Pancreatic protocol cr
Reading File
Finding Sources
Finding Sources
Searching the Web
pancreatic protocol CT scan phases technique radiology
Reading File
Reading File
Loading Image
Here is a complete overview of the Pancreatic Protocol CT.
Pancreatic Protocol CT
What Is It?
Pancreatic protocol CT (also called dedicated pancreatic CT or multiphasic pancreatic CT) is a specialized multi-phase CT technique optimized to detect and characterize pancreatic pathology - especially pancreatic ductal adenocarcinoma (PDAC), neuroendocrine tumors (NETs), cystic lesions, and pancreatitis. It differs from a routine abdominal CT in its timing, slice thickness, and oral contrast selection.
Indications
| Indication | Preferred Phases |
|---|---|
| Suspected PDAC / pancreatic mass | Pancreatic (late arterial) + portal venous |
| Neuroendocrine tumor | Arterial + portal venous |
| Cystic pancreatic lesion | Pancreatic + portal venous |
| Acute pancreatitis (severity, necrosis) | Portal venous (±arterial if pseudoaneurysm suspected) |
| Chronic pancreatitis / calcifications | Non-contrast + portal venous |
Technique Overview
Patient Preparation
- Position: Supine, arms elevated above head
- Oral contrast: Neutral contrast (water), not positive (barium/iodine-based). Approximately 800 mL water 20-30 min before scan - distends the stomach and duodenum to define the duodenal loop without obscuring vascular enhancement
- Breath-hold: Required for all phases
Scan Parameters
- Tube voltage: ≤120 kVp
- Slice thickness: ≤1 mm (thin slices, typically 0.625 mm), interval ≤0.5 mm
- FOV: ~350 mm, adjusted for patient size
- Reconstruction: Soft tissue algorithm; 3D reconstructions as needed
- Scan extent: Mid-diaphragm to iliac crest for arterial/pancreatic phase; above diaphragm to iliac crest for venous phase (to capture hepatic metastases)
IV Contrast
- Volume: 70-120 mL (1 mL/kg) with 30-40 mL saline chaser
- Injection rate: 3-5 mL/s (minimum 22G IV; 18G preferred)
- Timing: Bolus tracking or test bolus technique using the abdominal aorta as the reference
Phases of Acquisition
1. Non-Contrast Phase (optional but recommended)
- Identifies calcifications (chronic pancreatitis), hyperdense lesions, baseline density
- Establishes baseline Hounsfield units for enhancement analysis
- Bailey and Love: "An initial unenhanced CT scan is essential to determine the presence of calcification within the pancreas and gallbladder."
2. Pancreatic Phase (Late Arterial Phase)
- Timing: ~35-45 seconds after contrast injection (or 15-20 sec after bolus trigger)
- Also called the pancreatic parenchymal phase
- Maximum parenchymal enhancement of the pancreas occurs here
- Provides maximum contrast difference between the normally enhancing parenchyma and hypoenhancing PDAC - best phase to detect PDAC
- Best phase for evaluating tumor-artery relationships (SMA, celiac, hepatic artery) and identifying aberrant arterial anatomy
- The arterial opacification in this phase also limits the need for a separate dedicated arterial phase in most cases
3. Portal Venous Phase
- Timing: ~60-70 seconds after injection
- Best for evaluating hepatic metastases (most liver mets are hypovascular and best seen here)
- Assesses variant venous anatomy and tumor involvement of the portal vein, SMV, and splenic vein (abutment, encasement, thrombosis)
- Standard phase for assessing venous thrombosis
4. Delayed / Hepatic Phase (optional)
- Timing: ~180 seconds
- May be added for characterization of indeterminate liver lesions
- Some institutions include for assessing biliary anatomy or certain cystic lesions
Why These Specific Phases?
PDAC is typically desmoplastic and hypovascular - it enhances less than the surrounding normal pancreatic parenchyma. The pancreatic phase maximizes the attenuation difference (tumor-to-pancreas contrast), making even small tumors (1-2 cm) visible. By contrast, NETs are hypervascular and light up brightly in the arterial phase.
Sabiston Textbook of Surgery: "The late-arterial phase is usually the best phase to identify PDAC because the timing provides the maximum contrast difference between normally enhancing pancreatic parenchyma and the PDAC, which is generally hypoenhancing. In addition, this is the best phase for analyzing the tumor-artery relationships and noting the presence of any aberrant arterial anatomy. The portal-venous phase is valuable for assessing variant venous anatomy and tumor-vessel abutment or encasement."
What the Scan Evaluates (for PDAC)
- Tumor location - head (most common), body, or tail
- Resectability - key surgical decision:
- Arterial involvement: SMA, celiac axis, hepatic artery (assessed on pancreatic phase)
- Venous involvement: portal vein, SMV (assessed on venous phase)
- Distant metastases - liver (venous phase), peritoneum, lung (include chest CT)
- Biliary/pancreatic duct dilation - double duct sign in periampullary tumors
- Nodal involvement
- Vascular anatomy variants - critical for surgical planning (e.g., replaced right hepatic artery from SMA)
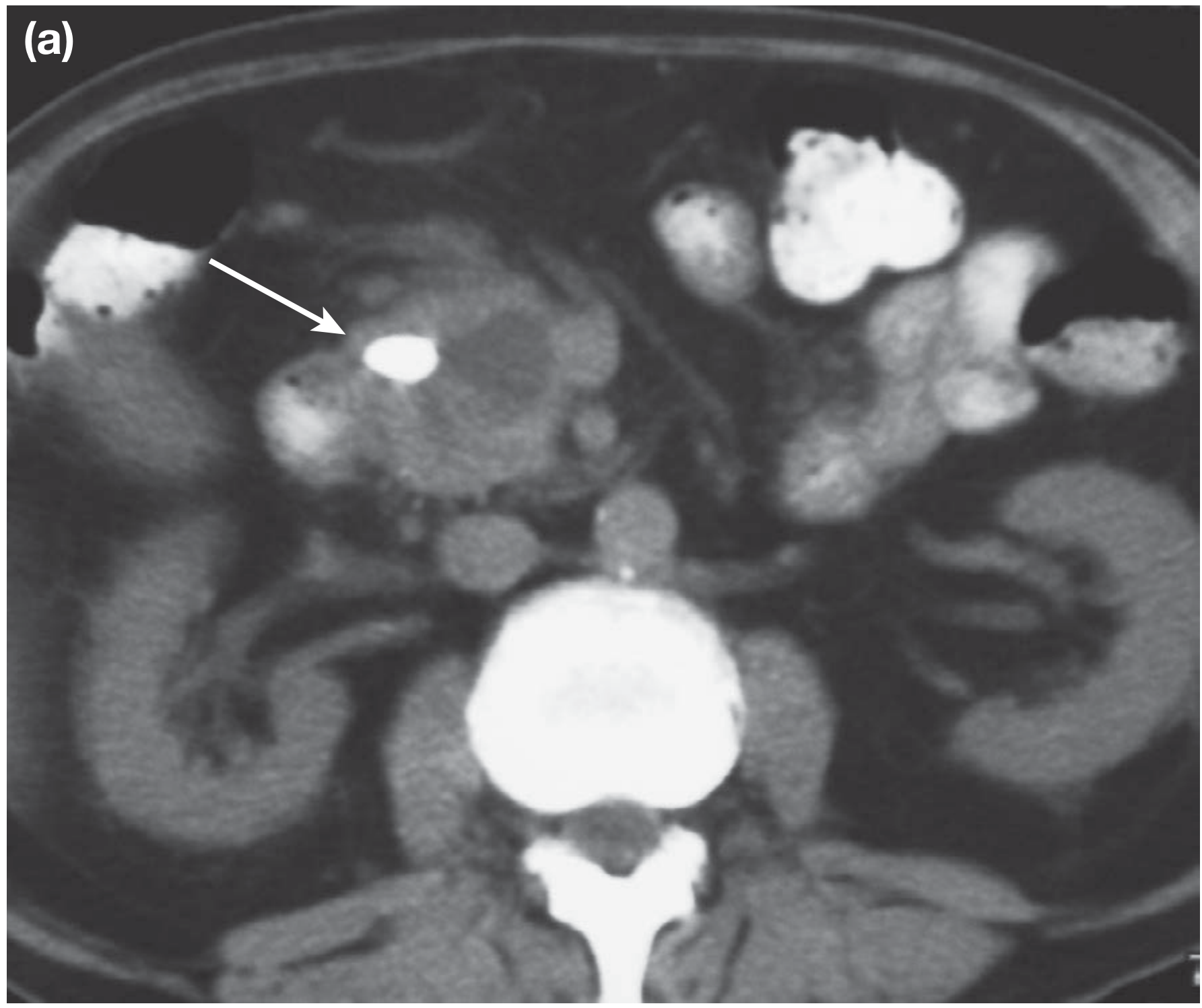
Unenhanced pancreatic CT showing calcification (arrow) in the head of the pancreas - Bailey and Love's Surgery
Limitations and Additional Imaging
- If indeterminate liver lesions or suspicious nodal involvement exist on CT, add MRI (better soft tissue characterization) or PET-CT (metabolic activity)
- CT should always be done before any invasive procedure (ERCP, EUS-FNA). ERCP-related pancreatitis causes peripancreatic inflammation that obscures the tumor-vessel relationship and degrades staging accuracy
- For vascular planning, CT angiography reconstructions from the same dataset are often produced
Summary Table
| Phase | Timing | Key Purpose |
|---|---|---|
| Non-contrast | Before injection | Calcifications, baseline |
| Pancreatic (late arterial) | ~35-45 sec | PDAC detection, arterial anatomy |
| Portal venous | ~60-70 sec | Venous anatomy, liver mets |
| Delayed (optional) | ~180 sec | Indeterminate liver lesions |
Sources:
- Sabiston Textbook of Surgery - Diagnostic Studies (PDAC chapter)
- Bailey and Love's Short Practice of Surgery, 28th ed. - Computed Tomography of the Pancreas
- Radiopaedia: CT Pancreas Protocol
- Applied Radiology: Imaging of the Pancreas
This is a shared conversation. Sign in to Orris to start your own chat.