Lab diagnosis of Myocardial infarction from Robbins
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Let me compile the full response.
Lab Diagnosis of Myocardial Infarction
(From Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease)
Overview
MI is diagnosed by a triad of:
- Clinical symptoms
- ECG changes
- Laboratory tests - measuring blood levels of myocardial proteins that leak out of irreversibly damaged myocytes
As stated in Robbins Basic Pathology: "The laboratory evaluation of MI is based on measuring blood levels of normally intracellular proteins that leak out of injured myocardial cells through damaged cell membranes."
Cardiac Biomarkers
When myocytes are irreversibly injured, their plasma membranes become leaky, releasing intracellular proteins into the circulation. The key biomarkers are:
| Biomarker | Rises | Peaks | Returns to Normal |
|---|---|---|---|
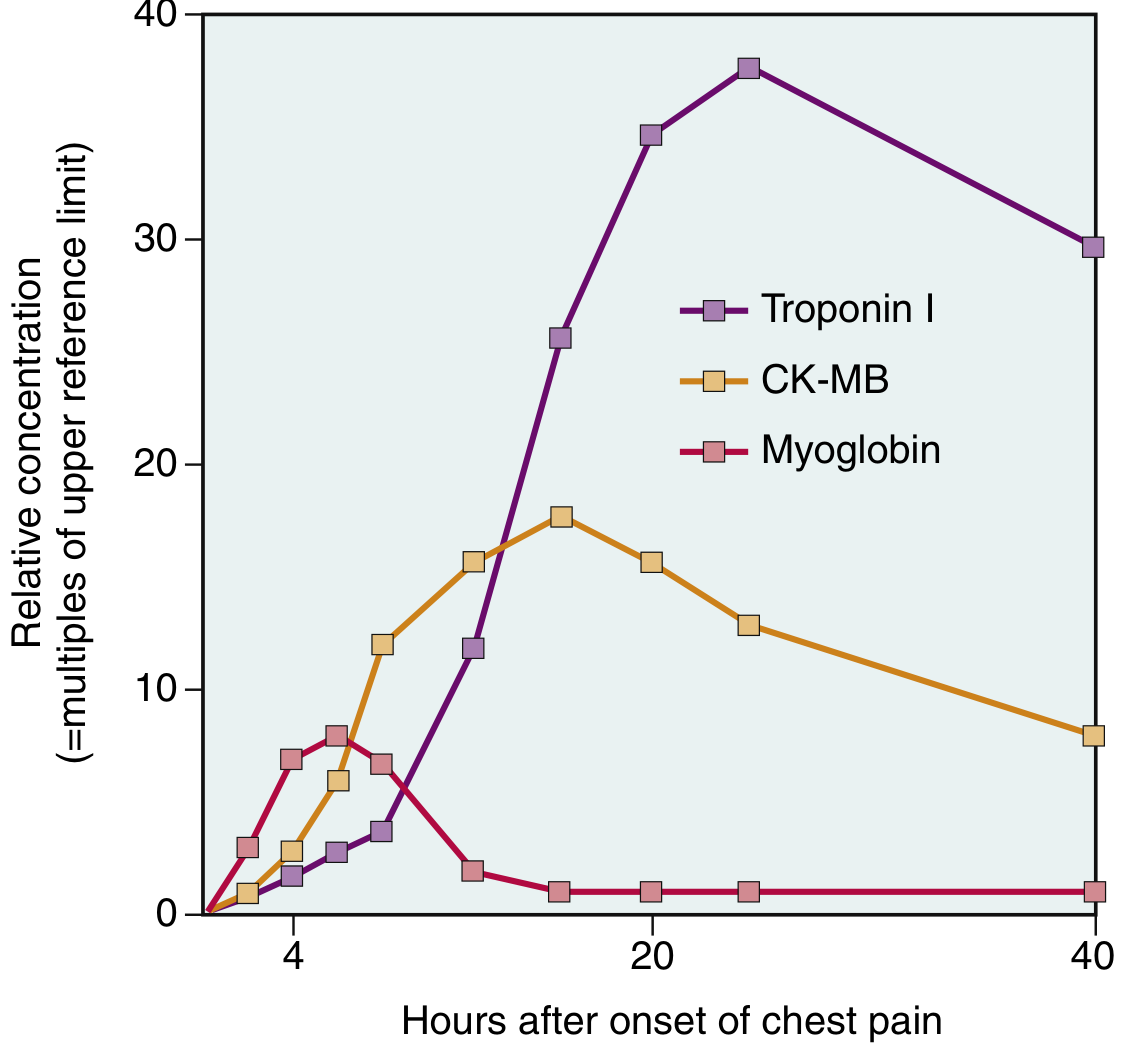
| Troponin I / T | 2-4 hours | 24-48 hours | 7-10 days |
| CK-MB | 2-4 hours | 24-48 hours | ~72 hours (3 days) |
| Myoglobin | Very early (1-4 hours) | ~6 hours | ~24 hours |
1. Cardiac Troponins T and I (cTnT, cTnI) - Gold Standard
- Troponin T and Troponin I are cardiac-specific proteins that normally regulate calcium-mediated contraction of cardiac muscle.
- They are normally not found in the circulation.
- After acute MI, both are detectable within 2 to 4 hours, peak at 48 hours, and remain elevated for 7 to 10 days.
- The prolonged elevation (unlike CK-MB) allows diagnosis of an acute MI long after CK-MB levels have returned to normal.
- The diagnosis of myocardial injury is established when blood levels of troponin rise above threshold (upper reference limit/URL).
How troponin leaks out (Fig. 12.16, Robbins Pathologic Basis of Disease):
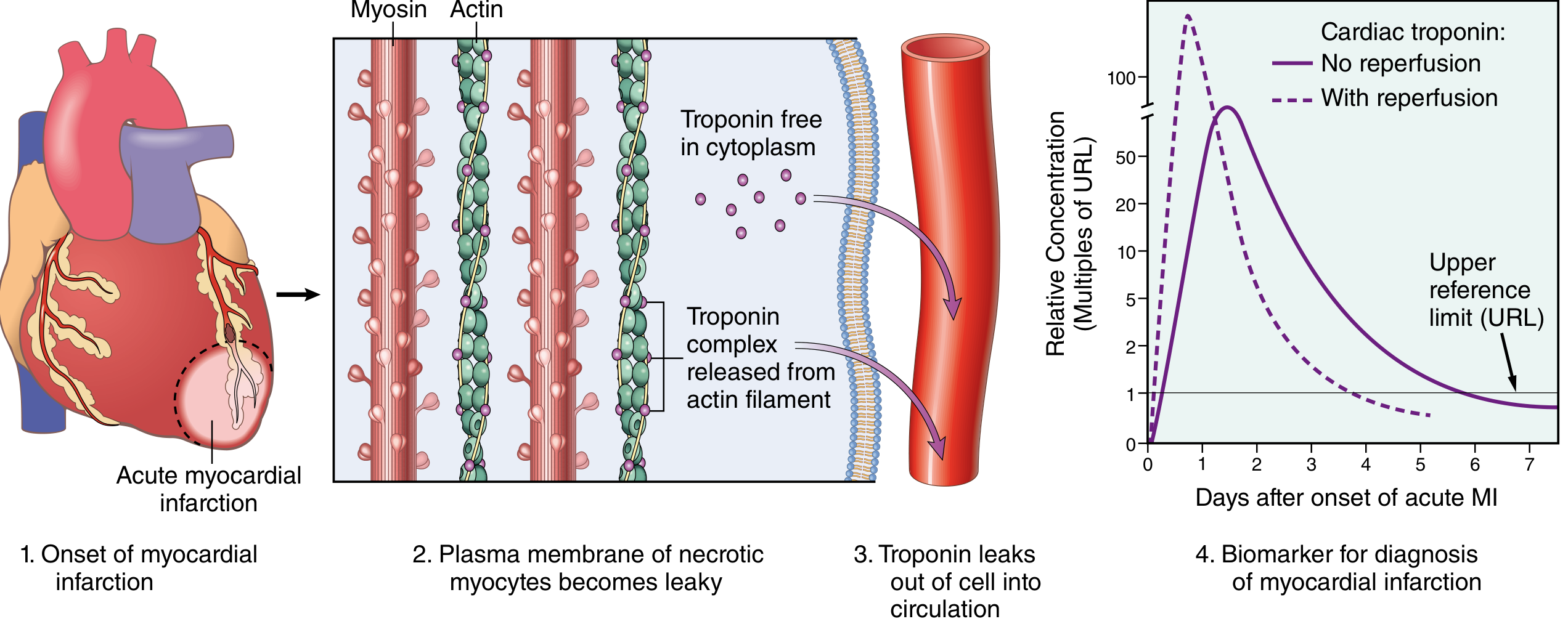
Effect of reperfusion on troponin kinetics:
- With reperfusion, both troponin and CK-MB levels may peak earlier and higher due to more rapid washout of the marker from necrotic tissue (the dashed line in the figure above).
Causes of troponin elevation other than MI:
- High-level elevation (follows MI time course): myocarditis, myocardial trauma
- Low-level "troponin leak" (does NOT follow MI time course): CHF, pulmonary embolism, renal failure, sepsis
- Serial measurements help distinguish MI from these other etiologies.
2. CK-MB (Creatine Kinase - Myocardial Isoform)
- CK-MB has historically been the biomarker of choice but is now tested less frequently in favor of the more sensitive cardiac-specific troponins.
- Activity rises within 2 to 4 hours of MI, peaks at 24 to 48 hours, and returns to normal within approximately 72 hours.
- Shorter window compared to troponins - useful for detecting reinfarction (a new rise after return to normal).
3. Myoglobin
- Detectable very early but substantially less sensitive and specific for myocardial injury.
- Rises first (within 1-4 hours), peaks around 6 hours, normalizes by ~24 hours.
- Not used as a primary diagnostic biomarker due to low specificity (also released from skeletal muscle).
Kinetics Graph (Robbins Basic Pathology, Fig. 9.13)
ECG Diagnosis (complementary)
- ECG changes include Q waves, ST segment changes, and T wave inversions.
- STEMI (ST-elevation MI): complete coronary occlusion, transmural infarct - requires urgent reperfusion (thrombolysis or PCI).
- NSTEMI (non-ST-elevation MI): no complete occlusion, not full-thickness - can often be managed more conservatively.
- Some MIs (especially small or microscopic) may be electrocardiographically silent.
Key Points Summary
| Feature | Detail |
|---|---|
| Best biomarker | Cardiac Troponin I or T |
| Earliest rise | Myoglobin (1-4 hrs), then Troponin/CK-MB (2-4 hrs) |
| Longest window for diagnosis | Troponin (7-10 days) |
| Useful for reinfarction | CK-MB (returns to normal at 72 hrs) |
| Reperfusion effect | Earlier, higher peak ("washout effect") |
| Troponin specificity | High - but low-level leak seen in non-MI conditions |
Sources:
- Robbins & Kumar Basic Pathology, Ch. 9, Clinical Features of MI (pp. 356-359) - Robbins & Kumar Basic Pathology (9780323790185)
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Ch. 12, Clinical Features of MI (pp. 516-517) - Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
This is a shared conversation. Sign in to Orris to start your own chat.