What is Pathophysiology of nipple retraction and skin dimpling puckering
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Pathophysiology of Nipple Retraction and Skin Dimpling / Puckering
To understand these signs, you must first understand the relevant anatomy.
Anatomical Basis
The breast is supported by Cooper's suspensory ligaments - fibrous bands running from the deep fascia (overlying pectoralis major) through the breast parenchyma to fuse with the dermis. Because these ligaments are anchored directly into the skin, any process that shortens or distorts them will produce visible surface changes.
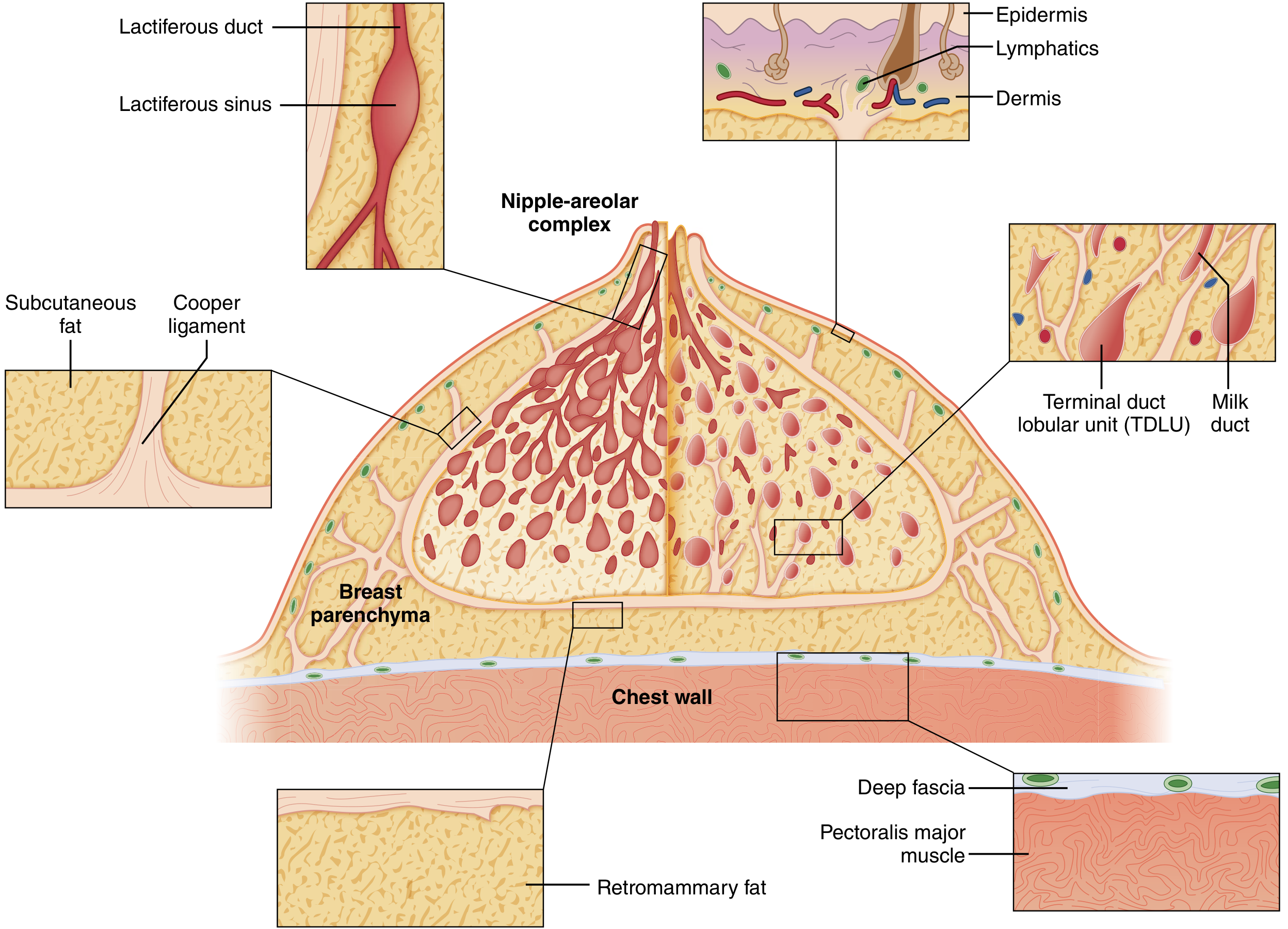
There are 15-20 major lactiferous ducts converging at the nipple. The nipple protrudes because these ducts elongate during puberty (ages 14-16). Failure of elongation, or later shortening, determines nipple position.
1. Nipple Retraction
There are two distinct mechanisms - congenital and acquired.
A. Congenital Nipple Inversion
- During puberty, the major milk ducts normally elongate, pushing the nipple forward (telarche occurs ~1 year before menarche).
- If the ducts fail to elongate, the nipple does not protrude - this is true nipple inversion.
- It does not predispose to breast cancer.
- It can interfere with breastfeeding and predispose to infection from retained debris.
B. Acquired Nipple Retraction - the two key causes:
i. Periductal Mastitis / Duct Ectasia (most common cause of longstanding retraction)
The sequence is:
- Duct ectasia: Major milk ducts dilate (>3 mm on ultrasound) and fill with debris - an abnormal involutional process.
- The stagnant secretions (containing chemically irritating fatty acids and lipoid material) leak through the thinned duct wall into the periductal tissue.
- This triggers periductal inflammation - predominantly plasma cell infiltrate (hence the old name "plasma cell mastitis").
- Repeated inflammatory episodes cause periductal fibrosis.
- The fibrous scarring shortens and tethers the major ducts, pulling the nipple inward - producing retraction.
- In periductal mastitis, the retraction pattern is characteristically transverse slit-like or "fish-mouth" in shape.

ii. Carcinoma
- A malignant tumour invades and infiltrates the periductal stroma and major ducts.
- The desmoplastic (fibrotic) reaction around the tumour shortens the duct system.
- The ducts tether and shorten the nipple inward - circumferential retraction (in contrast to the slit-like pattern of periductal mastitis).
- Recent-onset nipple retraction is always worrisome and must be assumed to indicate carcinoma until proven otherwise.
Key distinction: Slit-like retraction = periductal mastitis. Circumferential retraction = carcinoma.
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 945
- Schwartz's Principles of Surgery, 11th Ed., p. 579
2. Skin Dimpling / Puckering
Mechanism
Skin dimpling occurs when Cooper's ligaments are infiltrated, shortened, or tethered by tumour or fibrosis:
- A breast carcinoma invades the fibrous interlobular stroma.
- This induces a desmoplastic response - reactive fibrosis in and around the tumour.
- Cooper's ligaments, anchored to the dermis at one end and the deep fascia at the other, are caught up in this fibrous reaction.
- The shortened/tethered ligaments pull the overlying skin inward toward the tumour mass, producing a focal depression or dimple in the skin surface.
- The result is a visible puckering or dimpling over or near the tumour site.
As stated in Sabiston's Textbook of Surgery: "edema of the breast or infiltration of Cooper ligaments by cancer can produce dimpling of the otherwise smooth surface of the breast"
- Sabiston Textbook of Surgery, p. 1369
3. Peau d'Orange (a Related Sign)
Peau d'orange ("orange peel skin") is a more advanced manifestation and has a different mechanism from simple dimpling:
- Tumour cells invade and obstruct the subdermal lymphatic channels of the breast, or obstruct axillary lymph nodes.
- Lymphatic obstruction causes interstitial fluid accumulation (lymphoedema) in the dermis.
- The skin swells uniformly, but the hair follicles and sweat gland openings remain tethered by Cooper's ligaments at the dermis.
- These fixed points create characteristic small pits in the swollen skin, producing the "orange peel" texture.
- It is a sign of locally advanced breast cancer (Stage IIIB in inflammatory breast carcinoma).
As described in Robbins & Kumar Basic Pathology: "Infiltration and obstruction of superficial lymphatics by breast cancer may cause edema of the overlying skin; the characteristic finely pitted appearance of the skin of the affected breast is called peau d'orange (orange peel)."
- Robbins & Kumar Basic Pathology, p. 80
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 954
Summary Table
| Sign | Core Mechanism | Key Structures Involved | Main Cause |
|---|---|---|---|
| Nipple inversion (congenital) | Failure of duct elongation at puberty | Major lactiferous ducts | Developmental |
| Nipple retraction (slit-like) | Periductal fibrosis shortens ducts | Major ducts, periductal stroma | Periductal mastitis / duct ectasia |
| Nipple retraction (circumferential) | Desmoplastic fibrosis shortens ducts | Major ducts | Carcinoma |
| Skin dimpling / puckering | Cooper's ligaments tethered by tumour fibrosis | Cooper's suspensory ligaments, dermis | Carcinoma |
| Peau d'orange | Lymphatic obstruction + skin oedema with anchored follicles | Subdermal lymphatics, dermis | Advanced carcinoma / inflammatory BC |
The unifying theme is fibrosis and tethering - whether of the ducts (causing nipple retraction) or of the suspensory ligaments (causing skin dimpling), abnormal fibrous tissue mechanically distorts the flexible breast architecture into fixed, retracted positions.
This is a shared conversation. Sign in to Orris to start your own chat.