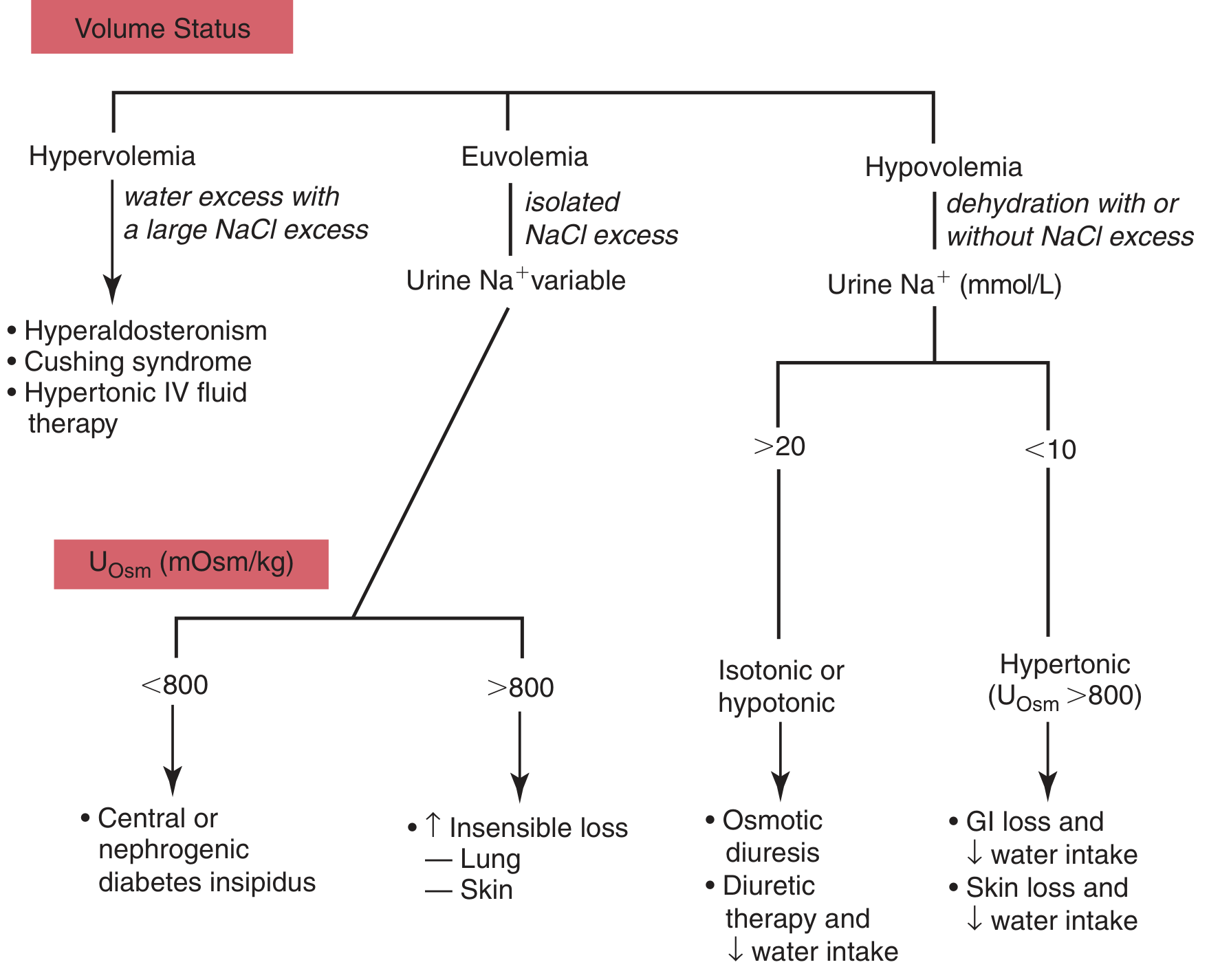
Figure: Differential diagnosis of hypernatremia (Tietz Textbook of Laboratory Medicine, 7th Ed., Fig. 50.4)
Clinical Features
Symptoms are primarily neurological because neurons lose water to the hyperosmolar ECF, causing cell shrinkage:
| Degree | Na+ Level | Symptoms |
|---|---|---|
| Mild | 145-155 mmol/L | Often asymptomatic (if chronic) |
| Moderate | 155-165 mmol/L | Tremors, irritability, restlessness |
| Severe/Acute | >160 mmol/L (acute) | Ataxia, confusion, twitching, muscle rigidity |
| Critical | >175 mmol/L (chronic) | Coma, intracerebral hemorrhage |
- In acute hypernatremia, symptoms may appear at Na+ ~160 mmol/L
- In chronic hypernatremia, symptoms may not appear until Na+ exceeds ~175 mmol/L (CNS cells increase intracellular osmolality to protect against dehydration)
- Polyuria and polydipsia in patients with diabetes insipidus
- Altered mental status is the most common presenting finding
- Patients may be entirely asymptomatic if symptoms are masked by underlying conditions
High-risk groups: elderly, infants, patients with altered mental status, intubated/sedated patients.
Complications
- Cerebral dehydration/shrinkage: Neurons lose water to the hyperosmolar ECF - major cause of neurological symptoms
- Intracerebral hemorrhage: Due to tearing of bridging veins as brain shrinks away from skull (especially in acute, severe cases)
- Cerebral venous thrombosis
- Subarachnoid hemorrhage
- Osmotic demyelination (from overly rapid correction): CNS cells accumulate "idiogenic osmoles" (organic osmolytes) to protect against dehydration. If Na+ is corrected too fast, cells take up excessive water causing cerebral edema - particularly dangerous with chronic hypernatremia
- Rhabdomyolysis (in severe dehydration)
- High mortality: 40-60% in critically ill patients
Investigations
- Serum Na+, serum osmolality (always elevated/hyperosmotic)
- Urine osmolality and urine Na+ (critical for identifying source)
- TBW deficit calculation:
TBW deficit = TBW × (serum Na+ - 140) / 140 Where TBW = body weight (kg) × 0.6 (adjust for age/sex)
- Water deprivation test + vasopressin challenge: To distinguish central from nephrogenic DI
- In central DI: urine osmolality rises with exogenous vasopressin
- In nephrogenic DI: no response to vasopressin
Urine findings by cause:
- Extrarenal loss: Concentrated urine (>800 mOsm/kg), urine Na+ <20 mmol/L
- Central DI: Dilute urine (<250 mOsm/kg), polyuria
- Nephrogenic DI: Dilute urine, no response to ADH
- Hypervolemic causes: Concentrated urine with high urine Na+
Management
Three interdependent goals (ROSEN's Emergency Medicine):
- Rapidly correct underlying shock, hypoperfusion, or significant hypovolemia with normal (0.9%) saline
- Treat the underlying cause (fever, vomiting, diabetes insipidus, etc.)
- Carefully lower serum Na+ by replacing the total water deficit
Rate of Correction - Very Important
- Chronic hypernatremia: Lower Na+ no faster than 0.5 mmol/L/hour (or ~10-12 mmol/L per 24 hours)
- Acute salt poisoning: Rapid correction is safe and may prevent intracranial hemorrhage
- Too-rapid correction of chronic hypernatremia → cerebral edema (cells with accumulated idiogenic osmoles take up excessive water)
Fluid Choices by Type:
| Type | Initial Fluid | Follow-up |
|---|---|---|
| Hypovolemic hypernatremia | Isotonic saline (to restore perfusion) | Then 0.45% saline or 5% dextrose water (D5W) to replace free water |
| Normovolemic (DI) | Oral water rehydration if possible | IV 5% D5W or 0.45% saline |
| Hypervolemic | Loop diuretics (furosemide) + free water | Dialysis if severe renal dysfunction |
Specific Treatments:
- Central DI: Desmopressin (DDAVP) - synthetic ADH analog, intranasal or IV
- Nephrogenic DI: Treat/remove offending drug; thiazide diuretics (paradoxically reduce polyuria); NSAIDs (reduce prostaglandin-mediated inhibition of ADH); correct hypercalcemia or hypokalemia
- Hypervolemic hypernatremia: Loop diuretics + hypotonic fluid; dialysis if needed
- Salt poisoning: Rapid correction with hypotonic fluids is appropriate (unlike chronic hypernatremia)
Summary Comparison Table
| Feature | Hyponatremia | Hypernatremia |
|---|---|---|
| Definition | Na+ < 135 mmol/L | Na+ > 145 mmol/L |
| Osmolality | Low (usually), normal, or high | Always high (hyperosmotic) |
| Pathophysiology | Water excess relative to Na+ | Water deficit relative to Na+ |
| Main CNS mechanism | Cerebral edema (water into cells) | Cerebral dehydration (water out of cells) |
| High-risk groups | Hospitalized, SIADH, diuretic users | Elderly, infants, ICU/intubated patients |
| Key investigation | Serum + urine osmolality, urine Na+ | Serum + urine osmolality, water deprivation test |
| Correction rate | ≤10-12 mmol/L/24 hr | ≤0.5 mmol/L/hr (chronic) |
| Rapid correction risk | Osmotic demyelination (ODS) | Cerebral edema |
| Emergency treatment | 3% hypertonic saline | Normal saline (if hypovol.) then free water |
Key sources:
- ROSEN's Emergency Medicine Concepts and Clinical Practice
- Tietz Textbook of Laboratory Medicine, 7th Edition, pp. 1938-1941
- Brenner and Rector's The Kidney, 2-Volume Set
- Guyton and Hall Textbook of Medical Physiology
- Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.