How to depotash a patient
Reading File
Finding Sources
Searching PubMed
hyperkalemia management treatment
Reading File
Reading File
Reading File
Loading Image
Here is a complete, evidence-based guide to "depotashing" (lowering potassium in) a patient with hyperkalemia. Treatment is organized into three sequential stages.
How to Depotash a Patient (Treating Hyperkalemia)
Hyperkalemia = serum K+ ≥ 5.5 mmol/L. K+ ≥ 6.0 mmol/L OR any ECG changes = medical emergency.
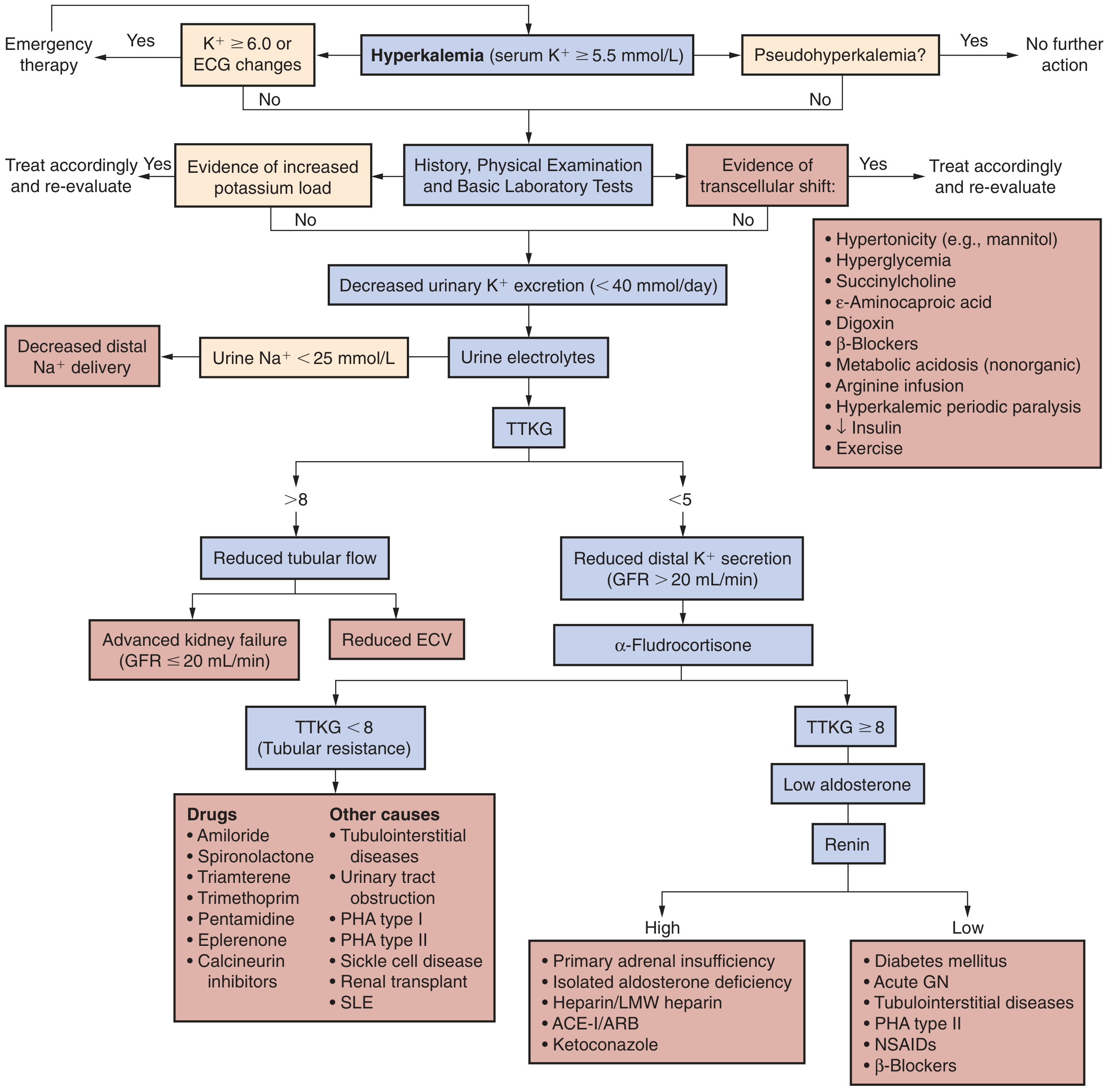
Step 0 - First, Rule Out Pseudohyperkalemia & Start Monitoring
- Check for pseudohyperkalemia (haemolysed sample, extreme thrombocytosis/leukocytosis) - repeat the test
- Admit, start continuous cardiac monitoring and 12-lead ECG
- Restrict dietary K+ (typically 60 mEq/day)
- Review and stop/adjust offending medications (ACE inhibitors, ARBs, K+-sparing diuretics, NSAIDs, heparin, TMP-SMX)
Stage 1 - Cardiac Membrane Stabilization (Immediate)
Goal: Protect the heart NOW - does NOT lower K+
| Agent | Dose | Onset | Duration | Notes |
|---|---|---|---|---|
| Calcium gluconate 10% | 10 mL IV over 2-3 min | 1-3 min | 30-60 min | Preferred - safe via peripheral line; repeat if ECG changes persist or recur |
| Calcium chloride 10% | 3-4 mL IV | 1-3 min | 30-60 min | More elemental Ca2+; requires central line (tissue necrosis if it extravasates) |
Digoxin caution: If the patient is on digoxin, hypercalcemia worsens digoxin toxicity. Instead, dilute 10 mL of 10% calcium gluconate in 100 mL D5W and infuse over 20-30 min to avoid acute hypercalcemia.
Stage 2 - Redistribute K+ Into Cells (Rapid, 10-90 min)
A. Insulin + Glucose (First-line)
- Insulin: 10 units regular insulin IV
- Glucose: 50 mL of 50% dextrose (D50W, 25g) immediately after
- Onset: 10-20 min | Peak: 30-60 min | Duration: 4-6 h
- Follow with 10% dextrose infusion at 50-75 mL/h to prevent hypoglycemia (monitor glucose closely)
- If glucose is already ≥ 200-250 mg/dL: give insulin alone (no glucose), with close glucose monitoring
B. Nebulized Albuterol (Additive to Insulin)
- Dose: 10-20 mg nebulized in 4 mL normal saline over 10 min
- Onset: ~30 min | Peak: ~90 min | Duration: 2-6 h
- Albuterol + insulin have an additive effect
- Caution: ~20% of ESRD patients are resistant; should never be used alone without insulin
- Side effects: tachycardia, hyperglycemia - use with caution in known cardiac disease
C. Sodium Bicarbonate (Limited role)
- No role in acute treatment for immediate effect
- May slowly attenuate K+ over 4-6 h in metabolic acidosis patients
- Give as isotonic infusion (150 mEq NaHCO3 in 1 L D5W) - do NOT give repeated hypertonic boluses (risk of hypernatremia)
Stage 3 - Remove K+ From the Body (Definitive)
A. Diuretics
- Loop diuretics (furosemide) or thiazides: useful if patient has adequate renal function and is volume-replete or hypervolemic
- May combine with IV saline or isotonic bicarbonate to maintain euvolemia
- IV saline alone: useful in hypovolemic patients with oliguria and reduced distal Na+ delivery
B. Gastrointestinal Cation Exchangers (Potassium Binders)
| Agent | Mechanism | Dose | Notes |
|---|---|---|---|
| Patiromer (Veltassa) | Binds K+, releases Ca2+ | Powder suspension | Preferred over SPS - no intestinal toxicity; watch for hypomagnesemia |
| Sodium zirconium cyclosilicate (SZC/Lokelma) | Exchanges Na+/H+ for K+/NH4+ | Powder suspension | Preferred over SPS; fast-acting for a binder |
| Sodium polystyrene sulfonate (SPS/Kayexalate) | Exchanges Na+ for K+ in GI tract | 15-30 g powder in 33% sorbitol suspension | Last resort - full effect takes up to 24 h; rare but often fatal intestinal necrosis, especially in post-op patients or opioid users |
Patiromer and SZC are preferred over SPS whenever available, per Harrison's 22nd ed and recent systematic review evidence (PMID: 40542996).
C. Dialysis (Most Effective)
- Hemodialysis: most effective and fastest definitive K+ removal - use when K+ is life-threatening and medical therapy is insufficient or for AKI/ESRD patients
- Peritoneal dialysis: considerably less effective than hemodialysis
- Amount removed depends on: dialyzer type/surface area, blood/dialysate flow rates, duration, and plasma-to-dialysate K+ gradient
Quick Summary Table
| Stage | Goal | Agent(s) | Onset |
|---|---|---|---|
| 1 - Membrane stabilization | Protect heart | IV Calcium | 1-3 min |
| 2 - Shift K+ into cells | Lower serum K+ temporarily | Insulin + Glucose, Albuterol, NaHCO3 | 10-90 min |
| 3 - Remove K+ from body | Permanently lower K+ | Diuretics, K+ binders (patiromer/SZC), Dialysis | Hours |
Special Situations
- Digoxin toxicity causing hyperkalemia: treat with anti-digoxin Fab (DigiFab) first; avoid calcium if possible
- Hyperkalemia from metabolic acidosis: bicarbonate infusion over hours can help
- ESRD patient: hemodialysis is often the primary definitive treatment
- Post-op/opioid patients: avoid SPS (high risk of intestinal necrosis)
Sources: Harrison's Principles of Internal Medicine 22e, p. 404; Brenner & Rector's The Kidney, p. 774; National Kidney Foundation Primer on Kidney Diseases 8e
This is a shared conversation. Sign in to Orris to start your own chat.