Stroke
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the core content needed. Let me compile the comprehensive overview.
Stroke - Overview for Medical Students
Definition
Stroke is the clinical syndrome of acute-onset focal neurologic deficits lasting >24 hours resulting from either vessel occlusion or vessel rupture in the brain. A deficit resolving within 24 hours (with no infarction on imaging) is termed a Transient Ischemic Attack (TIA).
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1155
Types of Stroke
Stroke is classified into two major categories:
1. Ischemic Stroke (~80% of all strokes)
Caused by occlusion of a cerebral vessel, depriving brain tissue of glucose and oxygen.
2. Hemorrhagic Stroke (~20%)
Caused by rupture of a vessel, producing blood in or around the brain.
Ischemic Stroke - Subtypes (TOAST Classification)
The TOAST (Trial of Org 10172 in Acute Stroke Treatment) classification is the standard etiological framework:
| Subtype | Mechanism | Typical Features |
|---|---|---|
| Large artery atherosclerosis | Artery-to-artery emboli or in situ thrombosis; significant stenosis (≥50%) of extracranial/intracranial large vessels | Cortical deficits, carotid bruits, prior TIA in same territory |
| Cardioembolic | Embolus from cardiac sources - AF, LV thrombus, valvular disease, dilated cardiomyopathy | Sudden maximal deficit, multiple territory involvement, hemorrhagic transformation |
| Small artery occlusion (Lacunar) | Lipohyalinosis/microatheroma of small penetrating arteries (basal ganglia, thalamus, internal capsule, pons, corona radiata) | Infarct ≤2 cm on MRI, classic lacunar syndromes (see below), no cortical features |
| Other determined etiology | Dissection, vasculitis, coagulopathy, CADASIL, Fabry disease | Younger patients especially |
| Cryptogenic (undetermined) | No cause identified after full workup | ~25-35% of all strokes |
- Fuster and Hurst's The Heart, 15th Edition, p. 805
- Harrison's Principles of Internal Medicine 22E, p. 3487
Pathophysiology of Ischemic Stroke
The Three Core Mechanisms
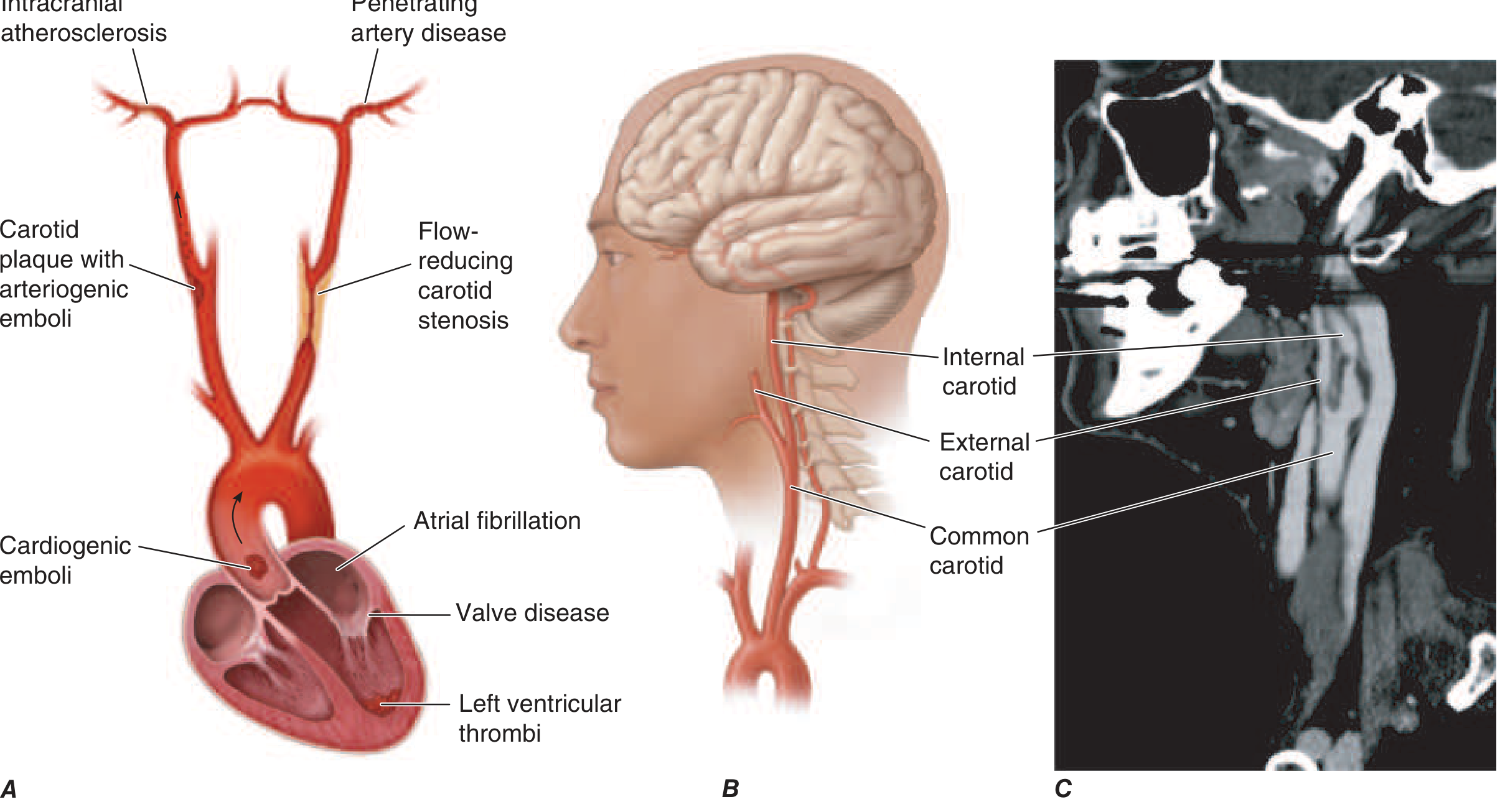
Figure: The three major mechanisms of ischemic stroke - embolism (cardiogenic or artery-to-artery), in situ thrombosis of small penetrating vessels, and hypoperfusion from flow-limiting stenosis. (Harrison's 22E, Fig. 438-4)
- Embolism - from cardiac sources (AF most important) or artery-to-artery (atherosclerotic plaque rupture), occluding large intracranial vessels
- In situ thrombosis - lipohyalinosis of small penetrating arteries producing lacunar infarcts
- Hypoperfusion - flow-limiting stenosis causing watershed (boundary zone) ischemia
Ischemic Penumbra (The Key Concept)
-
After vessel occlusion, some neurons die immediately - this is the infarct core
-
Surrounding it is the ischemic penumbra: a zone of functionally impaired but structurally viable neurons
-
The penumbra is potentially salvageable and is the target of reperfusion therapies (tPA, thrombectomy)
-
Without reperfusion, the penumbra is progressively recruited into the infarct core
-
Collateral circulation (circle of Willis, leptomeningeal collaterals) influences core size and penumbral survival
-
Fuster and Hurst's The Heart, 15th Edition, p. 806
Cellular Mechanism of Ischemic Injury
- Loss of glucose/oxygen → failure of Na-K ATPase
- Cytotoxic edema (water enters cells)
- Glutamate excitotoxicity → Ca²⁺ influx → mitochondrial damage
- Free radical formation, lipid peroxidation, proteolysis
- Neuronal apoptosis and necrosis
Lacunar Strokes - Classic Syndromes
Small penetrating artery occlusions produce stereotyped syndromes (no cortical features like aphasia, neglect, or visual field defects):
| Syndrome | Lesion Site |
|---|---|
| Pure motor hemiparesis | Posterior internal capsule / pons |
| Pure sensory stroke | Thalamus (VPL nucleus) |
| Sensorimotor stroke | Thalamus + adjacent internal capsule |
| Ataxic hemiparesis | Pons / internal capsule |
| Dysarthria-clumsy hand | Pons / genu of internal capsule |
- Fuster and Hurst's The Heart, 15th Edition, p. 805
Hemorrhagic Stroke - Subtypes
Intracerebral Hemorrhage (ICH)
- Deep/ganglionic hemorrhage (basal ganglia, thalamus, internal capsule, pons): caused by hypertensive microangiopathy - chronic hypertension causes lipohyalinosis and Charcot-Bouchard microaneurysms in small penetrating arteries
- Lobar hemorrhage: most commonly due to cerebral amyloid angiopathy (CAA) - beta-amyloid deposition in vessel walls, particularly in elderly patients
- ICH may extend into the ventricular system (intraventricular hemorrhage)
Subarachnoid Hemorrhage (SAH)
-
~1% of all strokes
-
Most common cause: rupture of an intracranial saccular aneurysm (berry aneurysm), typically at arterial bifurcations
-
Classic presentation: sudden-onset "thunderclap headache" (worst headache of life)
-
Less common: AVM rupture, RCVS
-
Fuster and Hurst's The Heart, 15th Edition, p. 806
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1155
Clinical Features
Anterior Circulation (Carotid Territory - MCA/ACA)
- MCA territory: contralateral hemiplegia (face and arm > leg), hemisensory loss, homonymous hemianopia
- Dominant hemisphere (usually left): aphasia (Broca's = expressive; Wernicke's = receptive)
- Non-dominant hemisphere: neglect, anosognosia, constructional apraxia
- ACA territory: contralateral leg > arm weakness, frontal lobe signs, abulia, urinary incontinence
Posterior Circulation (Vertebrobasilar Territory)
- PICA (lateral medullary / Wallenberg syndrome): ipsilateral facial pain/numbness, contralateral body pain/temperature loss, Horner's, dysphagia, ataxia - "crossed" sensory deficits
- Basilar artery occlusion: bilateral limb weakness, coma, locked-in syndrome (catastrophic)
- PCA territory: contralateral homonymous hemianopia (macular sparing common)
FAST Acronym (Screening)
- Face drooping (asymmetric smile)
- Arm weakness (one arm drifts down)
- Speech difficulty (slurred, wrong words, mute)
- Time to call emergency services
Key Distinguishing Features: Ischemic vs Hemorrhagic
| Feature | Ischemic | Hemorrhagic (ICH) |
|---|---|---|
| Onset | Sudden, maximal at onset | Sudden, may progress over minutes |
| Headache | Uncommon | Common, severe |
| Vomiting | Uncommon | Common |
| Loss of consciousness | Uncommon (except basilar) | More frequent |
| Blood pressure | Variable | Often severely elevated |
| CT finding | Hypodense (after hours) | Hyperdense (blood, immediate) |
Risk Factors
Modifiable: hypertension (most important), atrial fibrillation, diabetes, smoking, hyperlipidemia, obesity, physical inactivity, excessive alcohol, cocaine/amphetamines
Non-modifiable: age, male sex, prior stroke/TIA, race (African American, Asian higher risk for lacunar), family history
TIA - The "Warning Stroke"
-
Defined as focal neurologic symptoms lasting <24 hours with no infarction on imaging
-
Most TIAs last <1 hour
-
10-15% risk of stroke in the first 3 months, with majority occurring within 2 days
-
Risk stratified by ABCD2 score: Age, Blood pressure, Clinical features, Duration, Diabetes
-
Causes are identical to ischemic stroke; urgent evaluation is required
-
Harrison's Principles of Internal Medicine 22E, p. 3488
Causes of Ischemic Stroke (Common vs Uncommon)
Common:
- Thrombosis: lacunar, large-vessel, dehydration
- Embolic: artery-to-artery (carotid bifurcation, aortic arch), cardioembolic (AF, mural thrombus, MI, valvular disease, paradoxical embolus via PFO)
Uncommon/Special:
-
Hypercoagulable states (Protein C/S deficiency, antiphospholipid syndrome, factor V Leiden)
-
Sickle cell disease, polycythemia vera
-
Vasculitis (primary CNS or systemic)
-
Dissection (ICA or vertebral - most common cause of stroke in young adults <60)
-
CADASIL (Notch-3 gene mutation - hereditary small-vessel disease)
-
COVID-19-associated coagulopathy
-
Oral contraceptives, stimulant drugs
-
Harrison's Principles of Internal Medicine 22E, p. 3487
Key Exam Points
- Ischemic stroke = ~80%, hemorrhagic = ~20% of all strokes
- TOAST classification: large artery, cardioembolic, lacunar (small vessel), other determined, cryptogenic
- Penumbra = the salvageable zone around the infarct core - the rationale for thrombolysis and thrombectomy
- Lacunar strokes: five classic syndromes, no cortical features, small penetrating artery occlusion
- Deep ICH = hypertension; lobar ICH = cerebral amyloid angiopathy
- SAH = thunderclap headache + meningism = berry aneurysm rupture until proven otherwise
- Atrial fibrillation is the single most important cardiac cause of embolic stroke
- Arterial dissection = most common cause of stroke in patients under 60
- CADASIL = autosomal dominant, Notch-3 mutation, small vessel strokes + dementia + migraine with aura
- TIA is a medical emergency - ABCD2 score, 10-15% stroke risk within 3 months
This is a shared conversation. Sign in to Orris to start your own chat.