What is that thing required in follicular and papillary carcinoma to differentiate them
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Here is a complete, textbook-based answer:
Differentiating Follicular vs. Papillary Thyroid Carcinoma
The question is really asking two related things:
1. What differentiates Follicular Carcinoma from Follicular Adenoma (i.e., proves it IS carcinoma)?
Capsular and/or vascular invasion - seen only on histology.
FNAC (fine needle aspiration cytology) cannot make this distinction. As Bailey & Love states directly:
"FNAC cannot distinguish between a benign follicular adenoma and follicular carcinoma, as this distinction is dependent not on cytology but on histological criteria, which include capsular and vascular invasion."
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Two forms are recognized:
| Type | Feature |
|---|---|
| Minimally invasive FTC (MIFC) | Microscopic transcapsular invasion ± pericapsular vascular infiltration |
| Widely invasive FTC (WIFC) | Gross infiltrative/destructive growth into surrounding gland |
FTC spreads via haematogenous routes (bone, lung) - NOT lymphatics.
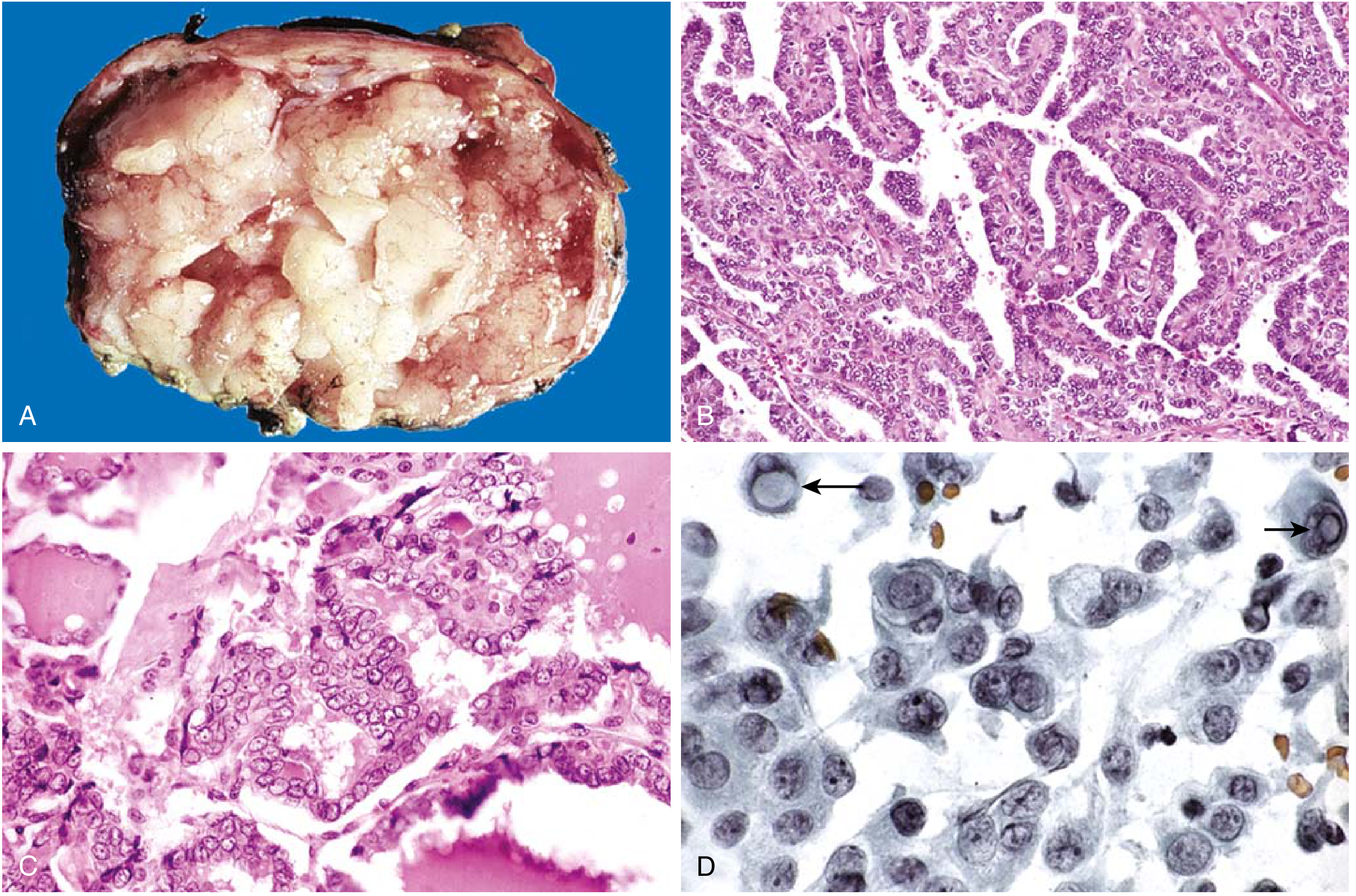
2. What differentiates Papillary Thyroid Carcinoma (PTC) from other lesions?
Nuclear features - these are pathognomonic and can be seen on FNAC.
The classic nuclear hallmarks (from Robbins Basic Pathology):
- Ground-glass / Orphan Annie eye nuclei - finely dispersed chromatin giving an optically clear/empty appearance
- Intranuclear pseudo-inclusions - cytoplasmic invaginations appearing as inclusions inside the nucleus
- Intranuclear grooves
- Psammoma bodies - concentric calcified structures within papillae (almost never in follicular or medullary carcinoma)
"These nuclear features are sufficient for the diagnosis of papillary thyroid carcinoma, even in the absence of papillary architecture."
- Robbins & Kumar Basic Pathology
This is why the follicular variant of PTC is still called PTC - it has follicular architecture but carries all the nuclear features above.
Key Summary Table
| Feature | Papillary Carcinoma (PTC) | Follicular Carcinoma (FTC) |
|---|---|---|
| Diagnosis requires | Nuclear features (FNAC sufficient) | Capsular/vascular invasion (histology mandatory) |
| FNAC role | Diagnostic | Cannot confirm malignancy |
| Spread | Lymphatic (cervical nodes) | Haematogenous (bone, lung) |
| Architecture | Papillary (or follicular variant) | Follicular |
| Psammoma bodies | Yes | No |
| Mutations | BRAF, RET/PTC | RAS, PAX8-PPARG |
The NIFTP Concept (important nuance)
"Noninvasive Follicular Thyroid Neoplasm with Papillary-like Nuclear Features" (NIFTP) is a reclassification for encapsulated, non-invasive follicular-variant PTC. These are low-risk and do not require aggressive treatment - but the key word is non-invasive. The moment invasion (capsular or vascular) is present, it becomes "invasive encapsulated follicular variant of PTC" and is managed as carcinoma.
- Robbins, Cotran & Kumar Pathologic Basis of Disease; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1
This is a shared conversation. Sign in to Orris to start your own chat.