Drowsy
Reading File
Asking for Preferences
Searching the Web
drowsy driving safety statistics risks prevention 2024 2025
Searching PubMed
drowsy driving crash risk sleepiness
Reading Web Page
drowsy driving risks statistics warning signs prevention tips
Drowsy Driving
The Scale of the Problem
Drowsy driving is a serious and underreported road safety issue. According to NHTSA's 2024 data, 644 people died in drowsy-driving-related crashes in 2024 - but this is widely considered a significant undercount because drowsiness is difficult to detect post-crash. Estimates from AAA and the CDC suggest the true number may be 6,400+ deaths annually.
- 93% of drivers say drowsy driving is "very or extremely dangerous"
- Yet 19% of drivers admit to having driven drowsy in the past 30 days (AAA Foundation, 2024 Traffic Safety Culture Index)
- Young adults (ages 19-24) report the highest rates of drowsy driving behavior
Why It's So Dangerous
Drowsiness impairs judgment, reaction time, and attention in ways similar to alcohol. Being awake for 18 hours produces impairment equivalent to a BAC of 0.05%; 24 hours awake equals a BAC of ~0.10% - above the legal limit.
Three crash patterns are most common:
- Occur between midnight - 6 a.m. or late afternoon (circadian dips)
- Single driver, no passengers, running off road at high speed with no braking evidence
- Happen on rural roads and highways
Warning Signs You're Too Drowsy to Drive
- Frequent yawning or blinking
- Difficulty keeping eyes open or focused
- Head drooping or "nodding off"
- Missing exits or traffic signs
- Drifting out of your lane or hitting rumble strips
- Can't remember the last few miles driven
If any of these appear - pull over. There is no safe way to "push through" severe drowsiness while driving.
Prevention Tips (from NHTSA)
| Strategy | Details |
|---|---|
| Get enough sleep | 7-8 hours per night is the only true protection |
| Plan trips carefully | Avoid driving during midnight-6 a.m. and late afternoon if possible |
| Avoid alcohol | Even small amounts amplify sleepiness significantly |
| Check medications | Many antihistamines, sleep aids, and some antidepressants cause drowsiness - check labels |
| Take breaks | On long trips, stop every 2 hours or every 100 miles |
| Caffeine - short-term only | A cup of coffee can provide ~30 minutes of alertness, but is not a substitute for sleep |
| Travel with a companion | A passenger can watch for warning signs and take over driving |
High-Risk Groups
- Teen and young adult drivers - sleep-deprived and less experienced at recognizing impairment
- Shift workers - especially night-shift or rotating-shift employees
- Commercial truck drivers - long hours, monotonous roads
- People with untreated sleep disorders - obstructive sleep apnea significantly elevates crash risk (systematic review, PMID 17557495)
- People taking sedating medications
The Myth of "Pushing Through"
Rolling down the window, turning up the radio, or splashing water on your face do not reliably combat drowsiness. The only real solutions are pulling over and taking a short nap (20 minutes), switching drivers, or stopping for the night.
The National Sleep Foundation runs Drowsy Driving Prevention Week every November with resources and educational materials.
Pneumonitis
Finding Sources
Searching the Web
pneumonitis types causes diagnosis management 2024 2025
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of pneumonitis drawn from multiple major textbooks:
Pneumonitis
Pneumonitis is a broad term for non-infectious inflammation of lung parenchyma, particularly the alveolar walls and interstitium. It is distinct from pneumonia in that it is not caused by active microbial infection, though infection must always be excluded. The most clinically important forms are hypersensitivity pneumonitis (HP), drug-induced pneumonitis, and radiation pneumonitis.
Types and Causes
| Type | Common Triggers |
|---|---|
| Hypersensitivity pneumonitis (HP) | Inhaled organic antigens (bacteria, fungi, animal proteins, chemicals) |
| Drug-induced | Bleomycin, methotrexate, checkpoint inhibitors, EGFR inhibitors, amiodarone |
| Radiation pneumonitis | Thoracic radiotherapy |
| Aspiration pneumonitis | Gastric acid inhalation |
| Lupus/connective tissue | SLE, rheumatoid arthritis, systemic sclerosis |
| Lymphocytic interstitial | HIV infection, Sjogren's syndrome |
Hypersensitivity Pneumonitis (HP)
Definition and Mechanism
HP is a complex inflammatory and/or fibrotic interstitial lung disease (ILD) seen in susceptible individuals due to an immunologically mediated reaction to inhaled antigens. It is also known as extrinsic allergic alveolitis. The pathologic changes primarily involve the alveolar walls - distinguishing it from asthma.
Evidence for immune-mediated pathogenesis includes:
- Elevated proinflammatory chemokines (MIP-1α/CCL3, IL-8) in bronchoalveolar lavage (BAL)
- Increased CD4+ and CD8+ T lymphocytes in BAL
- Specific serum antibodies against causative antigens
- Non-necrotizing granulomas in ~two-thirds of cases (suggesting Type IV/T cell-mediated hypersensitivity)
- Complement and immunoglobulins in vessel walls on immunofluorescence
(Robbins, Cotran & Kumar Pathologic Basis of Disease)
Common Named Syndromes
More than 200 exposure sources have been identified. Classic examples include:
- Farmer's lung - thermophilic actinomycetes from moldy hay
- Pigeon breeder's lung (bird fancier's disease) - proteins from serum, excreta, or feathers
- Humidifier/air-conditioner lung - thermophilic bacteria in heated water
- Hot tub lung - Mycobacterium species from contaminated hot tubs
- Cheese washer's lung - mold exposure
In up to 50% of chronic HP patients at tertiary centers, no causative antigen can be identified despite exhaustive evaluation.
Classification: Nonfibrotic vs. Fibrotic
Modern classification (replacing the older acute/subacute/chronic model) divides HP into two groups based on prognosis:
- Nonfibrotic HP (acute) - lymphocytic alveolitis, neutrophilic infiltration, typically reversible with antigen removal
- Fibrotic HP (chronic) - UIP or NSIP patterns, honeycombing, fibroblastic foci, bronchiolocentric fibrosis; associated with higher mortality
(Murray & Nadel's Textbook of Respiratory Medicine)
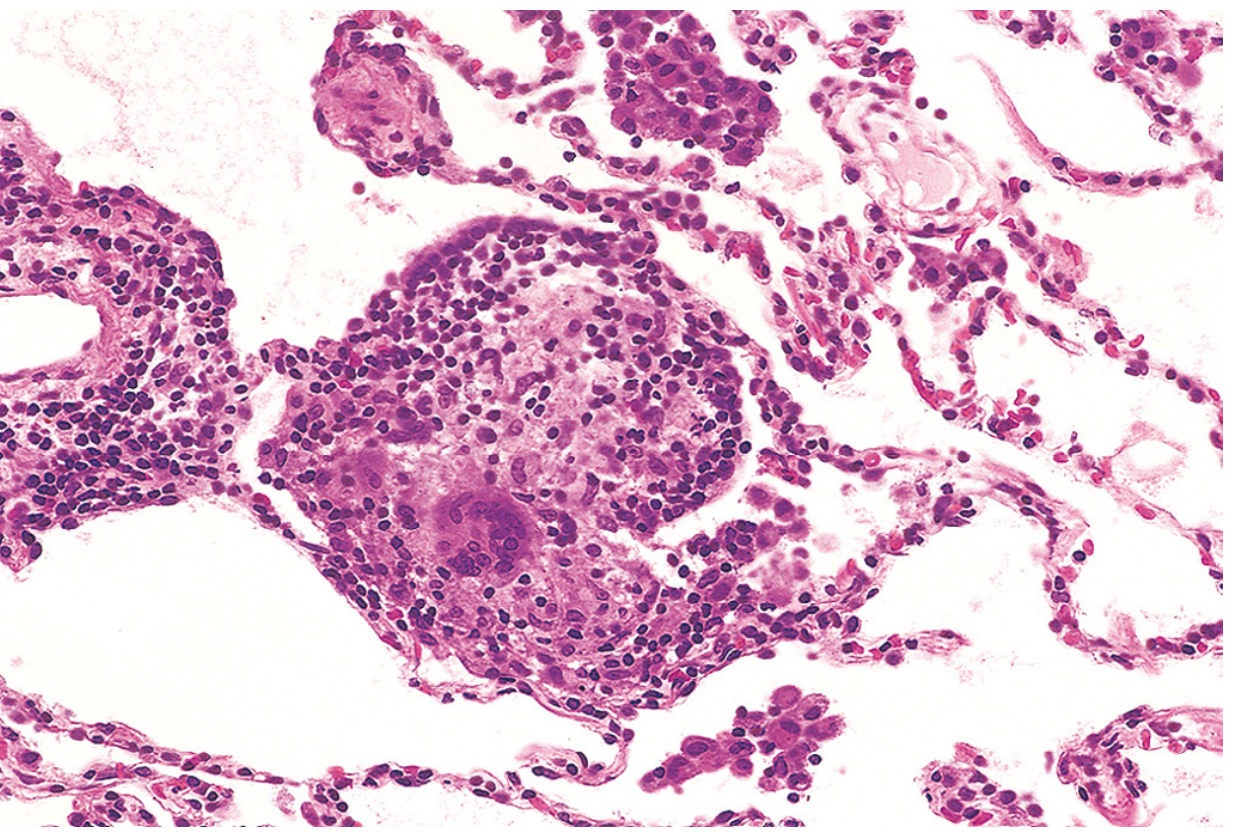
Histopathology
The classic triad on biopsy:
- Lymphocytic interstitial pneumonitis (lymphocytes, plasma cells, macrophages - eosinophils rare)
- Non-necrotizing granulomas (loosely formed, unlike the well-formed granulomas of sarcoidosis)
- Bronchiolocentric distribution
Chronic fibrotic HP may show:
- Bridging fibrosis between perilobular and peribronchiolar areas
- UIP-like pattern with honeycombing
- Organizing pneumonia and constrictive bronchiolitis
Cholesterol clefts in the interstitium are common but nonspecific. Granulomas in HP rarely hyalinize and can resolve after antigen removal.
Epidemiology
- Prevalence increases with age (0.95/100,000 in children ages 0-9 vs. 11.2/100,000 in adults >65)
- HP mortality rates rose from 0.1 to 0.7 per 1,000,000 between 1988 and 2016 (5.6% average annual increase)
- Higher rates in men and farming states of the Midwestern United States
(Murray & Nadel's)
Diagnosis
No single test confirms HP. Diagnosis requires integration of three domains in a multidisciplinary discussion (MDD):
| Domain | Key Findings |
|---|---|
| Exposure history | Detailed occupational, avocational, residential history; pet birds and moldy basements are commonly missed |
| Radiology (HRCT) | Ground-glass opacities, centrilobular nodules, mosaic attenuation, air trapping; UIP pattern in fibrotic HP |
| BAL | Lymphocytosis (CD4+/CD8+ both elevated); helps distinguish from other ILDs |
| Serum precipitins/IgG | Supports antigen identification but positive test ≠ causation |
| Lung biopsy | Surgical or transbronchial; used when diagnosis uncertain after non-invasive workup |
BAL lymphocytosis is also seen in sarcoidosis, nonspecific interstitial pneumonitis, radiation pneumonitis, and cryptogenic organizing pneumonia, so clinical context is essential.
Drug-Induced Pneumonitis
Important drugs and mechanisms:
- Bleomycin - free radical oxygen species; interstitial/ground-glass changes, worse in lower lobes. Dose-limiting; DLCO is a sensitive monitor (stop if DLCO falls ≥25% from baseline)
- Methotrexate, gemcitabine, irinotecan, fludarabine - idiosyncratic, not dose-related
- Checkpoint inhibitors (anti-PD-1/PD-L1), EGFR inhibitors (cetuximab, afatinib), ALK inhibitors (crizotinib) - potentially life-threatening; often require permanent drug discontinuation
- Amiodarone - chronic interstitial infiltrates
- Brentuximab vedotin, fam-trastuzumab deruxtecan - antibody-drug conjugates with significant pulmonary toxicity
Onset can be rapid. Prompt glucocorticoids are important once infection is excluded. Severe pneumonitis = permanent drug discontinuation.
(Harrison's Principles of Internal Medicine 22E)
Radiation Pneumonitis
- Occurs weeks to months after thoracic radiotherapy
- Presents with cough, dyspnea, low-grade fever
- Imaging shows ground-glass opacity or consolidation conforming to the radiation field
- BAL shows lymphocytosis
- Generally glucocorticoid-responsive
Management
Hypersensitivity Pneumonitis
- Antigen avoidance - cornerstone of treatment; most important intervention. May require job change or relocation in severe cases
- Corticosteroids - prednisone 0.5-1 mg/kg/day for 1-2 weeks (acute) or 4-8 weeks (subacute/chronic), then gradual taper to ~10 mg/day maintenance
- Antifibrotic therapy - considered in fibrotic HP (nintedanib has evidence in progressive fibrotic ILD)
- Lung transplantation - for end-stage fibrotic disease
Drug-Induced / Radiation Pneumonitis
- Prednisone 1 mg/kg for acute symptoms, slow taper over months
- Adjuncts: antibiotics (if superinfection), bronchodilators, oxygen, diuretics
- Refractory cases: azathioprine or cyclosporine
- No effective therapy for established pulmonary fibrosis - supportive only
Key Points to Remember
- Early recognition prevents progression to irreversible fibrosis
- Always ask specifically about pet birds and moldy environments - easily missed
- Granulomas in HP are loosely formed and non-necrotizing - unlike sarcoidosis (well-formed) or TB (caseating)
- Fibrotic HP carries a significantly higher mortality than nonfibrotic HP
- A negative antigen history does not rule out HP
- Drug-induced pneumonitis from checkpoint inhibitors is increasingly common with the rise of cancer immunotherapy
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Murray & Nadel's Textbook of Respiratory Medicine; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.